Direct oral anticoagulants vs vitamin K antagonists in patients with single- or double-positive antiphospholipid syndrome: a systematic review and meta-analysis
Key words: anticoagulants, antiphospholipid syndrome, hemorrhage, meta-analysis, thrombosis

 CC BY 4.0
CC BY 4.0
Direct oral anticoagulants vs vitamin K antagonists in patients with single- or double-positive antiphospholipid syndrome: a systematic review and meta-analysis
Introduction: Antiphospholipid syndrome (APS) is a heterogeneous disease where the presence of antiphospholipid antibodies (aPLs) results in blood clot formation. Compared with patients with a triple‑positive antibody profile, the optimal anticoagulant strategy in individuals with a single- or double‑positive APS is still debated due to their different risks of recurrent thrombosis.
Objectives: This systematic review and meta‑analysis aimed to investigate the efficacy and safety of direct oral anticoagulants (DOACs) and vitamin K antagonists (VKAs) for treating single- or double‑positive APS.
Patients and methods: The Medline and EMBASE databases were searched until September 2024 for randomized clinical trials (RCTs) and observational studies that included patients with APS positive to a single or double aPL test. Pooled risk ratios (RRs) and 95% CIs were estimated with a random‑effects model.
Results: Three RCTs and 7 observational studies were included in the efficacy analysis, totaling 439 patients treated with DOACs and 481 with VKAs. No difference in the risk of thrombosis recurrence was observed between the 2 treatments (RR, 0.78; 95% CI, 0.36–1.69), despite an opposite trend in RCTs (RR, 2.54; 95% CI, 0.61–10.59) as compared with the observational studies (RR, 0.6; 95% CI, 0.25–1.39). Two RCTs and 6 observational studies reported data on bleeding, totaling 287 patients in the DOAC and 367 in the VKA group. No difference in the risk of major bleeding / clinically relevant nonmajor bleeding between treatments was detected (RR, 0.78; 95% CI, 0.3–2.05).
Conclusions: DOACs could be an effective and safe alternative to VKAs for managing single- or double‑positive APS.
What's new?
While vitamin K antagonists (VKAs) are an established anticoagulation therapy for patients with triple‑positive antiphospholipid syndrome, the optimal strategy for single- or double‑positive patients is still debated. This meta‑analysis suggests that direct oral anticoagulants may offer comparable effectiveness and safety to VKAs in these patients, who typically have a lower risk of thrombotic recurrence than triple‑positive individuals. However, more longitudinal studies, possibly stratified by the antibody profile, are needed to confirm this finding.
Introduction
Antiphospholipid syndrome (APS) is an autoimmune systemic disease characterized by a hypercoagulable state due to the presence of persistent antiphospholipid antibodies (aPLs), which clinically manifests with venous and / or arterial thrombotic events and / or pregnancy morbidity.1 aPLs promote the activation of inflammatory and endothelial cells by binding to anionic phospholipid‑binding glycoprotein (GP), particularly β2‑GPI, resulting in blood clot formation.2 Laboratory tests routinely carried out to detect aPL include lupus anticoagulant (LAC), a functional coagulation assay, and solid‑phase enzyme‑linked immunosorbent assays for immunoglobulin G (IgG)/IgM anticardiolipin and IgG/IgM anti–β2‑GPI antibodies.3 Due to high heterogeneity of clinical and laboratory presentations, a diagnosis is often challenging and, not rarely, delayed or missed.4
Once the APS diagnosis is established, prompt anticoagulation therapy must be started to reduce the risk of thrombotic events. The recommended anticoagulation strategy involves vitamin K antagonists (VKAs), especially in high‑risk patients with triple‑positive aPL tests (LAC, anticardiolipin, and anti–β2‑GPI antibodies), whereas direct oral anticoagulants (DOACs) are not recommended.1,5-7 Indeed, Pengo et al8 in the TRAP trial (Rivaroxaban in Thrombotic Antiphospholipid Syndrome) showed that patients with triple‑positive tests experienced a significantly higher risk of thrombotic events when treated with rivaroxaban than VKAs (hazard ratio [HR], 7.4; 95% CI, 1.7–32.9), especially in the arterial bed. Subsequent randomized controlled trials (RCTs)9,10 and meta‑analyses11-14 confirmed this finding.
However, patients with established APS have a heterogeneous risk of recurrence that is related to their aPL profile, with triple positivity conferring the highest risk of recurrences. Risk stratification and appropriate anticoagulation strategy is still a matter of debate in patients with single- or double‑positive aPL tests, since none of the RCTs comparing DOACs vs VKAs available so far was specifically designed to explore the risk of recurrence in these patients.8-10,15 In comparison with VKAs, the potential advantages of DOACs include a rapid onset of action, stable and predictable anticoagulation effects, no need for frequent blood analysis, and a lower risk of major and intracranial bleeding, thus potentially they represent a suitable treatment option for lower‑risk patients.16 Encouragingly, a subanalysis of a 2022 meta‑analysis by Wu et al17 highlighted that, in the patients with a single- or double‑positive aPL profile, the risk of recurrent thrombosis or major bleeding was similar for VKAs and DOACs (risk ratio [RR] for thrombosis, 1.65; 95% CI, 0.72–3.81; RR for bleeding, 1.1; 95% CI, 0.26–4.63). Since then, more studies have been investigating patients with different aPL patterns.
Thus, this updated systematic review and meta‑analysis aimed to evaluate the efficacy and safety of DOACs vs VKAs for secondary thromboprophylaxis in patients with single- or double‑positive APS.
Patients and methods
The review has been registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number, CRD42024586538).
Search strategy and selection criteria
The literature search was performed in the Medline and EMBASE electronic databases from January 1, 2010 (the year of the first DOAC approval by the Food and Drug Administration) to September 30, 2024. The PICO criteria identified to carry out this systematic review and meta‑analysis included: patients with single- or double‑positive APS (population), DOACs (intervention), VKAs (comparison), recurrent thrombosis and major bleeding / clinically relevant nonmajor bleeding (CRNMB) (outcomes). According to the PICO criteria, a consistent search strategy was developed for each database (for details, see Supplementary material, Table S1).
To be suitable, studies had to include adults (age ≥18 years) and report the antibody profile of patients and controls. Single positivity or any combination of the 3 laboratory tests (LAC, IgG/IgM anticardiolipin, or IgG/IgM anti–β2‑GPI antibodies) was accepted, except for triple positivity. Only RCTs, cohort studies, and case‑control studies were included. No language or geographic restrictions were applied.
Based on titles and abstracts, 2 investigators (AG and FB) independently performed the first screening of the identified studies. Then, the second selection based on full‑text evaluation was carried out. Any disagreements between the 2 investigators were resolved by consulting a third investigator (MN). Finally, we manually retrieved the included studies’ reference lists and prior relevant reviews and meta‑analyses for possible additional studies. Concordance between the authors was evaluated by the κ statistic, which measures agreement beyond chance.18
Data extraction and risk of bias assessment
The following data from each included study were extracted and recorded in a standardized data extraction form (Excel spreadsheet) by 2 reviewers (MN and FB): 1) first author’s last name, year of publication, and study design; 2) number of cases and controls and their baseline characteristics (age, sex, duration of follow‑up, time in therapeutic range [TTR] for VKAs treatment); 3) antibody profile (single or double positivity) for patients and controls; 4) clinical outcomes: recurrent thrombosis (if reported classified by vascular bed) and major bleeding/CRNMB. If necessary, the corresponding authors were contacted by email for missing data.
Quality assessment of the eligible studies was performed independently by 2 investigators (SC and EG). To assess the risk of bias in the RCTs, we used the Cochrane risk of bias tool for randomized trials (RoB 2). RoB 2 is structured into 5 domains of bias, focusing on different aspects of trial design, conduct, and reporting. The Newcastle–Ottawa scale (NOS) was utilized to assess the quality of nonrandomized studies. Two different NOS tools, for evaluating cohort studies and case‑control studies, are available; in both, a maximum of 4 stars can be assigned for selection, 2 for comparability, and 3 for exposure (cohort studies) or outcome (case‑control studies) categories, with a total score between 0 and 9. In particular, for comparability, we awarded 1 star to the studies in which the mean or median duration of follow‑up in the 2 treatment groups differed by no more than 20%. For the outcome category, we considered that a study had a sufficient mean or median follow‑up time when in both groups it was at least 12 months. For our purpose, a study awarded with a minimum of 7 stars was considered of high quality.
The third reviewer (MN) was involved when disagreements between the investigators occurred.
Statistical analysis
The pooled risk ratios (RRs) and 95% CIs of the treatment efficacy and safety of DOACs vs VKAs were estimated using a random‑effects model (Mantel–Haenszel). The heterogeneity between studies was explored using the I2 statistic and, according to the Cochrane Handbook for Systematic Reviews of Interventions,19 an I2 of less than 30% suggested mild heterogeneity, 30%–60% moderate heterogeneity, and over 60% substantial heterogeneity. In the presence of moderate‑substantial heterogeneity, we removed 1 study at a time to identify the potential source of heterogeneity. As a sensitivity analysis, we planned on repeating the analysis by including only the studies with similar follow‑up times between treatments. Finally, 2 additional subgroup analyses were carried out based on antibody profile (single positivity only) and site of recurrent thrombosis (venous or arterial).
A 2‑tailed P value below 0.05 was considered significant. The statistical analyses were performed in Cochrane Review Manager version 5.4 (The Cochrane Collaboration, London, United Kingdom).
Publication bias
The publication bias was explored graphically by funnel plots of effect size vs standard error.
Results
Study selection
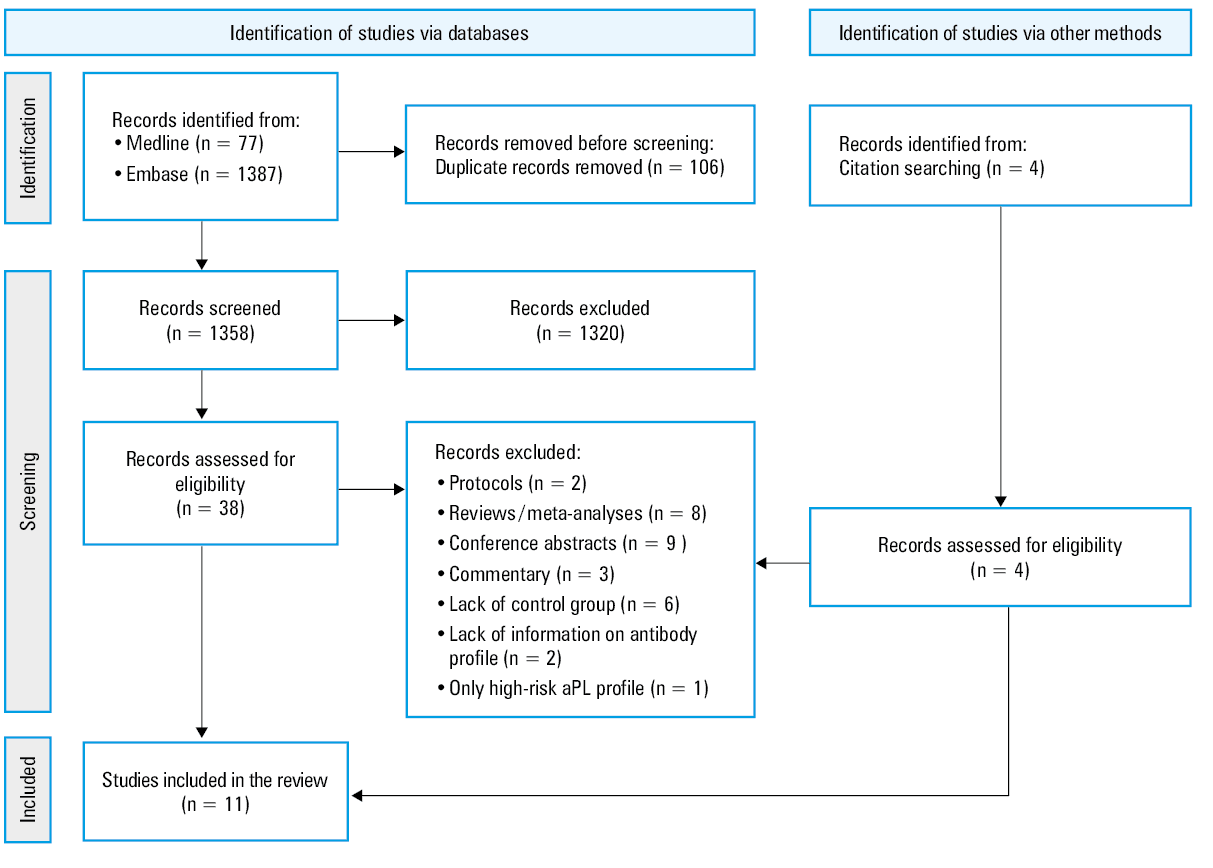
Our search in the electronic databases through EMBASE and Medline identified 1464 records. After removing duplicates, 1358 papers were screened based on their title and abstract, finding 38 studies eligible for full‑text evaluation. The interobserver agreement for the study selection was excellent, with a κ of 0.94. Four more potential studies were identified through a manual retrieval of the references of the selected studies, prior relevant reviews, and meta‑analyses. Of the 42 studies retrieved, 31 were excluded for not meeting the inclusion criteria, and 11 were included for the quantitative results. Of these, 10 studies were included in the main analysis, while 120 was considered only for a subgroup analysis, because suspected duplication with another included study21 based on published data could not be ruled out due to a lack of authors’ response. A detailed PRISMA flowchart of the selection process is shown in Figure 1.
Characteristics of the studies
The main baseline characteristics of the included studies are summarized in Table 1. Of the 11 studies included, 3 were RCTs,9,10,15 7 were retrospective cohort studies,20-25,27 and 1 was a prospective cohort study.26 In the RCTs, the patients included were mainly women at a mean age of 46–50 years. Data were reported stratified for antibody profile in 2 RCTs,9,15 while in the work by Ordi‑Ros et al10 the patients with single and double positivity were considered together. The follow‑up duration ranged between 7 and 35 months.
First author, trial design, and type of DOACa | Age, y, median (IQR)
or mean (SD) | Women, % | Follow‑up, mo, median (IQR) or mean (SD)b | aPL profile (single / double) | Patients treated, n | TTR on VKA treatment, %, median | ||||
DOAC | VKA | DOAC | VKA | DOAC | VKA | DOAC | VKA | |||
a Type of DOAC in the original study
b Mean or median data are provided only when available
c Included only in the subgroup analysis for single‑positive antibody test
Abbreviations: D, double‑positive antiphospholipid syndrome; DOAC, direct oral anticoagulant; IQR, interquartile range; N.R., not reported; S, single‑positive antiphospholipid syndrome; TTR, time in therapeutic range; VKA, vitamin K antagonist; others, see Figure 1 | ||||||||||
Martinelli27; prospective cohort study; rivaroxaban | 46 (16) | 43 (15) | 30 | 33 | 19 (12) | 23 (13) | D
S | 0
7 | 2
6 | N.R. |
Williams22; retrospective cohort study; rivaroxaban, dabigatran, apixaban | 56 (39–66) | 54 (36–69) | 44 | 65 | N.R. | N.R. | D
S | 10
29 | 13
44 | N.R. |
Liu23; retrospective cohort study; rivaroxaban, apixaban | 40 (33–52) | 46 (37–57) | 71 | 70 | 48 (29–62) | 56 (32–85) | S | 53 | 92 | N.R. |
Schulz24; retrospective cohort study; rivaroxaban, apixaban, edoxaban | 50 (31–66) | 46 (33–60) | 41 | 51 | 54 | 96 | S + D | 24 | 15 | N.R. |
Franke25; retrospective cohort study; rivaroxaban, dabigatran, apixaban, edoxaban | 55 (21–81) | 51 (21–76) | 52 | 58 | 16 (1–61) | 32 (3–91) | S + D | 116 | 77 | N.R. |
Bakow21; retrospective cohort study; N.R. | N.R. | N.R. | N.R. | N.R. | N.R. | N.R. | S + D | 54 | 76 | N.R. |
Sikorska26; prospective cohort study; apixaban | 44.5 (37–51) | 43.5 (34–57) | 85 | 85 | 58 (54–66) | 50 (38–53) | D
S | 23
28 | 25
38 | 63 |
Bakow20c; retrospective cohort study; N.R. | N.R. | N.R. | 40 | 68 | N.R. | N.R. | S | 44 | 54 | N.R. |
Cohen15; randomized clinical trial; rivaroxaban | 47 (17) | 50 (14) | 74 | 71 | 7 | 7 | D
S | 16
34 | 19
28 | 53 |
Ordi‑Ros10; randomized clinical trial; rivaroxaban | 47 (40–55) | 51 (38–63) | 64 | 63 | 35 | 35 | S + D | 37 | 38 | 56 |
Woller9; randomized clinical trial; apixaban | 46 (11) | 47 (13) | 83 | 84 | 12 | 12 | D
S | 4
5 | 2
7 | 60 |
In the cohort studies, women prevailed in 3,23,25,26 men in 1,27 and 3 studies20,22 had a balanced representation of both sexes. Median age of the participants was 43–55 years, and the follow‑up duration varied between 16 and 96 months. Nevertheless, 3 studies24,25,27 reported a significantly shorter follow‑up in the patients treated with DOACs than in those treated with VKAs, and 3 studies20-22 did not provide data on follow‑up duration. Two studies20,23 included only patients with a single positive antibody test, while 6 studies21,22,24-27 included both single- and double‑positive patients.
Only 4 studies9,10,15,26 reported median TTR in the patients treated with VKAs as ranging from 53% to 63%.
Quality of the study assessment
RCT summary of the risk of bias assessment is reported in Supplementary material, Figure S1. Although open‑label, all RCTs used an appropriate randomization process. We assessed the Ordi‑Ros et al10 trial as one with a high risk of bias due to the considerable number of patients lost to follow‑up without an adequate justification. Also the study by Woller et al9 raised some concerns about a deviation from the intended intervention by changing the protocol during the trial and switching apixaban from 2.5 mg twice daily to 5 mg twice daily.
Supplementary material, Table S2 summarizes quality assessment items for observational studies. All studies evaluated by NOS were classified as high‑quality.
Outcomes
Thrombosis recurrence
As many as 10 studies9,10,15,21-27 totaling 439 patients treated with DOACs and 481 with VKAs were included in the random‑effect meta‑analysis. The pooled RR of recurrent thrombosis was not significantly different in the individuals treated with DOACs vs VKAs (RR, 0.78; 95% CI, 0.36–1.69; I2 = 49%), with an opposite trend in RCTs (RR, 2.54; 95% CI, 0.61–10.59; I2= 0%), as compared with the observational studies (RR, 0.6; 95% CI, 0.25–1.39; I2 = 52%; Figure 2).
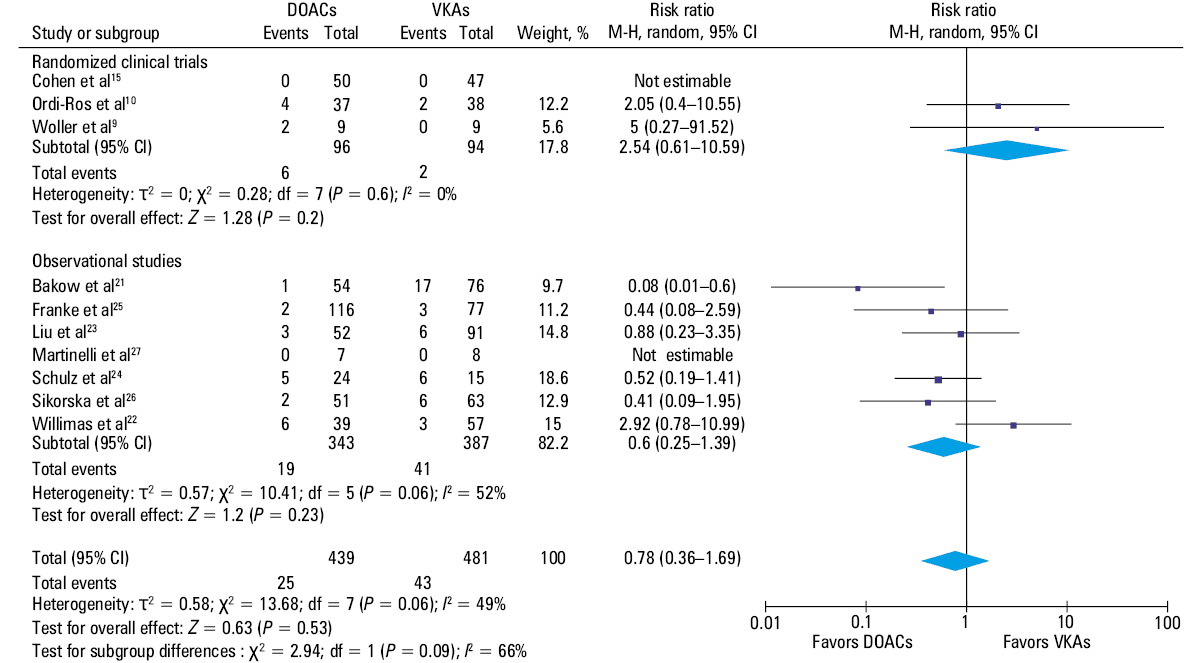
The heterogeneity among observational studies was moderate (I2 = 52%) but dropped to low (I2 = 8%) after the omission of 1 study.22 This study was the only one in which the number of thrombotic recurrences was higher in the DOAC group than in the VKA group, even though the follow‑up duration in the 2 groups was not reported. Considering only the studies with similar follow‑up times between treatments, the comparable efficacy of DOACs vs VKAs for secondary thromboprophylaxis was confirmed (RR, 1.02; 95% CI, 0.43–2.43; I2 = 6%; Supplementary material, Figure S2).
The funnel plot analysis was limited by the number of studies included, which was 10. However, it appeared quite asymmetrical, especially for the lack of studies in the bottom‑left quadrant (Supplementary material, Figure S3).
Subgroup analyses
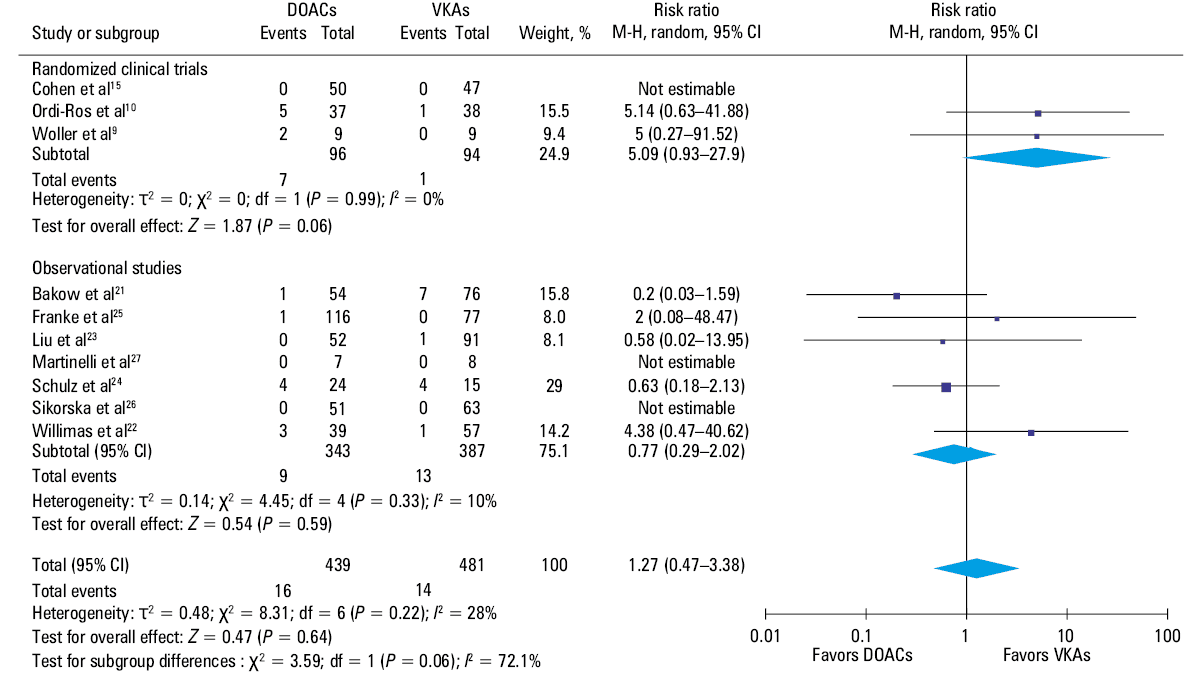
All studies included in the main analysis reported data stratified by the vascular bed of thrombosis (arterial or venous). Arterial thrombosis occurred in 16 out of 439 patients treated with DOACs and 14 out of 481 treated with VKAs. Indeed, no significant difference in efficacy was observed between the 2 treatments (RR, 1.27; 95% CI, 0.47–3.38; I2 = 28%; Figure 3), although in the RCT subgroup greater efficacy of VKAs could be noted (RR, 5.09; 95% CI, 0.93–27.9).
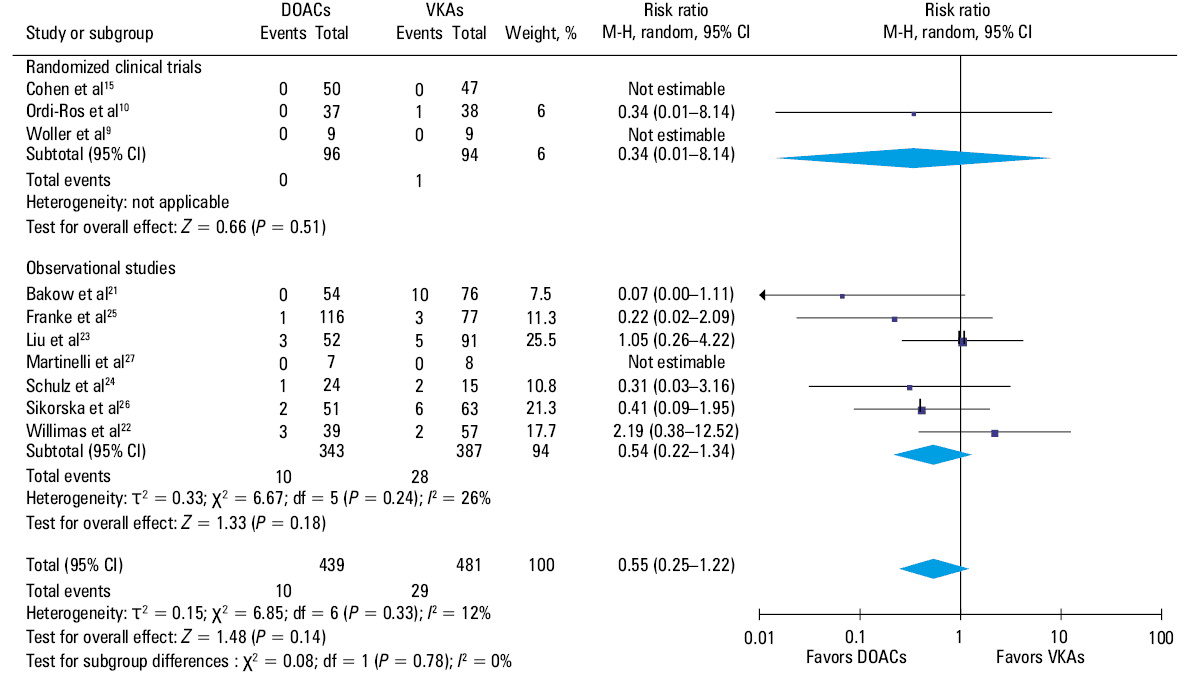
Venous thrombosis occurred in 10 out of 439 patients treated with DOACs and 29 out of 481 treated with VKAs. There was no significant difference in recurrent venous thrombosis between patients treated with DOACs vs VKAs (RR, 0.55; 95% CI, 0.25–1.22; I2 = 12%; Figure 4).
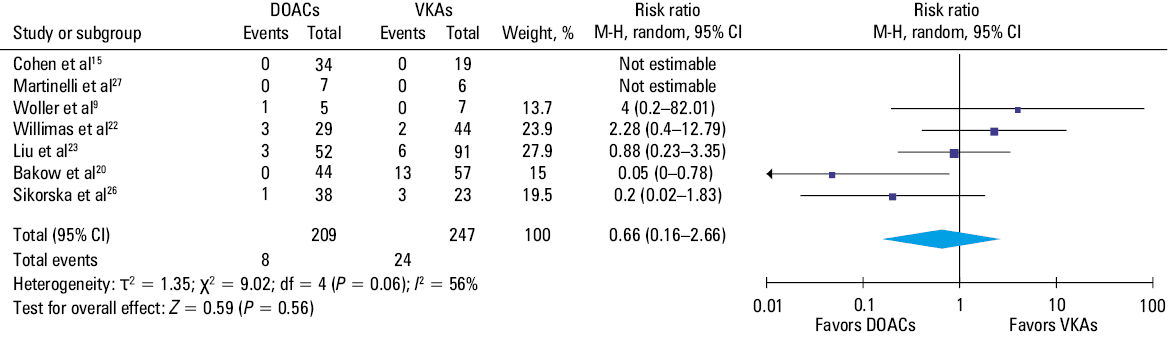
Finally, 7 studies9,15,20,22,23,26,27 reported the outcomes of patients with a single positive aPL test only, totaling 209 patients treated with DOACs and 247 with VKAs. An insignificant reduction in the risk of thrombosis recurrence was observed for those treated with DOACs vs VKAs (RR, 0.66; 95% CI, 0.16–2.66; I2 = 56%; Figure 5).
Bleeding
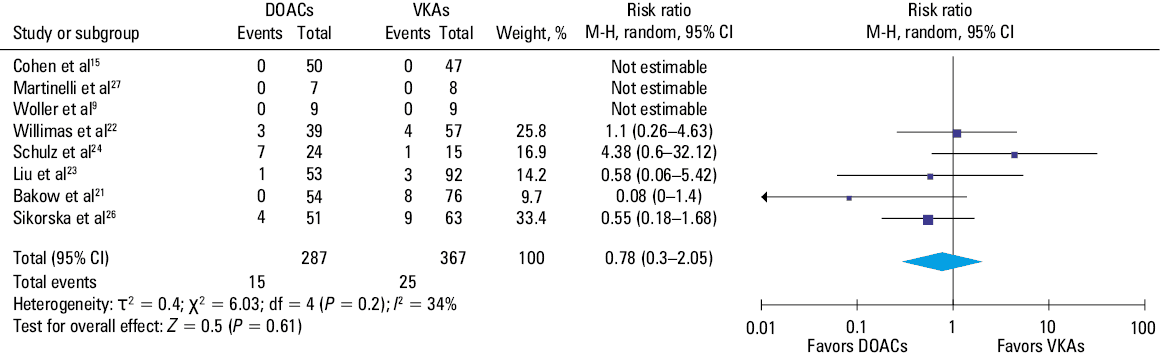
Two RCTs9,15 and 6 observational studies21-24,26,27 reported data regarding the safety outcome of patients with single- or double‑positive APS. Major bleeding was defined as each bleeding event of grade 3 or 4 according to the World Health Organization in 2 studies,21,23 and according to the International Society on Thrombosis and Haemostasis definition in the others.9,15,22,24,26,27 In 3 studies, no major bleeding events were observed, while 124 reported together major bleeding and CRNMB. Indeed, overall 15 out of 287 patients in the DOACs group and 25 out of 367 in the VKAs group suffered from major bleeding/CRNMB (RR, 0.78; 95% CI, 0.3–2.05; I2 = 34%; Figure 6).
Discussion
The main finding of our meta‑analysis including 920 patients with single- or double‑positive APS is that the efficacy of secondary thromboprophylaxis with DOACs is comparable to that with VKAs. Our analysis reported no difference between the 2 treatment arms, even though the trend for efficacy was opposite in the RCTs and observational studies, with a lower risk with VKAs in the first and a lower risk with DOACs in the latter. However, it must be highlighted that none of the RCTs was specifically designed to include only patients with single- or double‑positive aPL tests, which indeed represented less than 50% of the study population in both Woller et al9 and Ordi‑Ros et al10 studies.
The aPL profile is a well‑established risk factor for both first thrombosis in asymptomatic carriers and recurrences in those who have already had an event. As regards asymptomatic carriers, Mustonen et al28 reported the average annual rate of the first thrombotic event among patients with single-, double- and triple‑positive aPL profiles of 0.74%, 1.15%, and 1.85%, respectively. Similarly, Pengo et al29 reported the annual rate of the first cardiovascular event of 1.36% among 125 single aPL‑positive carriers. Among carriers with a single positive test, LAC appears to be associated with the highest risk of thrombotic events,30 and even transitory test negativity does not seem to modify the risk of suffering from a future thrombotic event.31
Similarly, patients with established APS and triple positivity have the highest risk of recurrences. Pengo et al32, in a retrospective analysis of 160 triple‑positive patients, reported a cumulative incidence of recurrence of 12.2% at 1 year. Recently, Mittal et al,33 in their single‑center experience, observed a significantly shorter recurrence‑free survival among triple‑positive patients in comparison with those non–triple‑positive (HR, 3.2; 95% CI, 1.03–11.1). Consistently, studies including only APS patients with single positivity report a lower cumulative incidence of recurrences, as compared with triple‑positive patients, even though the results are still debatable regarding the profile that confers the highest risk. Bakow et al20 reported a higher incidence rate of recurrence among patients positive for anticardiolipin (aCL; 5.88 per 100 patient‑years; 95% CI, 0.73–11.04) vs LAC (2.52 per 100 patient‑years; 95% CI, 0.96–4.08) and anti–β2‑GPI (2.58 per 100 patient‑years; 95% CI, 2.49–7.67), while Liu et al23 reported a 4.5‑fold increased risk in LAC‑positive patients than aCL‑positive ones, even though the difference did not reach significance.
In summary, data indicate that there probably are consistent risk differences among APS patients with different aPL profiles, and this could potentially motivate different treatment strategies in patients with a lower risk, that is, those without triple positivity.
Our meta‑analysis highlighted that the efficacy of DOACs and VKAs in the prevention of arterial thrombosis in the patients with single or double positivity did not significantly differ, although in the RCT subgroup there was an insignificant trend toward greater efficacy of VKAs. We hypothesize that the lower thrombotic risk could potentially account for the efficacy of DOACs, limited to this population, in preventing thrombotic recurrence also in this vascular bed. However, European Alliance of Associations for Rheumatology guidelines1 specifically recommend against the use of DOACs in APS patients due to a high number of arterial thrombotic recurrences in 2 RCTs,10,34 and in the meta‑analysis of RCTs by Dufrost et al13 reporting a 5‑fold increased risk of recurrent arterial thrombosis with anti‑factor Xa DOACs, as compared with VKAs. There is a lack of observational data on the matter, although in the subgroup of cohort studies in the meta‑analysis by Wu et al17 there was no difference between DOACs and VKAs. Still, our results should be interpreted with caution.
On the other hand, our analysis confirmed the comparable efficacy of DOACs and VKAs in preventing recurrent venous thrombosis. This finding was consistent in both RCTs and observational studies, and was comparable to those reported for higher‑risk patients in previous meta‑analyses by Dufrost et al13 and Wu et al.17
Finally, DOAC treatment is safe and, in our analysis, it was associated with a reduction of the risk of bleeding by around 20% as compared with VKA treatment, although the difference was not statistically significant. This finding mainly comes from the analysis of observational studies, due to the low number of events among patients with single- or double‑positive aPL tests in the RCTs. However, in the RCTs, the bleeding risk is traditionally lower as compared with the real‑world data due to the generally healthier patients included in the trials. Therefore, even if the result is not unexpected due to the strong safety profile of DOACs regardless of indication (ie, atrial fibrillation, venous thromboembolism), its relevance should not be underestimated and should be properly taken into account for evaluating the balance of benefits and risks of each anticoagulant therapy. Finally, to properly account for the risk / benefit profiles of each treatment, it would be of value to report data on adherence and TTR. Remarkably, only 4 of the 11 considered studies reported the TTR, which was around 60%, and no data on adherence were specified. These aspects should be properly assessed in the design of future studies to allow for better result interpretation.
Our meta‑analysis has some limitations. First, to broaden the sample size, we pooled together RCTs and observational studies, although their different designs could affect the pooled results. Moreover, the open‑blind design of the RTCs included does not allow to exclude performer and observer bias, whereas the retrospective nature of most of the observational studies implies the risk of selection bias and unmeasured confounders. The heterogeneity among the studies was moderate, despite our efforts to address heterogeneity by using the random‑effects model; therefore the results should be evaluated with caution.
Second, in the observational studies, the median follow‑up of patients treated with DOACs was generally shorter than of those treated with VKAs. This could lead to a false reduction of events in the DOAC group due to the shorter observation time. However, when we considered only the studies with similar follow‑up times among the groups, our results were consistent. Third, we had no access to individual patient data (IPD), so it was not possible to stratify the efficacy of anticoagulant therapy according to the specific antibody profile, or to establish whether there were differences in outcomes according to the type of DOAC that was used. Indeed, due to the strong relationship between each antibody test and the risk of recurrence, as well as the potential difference in efficacy and safety among DOACs, IPD meta‑analysis could yield more specific results.
Finally, we did not identify any unpublished studies. As it is known that publication bias can influence the results of meta‑analyses, we explored this potential bias using the funnel plots, which appeared asymmetrical, not allowing us to exclude the presence of publication bias.
In conclusion, our study identified a possible role of DOACs in the treatment of patients with single- or double‑positive APS that, in comparison with triple‑positive patients, have a lower risk of recurrent thrombosis. Indeed, the results of trials involving triple‑positive patients might not be generalizable to patients with different aPL profiles, and a tailored therapy should be identified for each patient, also taking into account the bleeding risk. To confirm our findings, further RCTs aimed at exploring the efficacy of DOACs in this specific population should be carried out.
- Tektonidou MG, Andreoli L, Limper M, et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Ann Rheum Dis. 2019; 78: 1296‑1304. | Crossref
- Garcia D, Erkan D. Diagnosis and management of the antiphospholipid syndrome. N Engl J Med. 2018; 379: 1290. | Crossref
- Barbhaiya M, Zuily S, Naden R, et al. 2023 ACR/EULAR antiphospholipid syndrome classification criteria. Ann Rheum Dis. 2023; 82: 1258‑1270.
- Radin M, Foddai SG, Barinotti A, et al. Reducing the diagnostic delay in antiphospholipid syndrome over time: a real‑world observation. Orphanet J Rare Dis. 2021; 16: 280. | Crossref
- Ortel TL, Neumann I, Ageno W, et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020; 4: 4693‑4738. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION