A 63-year-old woman with hypoxemic respiratory failure due to pulmonary arteriovenous malformation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A 63-year-old woman with hypoxemic respiratory failure due to pulmonary arteriovenous malformation
Pulmonary arteriovenous malformations (PAVMs) are rare vascular anomalies characterized by direct connections between pulmonary arteries and veins, leading to right‑to‑left shunts and hypoxemia. Hypoxemia results from a right‑to‑left shunt, whereby blood bypasses the alveolar capillary bed. The magnitude of the shunt proportionally determines the arterial oxygen deficit, while the progressive enlargement of the malformation exacerbates hypoxemia. PAVMs can present asymptomatically or with symptoms, such as dyspnea or cyanosis, and complications, including stroke or brain abscess due to paradoxical emboli.1 They are often associated with hereditary hemorrhagic telangiectasia, but they can occur sporadically.2 Early detection and management are crucial to prevent serious complications.
PAVMs represent an infrequent but clinically pivotal source of hypoxemic respiratory failure. We present a case illustrating diagnostic challenges and management decisions encountered in routine internal medicine practice.
A 63‑year‑old woman with a history of 2 transient ischemic attacks (TIAs; 8 and 10 years earlier), hypertension, heterozygous factor V Leiden mutation (hereditary thrombophilia), thyroidectomy (12 years earlier), and atherosclerosis of the jugular arteries was admitted to a hospital due to epigastric, right‑sided pleuritic chest wall pain, exacerbated by respiration and accompanied by fever. On examination, she exhibited moderate respiratory distress (oxygen saturation, 87%–91%). Cardiovascular and respiratory examinations were otherwise unremarkable. She was diagnosed with pneumonia and treated with ciprofloxacin until the symptoms resolved.
However, due to a sudden onset of symptoms and tachycardia, computed tomography angiography (angio‑CT) was performed, showing embolic material in the right lower lobe pulmonary artery supplying segments VIII, IX, and X, where inflammation was present. Therefore, rivaroxaban was started. Follow‑up angio‑CT performed 4 months later identified a large pulmonary arteriovenous malformation in segment X of the right lung (RL; Figure 1). The patient was discharged with continued follow‑up in a pulmonary clinic and was referred to a cardiologist in relation to the PAVM.
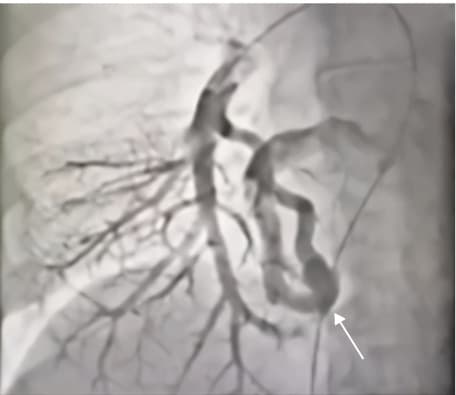
Four years after the episode of pulmonary embolism, the patient was diagnosed with chronic hypoxemic respiratory failure, and was subsequently treated with home oxygen therapy. Because of this, the PAVM was reevaluated via high‑resolution CT of the chest, showing a persistent, large malformation in segment X of the RL, approximately 25 mm × 30 mm in diameter, with a feeding vessel from the segmental artery and drainage into the right lower pulmonary vein. Additionally, partial regression of fibrous scar lesions in segments IX and X of the RL were observed. Pulmonary function tests showed normal spirometry, with moderately reduced diffusing capacity for carbon monoxide (single‑breath diffusion capacity of the lung for carbon monoxide at 52% of the predicted value). Hypoxemic respiratory failure was attributed to the PAVM causing the right‑to‑left shunt.
The patient remains under the supervision of a pulmonary clinic and is managed conservatively. No PAVM embolization has been performed to date.
This case underscores the importance of considering PAVMs in patients presenting with unexplained hypoxemia and a history of thromboembolic events (eg, TIAs). The patient’s pneumonia and / or pulmonary embolism may have contributed to the development or enlargement of the PAVM. Additionally, pneumonia has been reported as a diagnostic trigger that enables the observation of PAVMs, highlighting the need for increased vigilance. In our patient, progressive enlargement of the shunt was potentially closely related to the declining respiratory function, reinforcing the plausible connection between the PAVM size and the severity of hypoxemia. While conservative management was chosen due to the stable condition of the patient, transcatheter embolization is generally recommended for significant PAVMs to reduce the risk of complications, such as paradoxical emboli.3,4 According to the 2018 British Thoracic Society (BTS) Clinical Statement, all radiographically visible PAVMs should be referred to interventional teams experienced in PAVM embolization, even when patients are asymptomatic, because over 25% of them may otherwise experience paradoxical embolic events.5 Importantly, BTS recommends prophylactic antibiotics before dental or surgical procedures to mitigate the risk of cerebral abscess (incorporated into this patient’s care plan).5 BTS also cautions against routine follow‑up CT due to cumulative radiation exposure, and favors clinical, physiological, and chest radiography approximately 6 months after embolization.5
Regular monitoring is essential to assess changes in the size of PAVMs and the patients’ respiratory status, ensuring prompt intervention if the disease progresses.
- Etievant J, Si‑Mohamed S, Vinurel N, et al. Pulmonary arteriovenous malformations in hereditary haemorrhagic telangiectasia: correlations between computed tomography findings and cerebral complications. Eur Radiol. 2018; 28: 1338‑1344. | Crossref
- Scarpato BM, McDonald J, Bayrak‑Toydemir P, et al. The shunt of it. Chest. 2023; 163: e201‑e205. | Crossref
- Maruyama T, Kariya S, Nakatani M, et al. Congenital pulmonary varix: two case reports. Medicine. 2021; 100: e28340. | Crossref
- Lacombe P, Lacout A, Marcy PY, et al. Diagnosis and treatment of pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia: an overview. Diagn Interv Imaging. 2013; 94: 835‑848. | Crossref
- Shovlin CL, Condliffe R, Donaldson JW, et al. British Thoracic Society Clinical Statement on pulmonary arteriovenous malformations. Thorax. 2017; 72: 1154‑1163. | Crossref
ARTICLE INFORMATION