Dual pattern of immune-related hepatotoxicity induced by pembrolizumab: hepatitis and sclerosing cholangitis

 CC BY 4.0
CC BY 4.0
Dual pattern of immune-related hepatotoxicity induced by pembrolizumab: hepatitis and sclerosing cholangitis
Introduction of immune checkpoint inhibitors (ICIs) has significantly advanced oncology, particularly in treatmemt of melanoma, non‑small cell lung cancer, and triple‑negative breast cancer (TNBC). Although ICIs can produce durable responses, their use is limited by immune‑related adverse events (irAEs) affecting various organ systems. Hepatotoxicity, although less frequent than other irAEs, presents a major clinical challenge. Immune‑mediated hepatitis and the rarer immune‑related sclerosing cholangitis (irSC) require careful monitoring and timely interventions to prevent serious outcomes.
We present a case of a 37‑year‑old woman with early‑stage TNBC (pT1cN1, Ki67 >30%) who underwent mastectomy with sentinel lymph node biopsy, followed by adjuvant systemic therapy with 4 cycles of dose‑dense doxorubicin and cyclophosphamide combined with pembrolizumab, and then 12 cycles of paclitaxel with pembrolizumab.
After 1 dose of paclitaxel and 3 doses of pembrolizumab, the patient developed severe liver injury. Laboratory tests showed alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels of 4528 U/l (reference range [RR], 7–30 U/l) and 4917 U/l (RR, 5–40 U/l), respectively, accompanied by hyperbilirubinemia, coagulopathy, and hyperammonemia. Extensive evaluation excluded other causes of liver dysfunction, such as viral hepatitis, liver metastases, and hepatic vascular thrombosis. Due to coagulopathy, liver biopsy was not feasible. Based on the temporal relationship with pembrolizumab administration, a diagnosis of immune‑related hepatotoxicity was established.
The patient was treated according to European Society for Medical Oncology Clinical Practice Guidelines, receiving high‑dose intravenous methylprednisolone combined with acetylcysteine and ursodeoxycholic acid (UDCA). Liver function gradually improved, allowing for radical surgery.
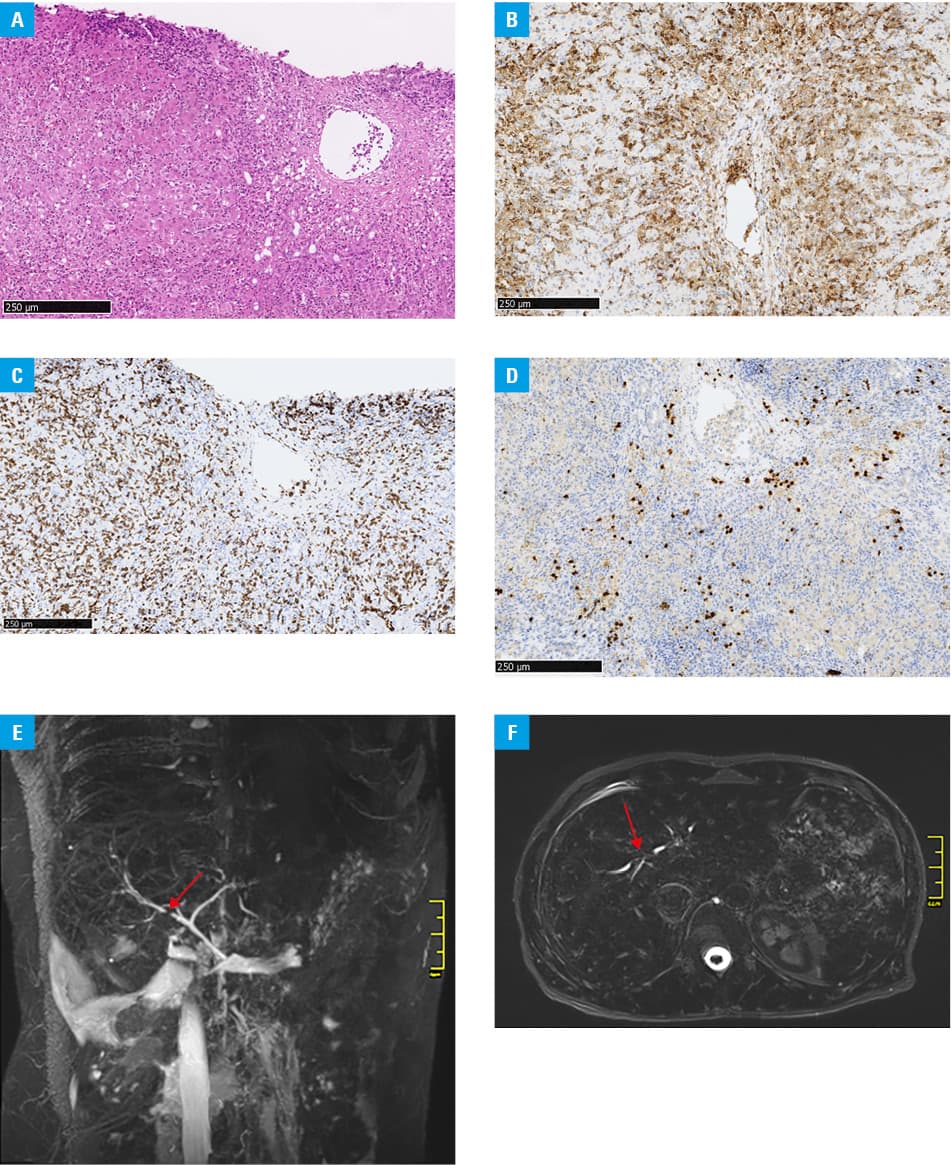
Several days postoperatively, the patient experienced a recurrent liver injury with ALT and AST levels of 1273 U/l and 1573 U/l, respectively, as well as elevated cholestatic markers: total bilirubin of 60.36 µmol/l (RR, 3.42–20.52 µmol/l), γ-glutamyl transpeptidase of 601 U/l (RR, 7–50 U/l), and alkaline phosphatase of 669 U/l (RR, 30–120 U/l). Liver biopsy showed portal and lobular inflammation with predominantly cytotoxic T lymphocytes and plasma cells, consistent with immune‑related hepatitis (Figure 1A and 1D). Magnetic resonance cholangiopancreatography identified intrahepatic biliary strictures and irregularities suggestive of irSC (Figure 1E and 1F). Reintroduction of corticosteroids and continuation of UDCA led to gradual normalization of liver function. At 6‑month follow‑up, the patient remained free from breast cancer recurrence with stable liver biochemistry.
Understanding the pathophysiological distinction between immune‑related hepatitis and irSC is critical. The former one primarily targets hepatocytes, resulting in lobular inflammation, whereas the latter involves immune‑mediated bile duct injury, leading to fibrosis and stricturing.
Biliary involvement in irAEs, particularly in the form of irSC, is rare. It affects approximately 4% of patients, and remains poorly defined.1 There are no established diagnostic criteria for irSC. It is typically diagnosed through radiographic identification of biliary dilation without obstruction, diffuse hypertrophy of the extrahepatic bile ducts, or multiple intrahepatic strictures.2 Current guidelines suggest corticosteroids and immunosuppressive therapies, often combined with UDCA, although management is limited by low‑quality evidence.3
It is important to note that immune‑related hepatitis may recur during corticosteroid tapering, underscoring the need for close monitoring and individualized immunosuppressive regimens. Clinicians should remain vigilant for irSC in patients with cholestatic liver enzyme elevations, particularly when hepatitis is resistant to steroids. In such cases, UDCA may offer therapeutic benefits, although further studies are needed to define optimal management strategies.
- Zheng C, Huang S, Lin M, et al. Hepatotoxicity of immune checkpoint inhibitors: What is currently known. Hepatol Commun. 2023; 7: e0063. | Crossref
- Onoyama T, Takeda Y, Yamashita T, et al. Programmed cell death‑1 inhibitor‑related sclerosing cholangitis: a systematic review. WJG. 2020; 26: 353‑365. | Crossref
- Haanen J, Obeid M, Spain L, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow‑up. Ann Oncol. 2022; 33: 1217‑1238. | Crossref
ARTICLE INFORMATION