Human alveolar echinococcosis lesion in the right atrium mimicking a large cardiac thrombus

 CC BY 4.0
CC BY 4.0
Human alveolar echinococcosis lesion in the right atrium mimicking a large cardiac thrombus
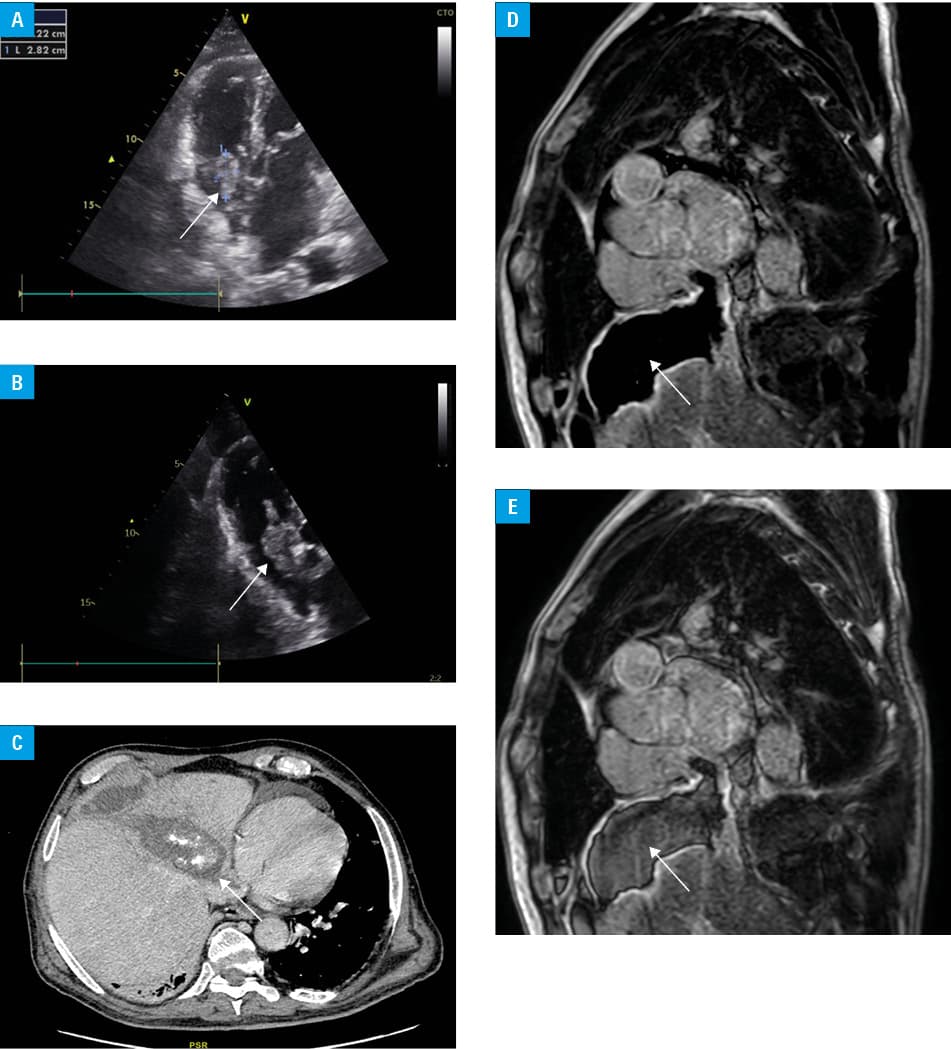
A 69‑year‑old man with hypertension, a biliary prosthesis, and a diagnosis of alveolar echinococcosis (AE) involving the liver and lungs was transferred from an internal medicine department to a cardiology department due to a lesion found in his right atrium. Bedside echocardiography showed an irregular mass (59 mm × 16 mm) originating from the outlet of the inferior vena cava (IVC) and extending into the right atrium (RA), partially obstructing the tricuspid orifice, which raised a suspicion of a large thrombus (Figure 1A and 1B). An urgent consultation with a cardiac surgeon was scheduled, and the patient was referred for conservative treatment with unfractionated heparin (UFH). It was advised to consider thrombolysis in the case of hemodynamic instability. Follow‑up echocardiography after 5 days of UFH treatment showed no regression of the mass. Due to a possibility of an unusual AE invasion, extensive diagnostic imaging was performed, including computed tomography (CT) of the chest and abdomen, as well as both CT and magnetic resonance imaging (MRI) of the heart. Cardiac MRI confirmed a focal lesion measuring 110 mm × 61 mm in the fourth segment of the liver, along with a lesion with an identical signal extending toward the IVC and into the RA, terminating in a spherical structure, approximately 13–14 mm in diameter, which impacted the hemodynamics of the tricuspid valve during the cardiac cycle, resting on the atrial side of the septal leaflet (Figure 1C–1E). We conducted a teleconsultation with the Department of Tropical and Parasitic Diseases in Poznań, a reference center in Poland that treats echinococcosis, to establish an optimal treatment strategy. Extensive surgical treatment, involving both heart and liver transplant, was considered. Unfortunately, after further observation, the patient was deemed to be in a disseminated and likely incurable stage of AE, and he was scheduled for continued conservative treatment with albendazole. He died a few months after hospital discharge.
Human AE caused by Echinococcus multilocularis is considered to be the most lethal zoonosis in the northern hemisphere. Following the introduction of pharmacological treatment with benzimidazoles, patient prognosis has improved, with a shift from a fatality rate of 90% to a survival rate of 88%.1 In Poland, the highest risk of AE is observed in the northeastern regions. Between the years 1990–2011, a total of 121 cases were reported, with a fatality rate of 19%. In all cases, the liver was the primary organ involved, and spread to other organs was noted in 30 patients. A total of 60% of patients underwent surgical treatment, including 15 liver transplants.2 The diagnosis of AE is often made incidentally. Symptoms typically appear in the advanced stages of the disease, and in contrast to an infection with E. granulosus, cysts formed by E. multilocularis frequently resemble a cancerous lesion on imaging. In our case, echogenicity of the mass in the right atrium was similar to that of a thrombus, tumor, as well as the adjacent myocardium wall; therefore, advanced, multimodality cardiac imaging was required for differential diagnosis.3 There are only a few cases documenting cardiac involvement in AE, and successful treatment heavily depends on early presentation and prompt surgical intervention.4,5 In our case, the patient presented with advanced disease that progressed despite albendazole treatment, resulting in multiorgan damage. It is crucial to implement treatment as soon as possible and to consider surgical intervention in the early stages of the disease.
- Kern P, Bardonnet K, Renner E, et al. European echinococcosis registry: human alveolar echinococcosis, Europe, 1982‑2000. Emerg Infect Dis. 2003; 9: 343‑349. | Crossref
- Nahorski WL, Knap JP, Pawłowski ZS, et al. Human alveolar echinococcosis in Poland: 1990‑2011. PLoS Negl Trop Dis. 2013; 7: e1986. | Crossref
- Matusik PS, Mikrut K, Bryll A, et al. Prominent crista terminalis mimicking a right atrial mass: a systematic literature review and meta‑analysis. Acta Radiol. 2024; 65: 588‑600. | Crossref
- Ruze R, Jiang T, Zhang W, et al. Liver autotransplantation and atrial reconstruction on a patient with multiorgan alveolar echinococcosis: a case report. BMC Infect Dis. 2024; 24: 659. | Crossref
- Chernyavskiy A, Alsov S, Guliaeva K, Porshennikov I. The first case of combined heart‐liver transplantation in a patient with alveolar echinococcosis. J Card Surg. 2020; 35: 3199‑3201. | Crossref
ARTICLE INFORMATION