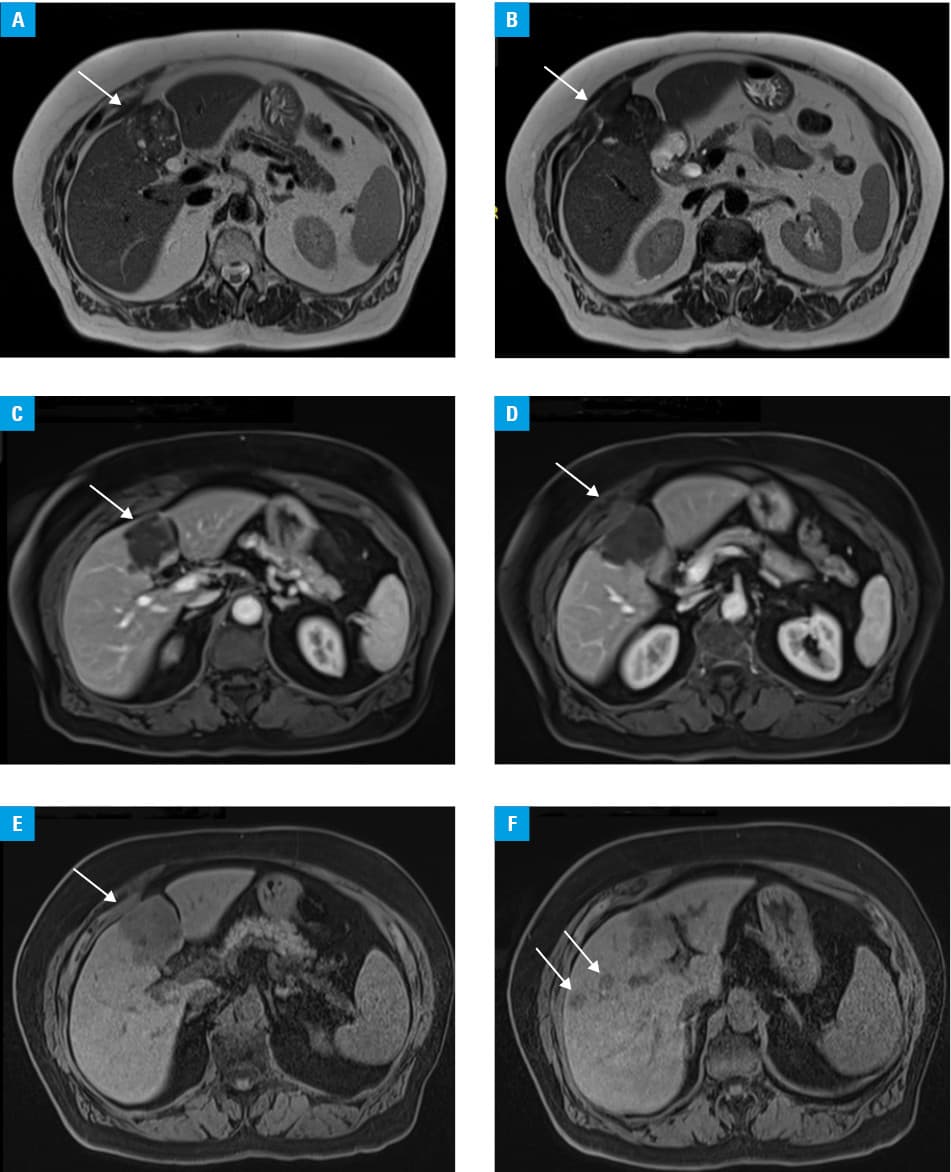
A 77‑year‑old woman with a history of hypertension and diabetes presented with nausea and right upper quadrant abdominal pain radiating to the back. Abdominal ultrasonography showed a liver lesion suggestive of a tumor. The patient was admitted to an oncology department, where abdominal computed tomography identified an irregular, nodular lesion located in the gallbladder and extending into segments 4 and 5 of the liver. The lesion measured 60 mm × 72 mm × 58 mm and adhered to the abdominal wall and directly to the duodenum, with possible wall infiltration. Additionally, smaller lesions indicative of metastases were observed in segments 5 and 8. Core needle biopsy was performed, and histologic examination showed fragments of necrotic tissues. The patient was transferred to a surgery department where core needle biopsy was repeated, showing a fragment of an echinococcal cyst. the patient was referred to an outpatient clinic of infectious diseases for further evaluation. Blood tests were conducted, and anti-Echinococcus spp. antibodies were detected in enzyme‑linked immunosorbent assay, while Western blot test was positive for anti-Echinococcus multilocularis antibodies. Magnetic resonance imaging (MRI) of the abdomen showed 2 lesions in segment 5 of the liver. The first measured 15 mm × 12 mm, and the second, 12.5 mm in diameter, both exhibiting characteristics of liver cyst membranes. In segment 4 of the liver, a polycyclic lesion measuring 52 mm × 65 mm × 55 mm and multiple minor cystic calcifications were identified. The MRI report primarily suggested alveolar echinococcosis. The patient declined any further surgical procedures. Consequently, a treatment with albendazole 400 mg twice daily was initiated, and the patient has remained under regular follow‑up at the outpatient clinic of infectious diseases. Follow‑up MRIs conducted 4 and 12 months postdiagnosis showed that the liver lesions remained stable (Figure 1A–1F).
E. multilocularis is a causative agent of alveolar echinococcosis, a rare zoonotic disease that mainly affects the liver, and is transmitted by ingestion of tapeworm eggs with forest fruits contaminated with fox feces. Our patient was a farmer, which put her at a risk of this infection.
According to the European Centre for Disease Prevention and Control data, in 2023, the notification rate of echinococcosis (alveolar and cystic) was 0.21 per 100 000 individuals, marking an 8.4% increase in comparison with 2022. It remains a diagnostic and therapeutic challenge due to the prolonged asymptomatic period,1 appearance resembling malignant tumors, and invasion of surrounding tissues. The course of the disease is always severe and, if left untreated, can be fatal.2 Therefore, early diagnosis of alveolar echinococcosis is crucial, as it allows for a radical surgical intervention that can potentially lead to complete recovery. Delayed diagnosis may limit treatment options to liver transplant or palliative care.3 It should be emphasized, however, that in patients with suspected alveolar echinococcosis, needle biopsy carries a high risk of intra‑abdominal dissemination of the infection and should not be performed routinely. In this case, when the patient was initially diagnosed with a suspected liver neoplasm, she showed no signs of echinococcosis.
- Kern P, Menezes da Silva A, Akhan O, et al. The echinococcoses: diagnosis, clinical management and burden of disease. Adv Parasitol. 2017: 96: 259‑369. | Crossref
- Respondek A, Baryła M, Popławska‑Ferenc A, et al. Echinococcosis of the liver in Poland ‑ review of the literature and our own clinical material. Clin Exp Hepatol. 2024; 10: 150‑158. | Crossref
- Dulger AC, Esen R, Begenik H, et al. Alveolar echinococcosis of the liver: a single center experience. Pol Arch Med Wewn. 2012; 122: 133‑138. | Crossref
ARTICLE INFORMATION