Nonstandard superficial vein thrombosis management. Should we consider a tailored approach? A critical review and discussion
Key words: angiopathies, management of disease, tailored medicine, venous thrombosis

 CC BY 4.0
CC BY 4.0
Nonstandard superficial vein thrombosis management. Should we consider a tailored approach? A critical review and discussion
Thrombophlebitis is an inflammatory process in the superficial veins with coexistent vein thrombosis, usually occurring in patients with specific preconditions (trauma, surgery or inactivity, signs of venous insufficiency, malignancies). The concept of thrombophlebitis has evolved over time, and its definition has changed from thrombophlebitis to superficial vein thrombosis (SVT). SVT course is usually benign, if appropriate and prompt treatment is undertaken. Pharmacologic treatment includes anticoagulation with low‑molecular‑weight heparin, fondaparinux and, more recently, rivaroxaban. In selected cases, the course of thrombophlebitis is not self‑limited, and its management is challenging for clinicians and varies in different centers. SVT complications include deep vein thrombosis, pulmonary embolism, and thrombosis recurrence. In this review, we define nonstandard SVT as the cases presenting with 1 or more of the following features: SVT involving healthy veins; recurrent, migrant, or significantly extended SVT; SVT involving deep vein confluence; or SVT not associated with recognized risk factors, especially if occurring in young individuals. In such nonstandard cases, SVT may also represent the epiphenomenon of a more complex systemic condition. Therefore, investigation may require more attention and resources. This series of clinical cases focuses on uncertainties in the management of nonstandard SVT, from diagnosis to treatment, and it underlines, on the one side, the need of a multidisciplinary approach to investigation and care, and on the other side, the opportunity of a systematic data collection and analysis to provide more reliable recommendations in this setting.
Introduction
Thrombophlebitis, more recently called superficial vein thrombosis (SVT), is an inflammatory process in the superficial veins with coexistent venous thrombosis1,2 occurring usually but not exclusively in the lower limbs. Varicose veins represent the main risk factor for lower limb SVT (80%–90%).3 Moreover, patients may have a history of antecedent trauma, surgery or immobility, intravenous cannulation, or infusion of irritants.2
A number of local and systemic risk factors for SVT are recognized, both nonmodifiable and acquired (largely modifiable), some of them with a still controversial role. A list of recognized risk factors for SVT development is included in Table 1.
Nonmodifiable | Acquired |
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism; SVT, superficial vein thrombosis | |
Age >65 years | Obesity |
Personal history of SVT/DVT/PE | Cancer |
Family history of SVT/DVT | Surgery / vascular surgery |
Chronic vein insufficiency | Hospitalization / immobilization |
Lower limb varicose veins | Prolonged travel |
Thrombophilias | Pregnancy |
Hormonal therapy | |
Autoimmune diseases | |
Drugs (steroids, Janus kinase inhibitors, chemotherapy, parenteral nutrition) | |
Although currently underestimated, the prevalence of SVT is higher than that of deep vein thrombosis (DVT) and pulmonary embolism (PE), as it ranges from 3% to 11%.4-6
If appropriate treatment is promptly undertaken, SVT prognosis is generally more favorable than that of DVT.7
In some cases, this relatively common process is less benign and self‑limiting than previously supposed. SVT can be associated with DVT in 6%–40% of patients at diagnosis,8-11 and can also be linked to more serious complications, such as asymptomatic PE in 20%–33% of cases, and symptomatic PE in 2%–13% of cases.12-14 In the POST (Prospective Observational Superficial Thrombophlebitis) study, the cases of DVT confirmed on Doppler ultrasound (DUS) and symptomatic PE were reported in 24.9% and 3.9%, respectively, in 844 patients with SVT.15 A meta‑analysis by Di Minno et al16 reported a weighted mean prevalence of 18.2% for DVT, and 8.2% for PE among patients with SVT.
A residual risk for recurrence is not negligible. The patients with a history of SVT seem to have a particularly increased risk for successive venous thrombosis, as compared with individuals without previous SVT. After a large case‑control study with over 10 000 participants showed a 5.5‑fold higher risk of SVT recurrence, a more recent study confirmed a similar recurrence rate in patients with isolated SVT, as compared with individuals with proximal DVT (5.4% vs 6.5% per patient/year), the former recurring more often as SVT than as DVT.7 The risk of recurrence was further increased in individuals with an acquired mild thrombotic risk factor (smoking or overweight) in addition to previous SVT, with different impact on SVT recurrence risk according to the type of the risk factor (a 31.4‑fold higher risk in patients with a strong thrombotic risk factor, ie, surgery, hospitalization, plaster cast immobilization, or malignancy, and a 34.9‑fold higher risk in women with a reproductive risk factor, such as hormonal therapy, pregnancy, and puerperium).17
In contrast with DVT, reliable scores allowing for identification of SVT cases at a high risk of DVT and recurrence are lacking; the promising ICARO score, a clinical score predicting the risk of DVT in patients with SVT, was not so successful.18 Nevertheless, specific features commonly used to identify an episode of SVT considered as high risk for venous thromboembolism (VTE) include: proximal SVT, involvement of nonvaricose vein, the presence of autoimmune disease, age above 65 years, previous VTE, or a diagnosis of cancer.19 Concerning recurrence, risk factors for recurrence in the POST study were identified as SVT involving an apparently healthy vein, cancer, male sex, and previous DVT.19 Recurrence rates for DVT or SVT are similar.7 There are different types of SVT including: nonstandard SVT (SVT involving healthy veins; recurrent, migrant, or significantly extended SVT); SVT involving deep vein confluence; or SVT not associated with recognized risk factors, especially if occurring in young individuals. SVT may represent the epiphenomenon of a more complex, often systemic condition.
Background of current treatments and perspectives
In general, anticoagulant treatment of SVT appears to be the most appropriate choice, as up to a quarter of untreated cases was associated with extension to deep venous system (DVS) or recurrence, while this did not occur in anticoagulated patients.20,21
In the case of SVT located 3 or more centimeters away from the DVS and 5 or more centimeters in length, a 45‑day regimen of anticoagulation is recommended (class IB).22 Guidelines recommend treatment of SVT with fondaparinux at a dose of 2.5 mg (class IB) or with low‑molecular‑weight heparin (LMWH) at intermediate doses (class IIa B).22
An overview of the main randomized trials exploring anticoagulation treatment of SVT is included in Table 2.
Trial | Inclusion criteria | Agent vs comparator | Efficacy outcomes | Safety |
Abbreviations: OD, once daily; VTE, venous thromboembolism; others, see Table 1 | ||||
STENOX21 | SVT ≥5 cm in length on ultrasound | Enoxaparin in therapeutic or prophylactic doses for 12 days | Risk of recurrence and / or proximal extension 5.7% on a therapeutic dose vs 8.2% on a prophylactic dose vs 29.5% on placebo | No death or major hemorrhages |
STEFLUX23 | SVT ≥4 cm in length | Parnaparin 8500 IU OD for 10 days followed by placebo for 20 days (group A) vs 8500 IU OD for 10 days followed by 6400 IU OD for 20 days (group B) vs 4250 IU OD for 30 days (group C) | Composite outcome (DVT, PE, and SVT recurrence) in 15.6% (group A) vs 1.8% (group B) vs 7.3% (group C) | No major hemorrhages |
CALISTO24 | SVT ≥5 cm in length, located 3 cm away from the junction with the deep veins | Subcutaneous fondaparinu × 2.5 mg OD or placebo for 45 days | Death or symptomatic VTE events (PE, DVT, SVT extension to junction, and SVT recurrence in 0.9% in the fondaparinux group and 5.9% in the placebo group (P <0.001) | No increased bleeding risk |
SURPRISE25 | Symptomatic SVT, location above the knee, ≥5 cm, and at least 1 additional risk factor | 10 mg oral rivaroxaban or 2.5 mg subcutaneous fondaparinux OD for 45 days | Symptomatic DVT, PE, progression or recurrence of SVT, and all‑cause mortality in 3% in the rivaroxaban group vs 2% in the fondaparinux group (P = 0.003). | No major bleeds in either group |
The STEFLUX (Superficial Thromboembolism and Fluxum) trial23 compared parnaparin 8500 IU once daily for 10 days followed by placebo for 20 days (group A) with parnaparin 8500 IU once daily for 10 days followed by 6400 IU once daily for 20 days (group B), and parnaparin 4250 IU once daily for 30 days (group C) in the treatment of SVT 4 or more centimeters in length. In this study, intermediate dose of parnaparin for 30 days was more efficacious than a 30‑day prophylactic dose or a 10‑day intermediate dose for a reduction of DVT, PE, and SVT recurrence following lower limb SVT.23
In the CALISTO (Comparison of Arixtra in Lower Limb Superficial Thrombophlebitis with Placebo), a multicenter, double‑blind, placebo‑controlled trial,24 fondaparinu × 2.5 mg given subcutaneously once daily for 45 days in approximately 3000 patients was effective and safe, as compared with placebo in acute SVT of the legs (symptom onset less than 3 weeks before randomization). In this study, the risk of DVT and PE was significantly reduced in the fondaparinux arm vs placebo (P = 0.001 and P = 0.02 by day 77, respectively).
In comparison with the patients with DVT/PE, less robust data support direct oral anticoagulant (DOAC) use for SVT treatment. In the prospective, randomized SURPRISE (Superficial Vein Thrombosis [SVT] Treated with Rivaroxaban Versus Fondaparinux) trial, rivaroxaban 10 mg given once daily for 45 days was safe and noninferior as compared to fondaparinux in preventing thromboembolism in the setting of high‑risk SVT.25 In real‑world clinical practice, due to a lack of power of the noninferiority SURPRISE study, rivaroxaban is still not considered in guidelines22 or for approval by regulatory agencies.
Randomized studies testing the possible application of DOACs for SVT treatment are still unavailable.
However, with a view to hypothetical or off‑label (at the moment) use of DOACs in this setting, the selection of patients remains challenging, requiring a case‑by‑case discussion and the patient’s personal involvement.
In our opinion, DOACs have to be considered for very specific cases only, in particular extended proximal SVT (SVT significantly >5 cm, especially located along the thigh) or SVT located very close to the junctions with deep veins (<3 cm). In such situations, DOACs may represent a more convenient choice than parenteral anticoagulation for a full‑dose 3‑month course DVT‑like treatment, as already suggested by Potere and Ageno for distal DVT treatment.26
Obviously, DOACs could be also an option for patients with SVT who deliberately refuse parenteral administration of drugs, and when reduced compliance to parenteral administration may severely compromise the results of treatment.
The role of nonsteroidal anti‑inflammatory drugs (NSAIDs) in SVT is still insufficiently studied.21 So far, NSAIDs are not taken into consideration by the guidelines.
To date, no study is available showing increased rate of thrombosis recanalization with increased dose of anticoagulation. Nevertheless, it has been postulated that risk stratification systems could be useful at baseline, as patients at a high risk for SVT complications may benefit from a more aggressive treatment. Contrary to that, patients with low‑risk SVT (asymptomatic, <5 cm in length) may not need anticoagulation at all,27 thus improving the cost‑effectiveness ratio of therapy in this setting.
Despite no strong data supporting long‑term anticoagulant treatment, in a recently published meta‑analysis of 24 studies, prolonged anticoagulation was associated with a reduction of DVT risk in patients with SVT limited to lower extremities, while the highest rates of DVT and PE were associated with particularly short‑term (≤14 days) treatment course.28
The decision on long‑term anticoagulation requires a case‑by‑case evaluation, taking into account all risk factors for SVT complications and frequency of SVT relapses.
In our view, a prophylactic dose of a DOAC (eg, rivaroxaban 10 mg once daily, as in the SURPRISE trial) could be an option not only in the acute treatment (45 days) but also in the following long‑term prophylaxis of SVT at a high risk for recurrence, for instance in patients with persistent risk factors, such as malignancies and autoimmune diseases (not associated with a high risk of bleeding).
In the case of recurrent SVT (n ≥3), the possibility of a prolonged treatment requires discussion with the patient, particularly with regard to the patient’s bleeding risk and personal preferences regarding the type of treatment.27
Diagnostic evaluation
Limited consensus exists about the need and modality of SVT investigation, making further studies on this topic advisable in our opinion, as available data are not only scarce but also only retrospective.
We defined nonstandard SVT in patients presenting with 1 or more of the following features: not adequately explained SVT, no involvement of a varicose vein, recurrent, migrant, or particularly extended proximal SVT, SVT with deep vein confluence involvement, etc.
In nonstandard SVT, thrombophlebitis may conceal several clinical settings deserving special attention due to a high risk of complications. Moreover, SVT may mask more complex, systemic conditions.
Information on the association between oncologic diseases and SVT is relatively scarce, as compared with DVT (in some studies in SVT patients cancer was an exclusion criterion, in other studies the prevalence of cancer was not mentioned).
Anyway, cancer may represent the strongest determinant of SVT complications, according to the results of dedicated studies. In particular, in a single‑center study of 276 consecutive SVT cases, a cancer diagnosis was present in a significantly higher percentage of patients with SVT and concurrent DVT/PE (18.8% vs 8.7% of those in the SVT‑only group; P <0.001).29
The prospective INSIGHT SVT (Investigating Significant Health Trends in the Management of Superficial Vein Thrombosis) trial,30 including patients with isolated SVT, showed that 6.7% of the patients received a diagnosis of cancer before SVT or within 1 year after SVT diagnosis, and that the diagnosis of malignancy increased the risk of VTE vs noncancer patients (13% vs 5.4% after 3 months), which suggests benefits from extended anticoagulation in this setting.
Beyond cancer, SVT may represent the event indicating many other more complex conditions (chronic autoimmune diseases, thrombophilia, etc.), not necessarily known at SVT diagnosis, probably acting as local or systemic triggering factors.
Here, we report a series of clinical cases of patients with nonstandard SVT history calling for tailored management of SVT (diagnosis and treatment) in specific settings.
Case 1
A 55‑year‑old woman of normal weight and without cardiovascular risk factors was referred to our center for observation for her first spontaneous episode of SVT in the right leg, without any signs of venous insufficiency on DUS examination. Her family and personal history were both negative for arterial and / or venous thrombosis. She had 2 pregnancies, without obstetric complications.
Two years later, SVT recurrence became particularly frequent (3 episodes per year) in different sites and in both legs; DVS was never involved.
Each episode was treated with a standard prophylactic dose of LMWH for a total of 6 weeks, with only temporary complete resolution of thrombosis. Congenital and acquired thrombophilia testing resulted negative, as did abdomen ultrasound, chest‑X ray, and mammography. The patient reported abdominal pain and diarrhea in the last months.
A diagnosis of ulcerative rectocolitis was made 18 months after the first recurrence of SVT, and regular, still continued treatment with anti‑tumor necrosis factor α (TNF-α) was implemented. Alongside the long‑term anticoagulant treatment, rivaroxaban 10 mg once daily was introduced to reduce relapses. This represents an off‑label use of a DOAC, as agencies do not support the use of rivaroxaban for SVT treatment and secondary prophylaxis in any country.
A link between autoimmune diseases and SVT has been showed (1.3% of SVT patients in the POST study and 0.9% in the CALISTO study),31 and it appears widely variable and therefore unpredictable, depending on specific underlying condition.32
Even though not all the mechanisms explaining the increased risk of thrombosis in autoimmune diseases are known, systemic inflammation is largely recognized as the first contributor to endothelial dysfunction and platelet hyperactivation leading to hypercoagulability.33
Patients with inflammatory bowel disease (IBD) are at an increased risk for venous thrombosis, significantly affecting morbidity and mortality.34 In this setting, thrombosis is more often represented by DVT of the lower limbs and PE.35 The prevalence rate of VTE among patients with IBD ranges from 5.6% to 7.6%,36 independently from sex,37 accounting for a 2.3‑times greater risk of VTE events vs the general population, particularly in ulcerative colitis and Crohn disease.38-40 Moreover, the risk of thrombosis recurrence is higher in patients with previous unprovoked VTE.41
A prothrombotic state represents a possible result of qualitative and quantitative abnormalities in hemostatic balance, especially (but not exclusively) shown in acute inflammatory phase and represented by: 1) increased levels of coagulation factors, also acting as acute‑phase reactants (fibrinogen, factor [F] II, FV, FVII, FVIII, FX, FXI, and FXII); 2) downregulation of natural anticoagulant proteins (antithrombin, tissue factor pathway inhibitor, protein C, and protein S); 3) impairment of fibrinolytic system consisting in a reduction of a fibrinolysis activator (tissue plasminogen activator) and an increase in a fibrinolysis inhibitor (plasminogen activator inhibitor 1 and thrombin activatable fibrinolysis inhibitor) levels; 4) greater reactivity and sensitivity of platelets to agonists (increased levels of platelet activation markers: P‑selectin, GP53 and β-thromboglobulin, CD40L on the cell surface and in serum; increased platelet microparticle circulation); 5) high rates of antiphospholipid positivity (anticardiolipin, anti-β2‑glycoprotein I).42-44
Clinical factors that increase the likelihood of thrombosis among IBD patients include older age, pregnancy, active disease, more extensive disease, or hospitalization.34
Medications, such as corticosteroids and more specific drugs, for example, tofacitinib (Janus kinase inhibitor) and surgical procedures can further increase the risk of thrombosis.44 On the other hand, anti–TNF-α agents resulted in a 5‑fold decreased risk of venous thrombosis in comparison with steroids.45
Published data on SVT and IBD are scarce (a few anecdotal cases). In our view, the phenomenon is underestimated in the literature, as lower limb SVT usually shares common risk factors with DVT and, as a matter of fact, SVT in this setting is common in everyday angiologist and gastroenterologist practice, with or without coexistence of other local or systemic risk factors.
At least basic investigation for a possible IBD diagnosis is advisable in patients referred for recurrent SVT when 1 or more gastrointestinal symptoms are present, especially if SVT involves healthy superficial veins.
In this regard, particularly in acute inflammatory phases, IBD is considered a sort of acquired thrombophilia condition, requiring attention regarding thromboprophylaxis during hospitalization.
A reliable risk stratification system is desirable to identify the patients who may benefit the most from prophylaxis in the case of hospitalization but also postdischarge, during surgery, therapy increasing the risk of thrombosis, or when cardiovascular risk factors are present.
Thromboprophylaxis should be given to patients with IBD during hospitalization (6‑fold higher risk of thrombosis vs nonhospitalized patients)40 for any cause, and at least considered in ambulatory patients with active IBD.39 It is currently debated if thromboprophylaxis should be used in patients with inactive disease; in general, good control over the disease activity seems to reduce the risk of venous (and arterial) thrombotic events in patients with IBD.40
The optimal anticoagulant treatment strategy is not clear in many cases. Data supporting DOAC use for SVT in IBD patients are still lacking. The possible use of DOACs in IBD is even more challenging because of a high local bleeding risk. Apixaban seems the most appropriate due to its lower impact on gastrointestinal bleeding in IBD, even though the only agent actually tested in SVT is rivaroxaban.24
Case 2
A 45‑year‑old woman of normal weight, with no history of arterial thrombosis and / or DVT, reported 2 episodes of SVT. Her father had myocardial infarction at the age of 49 years, in the absence of cardiovascular risk factors.
After a red, warm, tender area and a palpable cord became visible on her left lower limb, she underwent DUS examination that showed the great saphenous vein thrombosis, not involving DVS. Treatment with subcutaneous fondaparinu × 2.5 mg once daily was promptly started. Coagulation tests performed on the advice of her gynecologist due to multiple miscarriages showed a reduced level of free protein S (42%; reference range, 60%–100%). Hereditary anticoagulant protein S deficiency was confirmed in the patient’s father and sister.
According to current recommendations,46 SVT is not a condition requiring genetic thrombophilia testing. However, thrombophilia was reported in 19.8% of all SVT cases in a study on 100 patients,46 and De Moerlose et al48 showed a significantly higher incidence of mild thrombophilia and FV Leiden (but not G20210A prothrombin variant) among 112 consecutive patients with SVT diagnosis than in controls (14.3% vs 6.1%).
It should be noted that specific data on diverse populations of patients with or without varicose veins are still not available.
In our view, genetic testing could be appropriate in selected cases of recurrent SVT, for example, occurring in healthy veins or in young patients with personal or family history strongly positive for thrombotic diathesis (previous DVT/PE, significant obstetric complications).
In fact, thrombophilia testing is widely performed even in unselected patients, as clinicians worldwide do not always adequately select patients for investigation,49 or simply these tests are available for a patient even before SVT has occurred. Therefore, the relevance of information on thrombophilia previously acquired, especially not mild thrombophilia, in the management of SVT episodes is not well established.
Genetic thrombophilia only minimally increases the risk of VTE in patients with a history of SVT.50 There are no clear data suggesting that thrombophilia may change the rate of SVT recurrence or progression.51,52
Also, no significant differences were found concerning SVT symptom duration, family or personal history of DVT/PE, or personal history of SVT in thrombophilia carriers and noncarriers.29
There are numerous uncertainties concerning SVT management, at least in the case of nonmild thrombophilia, potentially modifying treatment strategy. If SVT is considered just a local and nonsystemic condition, the information about thrombophilia should not affect the choice of the type and duration of anticoagulation.
However, in some SVT cases (SVT involving confluence with DVS, SVT diagnosed in patients with a DVT history) being a carrier of nonmild thrombophilia could entail a higher risk of complications, and therefore a long‑term anticoagulation strategy seems the most appropriate choice, as in DVT.
No study to date has explored treatment of SVT in this setting. At the moment, no data support administration of higher drug doses or longer treatment in SVT.
Case 3
A 60‑year‑old woman with normal weight and hypercholesterolemia was referred to our center. She had no family history of thrombosis, had 3 pregnancies without obstetric complications, and SVT of the right leg years ago after surgery treated with prophylactic LMWH doses for nearly 40 days. Two months ago she experienced acute pain in the left lower limb, and DUS showed thrombosis of the left great saphenous vein extending up to 2 cm from the confluence in the femoral vein, without clear signs of venous insufficiency. After SVT/DVT diagnosis was made, a therapeutic approach similar to the one reserved for DVT was chosen, according to current guidelines.53,54
Acquired thrombophilia testing including antiphospholipid antibodies, homocysteine levels, and tumor markers was negative, similarly as abdominal ultrasound, chest‑X ray, and bilateral mammography.
Treatment with edoxaban 60 mg once daily was started, and is still ongoing. The estimated treatment time is 3 months, according to the current guidelines for DVT,55 and then the patient will be assessed for the need of extended anticoagulant therapy.
Even though current guidelines recommend full‑dose anticoagulation in the case of SVT extending to deep veins or if a distance from the junction with deep circulation is less than 3 cm,56 randomized clinical trials exploring the usefulness of therapeutic vs preventive anticoagulation in SVT closer to the junction are not yet available; the presence of thrombus head within 3 cm from the superficial veins and DVS junction often made the patients ineligible for recruitment in studies addressing the treatment of SVT. The same occurred usually in studies addressing the treatment of DVT.56
As reported in different studies, such patients are at a higher risk for severe complications,11 and thus they need more aggressive management (usually anticoagulation for at least 3–6 months).57
In the RIETE (Registro Informatizado de la Enfermedad Tromboembólica) trial, fewer thromboembolic events were observed in patients treated with anticoagulants at therapeutic doses vs standard SVT treatment (1.3% vs 2.7%), despite more significant bleeding complications (1.3% vs 0.7%) after 3‑month follow‑up, thus showing that individual bleeding risk is crucial, especially in view of the controversial status of anticoagulant treatment of SVT/DVT.56 In a recent retrospective study, 192 of 316 patients (60.8%) had SVT over 3 cm from the sapheno‑femoral junction / saphenopopliteal junction at presentation, and underwent 90‑day follow‑up. Of these 192 patients, 59 (30.7%) started anticoagulant treatment, and 125 (65.1%) received conservative management. Complications occurred in 46.4% of the patients managed conservatively and 17.5% of those on any dose of anticoagulation; DVT/PE occurred in 8% of the patients treated conservatively vs 0% in those fully anticoagulated.58
While SVT diagnosis can be based on clinical presentation, ultrasound is the most often used diagnostic method, as it is cost‑effective, accurate, and safe for patients.59
Considering the number of patients with SVT symptoms having also DVT at diagnosis, it seems advisable to perform venous DUS in all patients with suspected SVT.15
Apart from confirming or excluding DVT, DUS scanning at diagnosis is useful to evaluate SVT extension, measure the distance to the deep circulation, and identify the presence of varicose veins.60
DUS reports are still not homogeneous, and they do not always include all parameters considered essential for a diagnosis and management of SVT. The exact distance of thrombus from the saphenous‑femoral or saphenous‑popliteal junction as well as the SVT extension are not always specified in clinical practice. As a consequence, clinicians often do not consider DVT involvement in many cases of SVT. A recent survey among Italian angiologists and vascular specialists showed a definitely heterogeneous therapeutic approach to SVT involving the sapheno‑femoral junction.54
Conclusions
In conclusion, little evidence is available regarding investigation and treatment of SVT.
A few trials focusing on treatment of lower limb SVT have been published (Table 2), but despite available recommendations, therapy often depends on the treating physician’s discretion, ranging from conservative treatment (including NSAIDs and close DUS follow‑up) to standard anticoagulation, mostly with fondaparinux and LMWH in various dosing schemes. Also, different centers used different duration of anticoagulation (usually 45 days but ranging between 4 and 8 weeks).1,21,29,61
We strongly support the hypothesis that the best approach to treatment should be tailored and take into account specific clinical setting and pathogenesis of SVT, although always with respect to current guidelines.
This series of clinical cases of nonstandard SVT history opens the possibility of personalized SVT management considering comorbidities, site and extent of thrombosis, features predisposing to DVT and PE, and finally evaluating interprofessional team strategies to improve coordination of investigation and care.62
In our view, initial diagnosis in patients younger than 40 years, with SVT involving healthy veins, individuals without specific risk factors or migratory thrombophlebitis should consider possible underlying conditions.
Trials are needed pursuing the following aims: 1) to develop interprofessional team strategies to improve coordination of care, thus allowing a more precise diagnosis, and to investigate underlying causes, thereby improving outcomes; 2) to underline the importance of identifying different etiologies of superficial thrombophlebitis in order to promptly begin the most appropriate treatment according to the site and extent of thrombosis; 3) to individually consider critical factors that predispose to DVT and PE; 4) to outline the management options identifying patients in need of a more aggressive management. Our proposal consists in a multidisciplinary approach to nonstandard SVT, mainly based on age, thrombotic family and personal history, and SVT extension in order to establish a complete diagnostic algorithm including a proper combination of blood tests, acquired thrombophilia, instrumental examinations, and congenital thrombophilia tests (Figure 1).
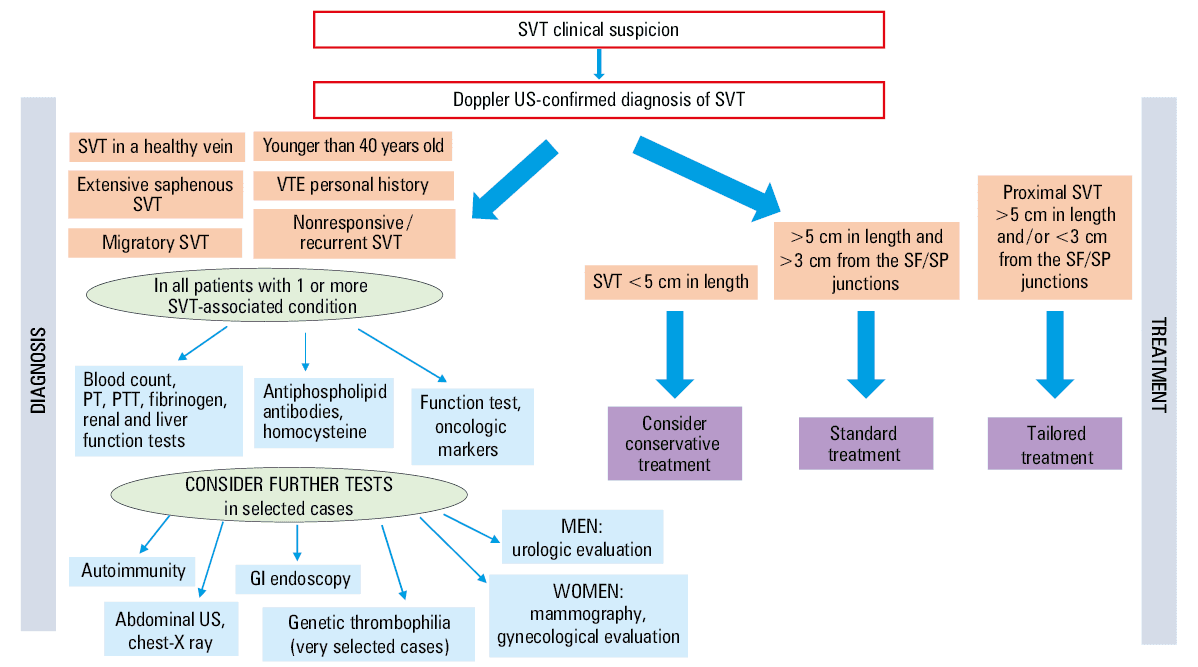
Abbreviations: GI, gastrointestinal; PT, prothrombin time; PTT, partial thromboplastin time; SF, sapheno‑femoral; SP, saphenopopliteal; US, ultrasound; others, see Table 1
Such an approach has multiple goals. First of all, this way we can be sure to collect data for a local registry of all nonstandard SVT cases for a complete data analysis, providing further information on the origin of the phenomenon. Secondly, collecting data for a local registry will make the approach to SVT more homogeneous. Thirdly, as a direct consequence of data collection, more complete information will be available on the most effective treatment in specific clinical settings. Finally, SVT may become a potential “filter” to investigate more complex clinical situations, such as cancer or autoimmune diseases, which we could not diagnose by limiting our diagnostic evaluation to DUS examination alone.
More validated and reliable suggestions and / or recommendations about nonstandard SVT management will be available after systematic data collection and analysis (Figure 2).
- Di Nisio M, Wichers IM, Middeldorp S. Treatment for superficial thrombophlebitis of the leg. Cochrane Database Syst Rev. 2018; 2: CD004982. | Crossref
- Nasr H, Scriven JM. Superficial thrombophlebitis (superficial venous thrombosis). BMJ. 2015; 350: h2039. | Crossref
- Frappé P, Buchmuller‑Cordier A, Bertoletti L, et al. Annual diagnosis rate of superficial‑vein thrombosis of the lower limbs: the STEPH community‑based study. J Thromb Haemost. 2014; 12: 831‑838. | Crossref
- Decousus H, Epinat M, Guillot K, et al. Superficial vein thrombosis: risk factors, diagnosis and treatment. Curr Opin Pulm Med. 2003; 9: 393‑397. | Crossref
- Leon L, Giannoukas AD, Dodd D, et al. Clinical significance of superficial vein thrombosis. Eur J Vasc Endovasc Surg. 2005; 29: 10‑17. | Crossref
ARTICLE INFORMATION