Effectiveness of dietary prehabilitation in patients with gastric, pancreatic, and colorectal cancers: a systematic review
Key words: colorectal cancer, dietary prehabilitation, gastric cancer, pancreatic cancer, prehabilitation in oncology

 CC BY 4.0
CC BY 4.0
Effectiveness of dietary prehabilitation in patients with gastric, pancreatic, and colorectal cancers: a systematic review
Introduction: Gastric, pancreatic, and colorectal cancers pose a serious health challenge, characterized by high morbidity and mortality rates. Dietary prehabilitation, aimed at optimizing nutritional status before treatment, has proven to be a promising strategy for improving outcomes.
Objectives: Our aim was to assess the effectiveness of dietary prehabilitation in improving clinical outcomes, including nutritional status, length of hospital stay, and quality of life in patients with gastric, pancreatic, and colorectal cancers.
Patients and methods: We systematically reviewed randomized controlled trials and observational studies in accordance with the PRISMA guidelines. Electronic databases searched included Embase, CINAHL, Cochrane Central Register of Controlled Trials, Medline, and Google Scholar.
Results: Twelve studies focusing on pretreatment dietary interventions were identified. Dietary prehabilitation, particularly using oral nutritional supplements or immunonutrition, reduced postoperative complications and improved nutritional status, especially in malnourished patients.
Conclusions: Dietary prehabilitation appears to benefit patients with gastric, pancreatic, and colorectal cancers, particularly in terms of postoperative outcomes and nutritional status.
What's new?
This is the first review to synthesize data on the role of dietary prehabilitation focusing on oral nutritional supplements and immunonutrition across 3 major gastrointestinal cancers, that is, gastric, pancreatic, and colorectal cancer. Dietary prehabilitation was associated with reduced postoperative complications and better maintenance of nutritional status, particularly in malnourished patients. Findings highlight the importance of individualized nutrition strategies and suggest future integration with multimodal approaches for improved oncological outcomes.
Introduction
Gastric, pancreatic, and colorectal cancers are significant global health challenges, associated with high incidence and mortality rates. According to the International Agency for Research on Cancer, colorectal cancer is the third most common cancer globally, with over 1.93 million new cases in 2022. Gastric cancer accounts for 1.9 million cases annually, while pancreatic cancer, though less common, has a 5‑year survival rate of under 10%.1 Addressing these malignancies requires innovative strategies to improve patient outcomes.
Oncological prehabilitation aims to enhance patient functional capacity before treatment, unlike traditional rehabilitation, which occurs afterward. Prehabilitation includes interventions such as exercise, psychological support, and nutrition.2-5 Systematic reviews show that prehabilitation can reduce postoperative complications, shorten hospitalization, improve nutritional status, and enhance quality of life (QoL).6-11
Dietary prehabilitation focuses on optimizing the patient nutritional status through tailored interventions, including a supply of proteins, fats, carbohydrates, and immunomodulatory components. It is particularly vital for patients with gastric, pancreatic, and colorectal cancers, who are at a high risk of malnutrition due to metabolic changes, digestive issues, and treatment side effects.12-15
This review evaluates the impact of dietary prehabilitation on clinical outcomes of patients with these cancers, highlighting its role in improving immunity, recovery, and overall prognosis.
Patients and methods
This narrative systematic review followed the 2020 PRISMA guidelines.16 It was registered with PROSPERO (CRD42024577926), an international prospective systematic review database.
Eligibility criteria
Both observational studies and randomized controlled trials (RCTs) published in English were included, with no publication date restrictions. We used the following inclusion criteria: 1) population: adult patients with gastric, pancreatic, or colorectal cancer (any stage) before anticancer treatment; 2) intervention: dietary prehabilitation (any type, duration, and form), including nutritional supplementation but excluding other prehabilitation forms; 3) comparison: standard care (no intervention or placebo); 4) outcomes: nutritional status (assessed by any method), QoL (any method), and length of hospital stay (LOS; any method).
Exclusion criteria encompassed “grey literature,” such as conference materials, theses, government documents, brochures, newsletters, annual reports, blogs, podcasts, newspaper articles, case reports, and study protocols.
Information sources and search strategy
The search included Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Controlled Trials, Medline, and Google Scholar. Free‑text queries and built‑in thesauri (eg, MeSH in Medline, EmTree in Embase) were used. Initially, the searches had no time or language restrictions. However, only the papers in English were included in the final review. A follow‑up search was performed to incorporate the latest studies, ensuring a comprehensive review of nutritional prehabilitation impact on cancer patient outcomes.
A comprehensive search strategy was developed to identify relevant studies. Various combinations of keywords and Boolean operators were used to ensure a wide range of studies were captured (Supplementary material, Table S1).
This strategy aimed to capture the breadth of literature addressing dietary prehabilitation and its effects on outcomes, such as changes in nutritional status, LOS, and QoL in cancer patients. The search was conducted between August 20 and September 30, 2024. The review was updated on December 7, 2024.
Study selection process
Two reviewers (DG and MW) independently reviewed titles and abstracts of the relevant studies. For papers that appeared to meet the inclusion criteria, full‑text versions were assessed to determine eligibility for final inclusion in the systematic review. At each stage of the selection process, any differences between the reviewers were resolved through discussion and mutual agreement.
Study risk of bias assessment
The risk of bias was assessed using the Cochrane RoB2 tool for randomized trials, covering 5 domains: randomization, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported outcomes. The criteria were categorized as entailing “low,” “moderate,” or “high” risk of bias.17 For 1 non‑RCT study, the QUADAS‑2 tool was applied to evaluate patient selection, diagnostic tests conducted, reference standards, and study flow.18
Data collection process and data elements
Screening and data extraction were conducted by 2 independent reviewers (DG and MW) using Covidence software (www.covidence.org, Veritas Health Innovation Ltd., Melbourne, Australia). The extracted data included study details (authors, year, study design, follow‑up duration), population characteristics (sample size, country, cancer stage, malnutrition risk, sex, age, planned therapy, treatment duration), intervention characteristics (duration, dosing, type), and reported outcomes (weight, body mass index [BMI], nutritional status, muscle mass, grip strength, physical function, QoL, complications, C‑reactive protein [CRP] levels, LOS, readmission, and mortality).
Study selection
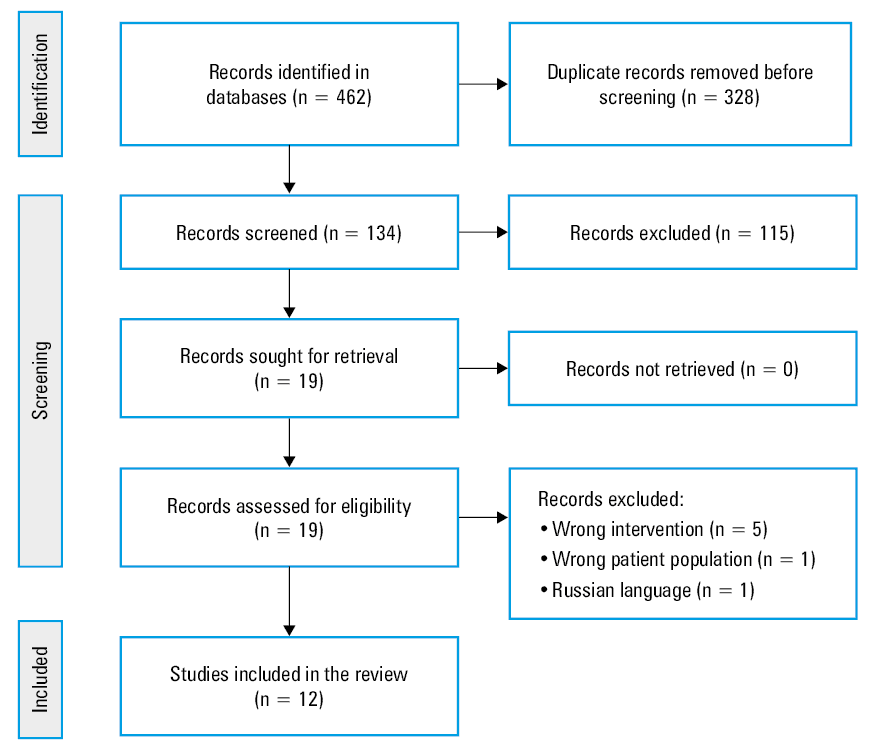
The study selection process, presented in the 2020 PRISMA flowchart (Figure 1), identified 462 records. After removing duplicates and evaluating 19 articles, 7 were excluded for not meeting the inclusion criteria (ie, population, intervention, or language). Ultimately, 12 studies, including 1 observational study and 11 RCTs, were analyzed. Studies involving multimodal prehabilitation, nonmalignant gastrointestinal diseases, or cancer recurrence were excluded.
Ethics
Due to the retrospective design of the study, no approval of an ethics committee and patient consent were necessary.
Results
Characteristics of the included studies
In Tables 1, 2, 3 we summarize the nutritional interventions before oncological treatment, highlighting heterogeneity in cancer stages and profiles. Colorectal cancer patients dominated (6 studies), followed by gastric (4 studies) and pancreatic cancers (2 studies). Commonly assessed outcomes included LOS and general postoperative complications, for example, infectious, gastrointestinal, or postoperative wound–related, while muscle mass, grip strength, physical fitness, and QoL were less frequently evaluated.
Authors, year, and country | Type of study and population | Intervention | Duration of intervention | Length of observation | Measured outcomes | Results |
Abbreviations: ALB, albumin; CON, control group; CRP, C‑reactive protein; EN, enteral nutrition; GPC, general postoperative complications; IC, infectious complications; IF, immune function; IL, interleukin; INT, intervention group; IRI, inflammatory reaction indicator; LOS, length of hospital stay; ONS, oral nutritional supplementation; PA, prealbumin; PG‑SGA, Patient‑Generated Subjective Global Assessment; QoL, quality of life; RCT, randomized controlled trial; RR, risk ratio; SSI, surgical site infection | ||||||
Fujitani et al,19 2012, Japan | RCT; 244 patients undergoing elective total gastrectomy for gastric cancer
INT, n = 127
CON, n = 117 |
| 5 d before surgery | From the time of surgery to the discharge from the hospital, which corresponded to an average of 17–18 d | SSI | RR, 1.09 (95% CI, 0.66–1.78) |
IC | RR, 1.11 (95% CI, 0.59–2.08) | |||||
CRP | P = 0.11 | |||||
LOS | P = 0.4 | |||||
Wang et al,20 2015, China | RCT; 200 patients with gastric cancer treated with radical surgery
INT, n = 100
CON, n = 100 |
| 7 d before surgery and continued until day 9 after surgery | 10 d before surgery and 10 d after surgery | ALB | Higher in INT (P <0.05) |
PA | Higher in INT (P <0.05) | |||||
IF | CD4+/CD8+ higher in INT (P = 0.03) | |||||
IRI | CRP lower in INT (P = 0.03), IL‑6 lower in INT (P = 0.02) | |||||
Kong et al,21 2018, South Korea | RCT; 127 gastric cancer patients
INT, n = 65
CON, n = 62 |
| 14 d before surgery and continued for 28 d after surgery (a total of 42 days) | 35 d after surgery | GPC | Lower in INT (P = 0.02) |
PG‑SGA | Grade C, lower in INT (P = 0.04) | |||||
LOS | No significant difference (P = 0.4) | |||||
QoL | No significant difference (P = 0.82) | |||||
Li et al,22 2024, China | RCT; 136 patients with locally advanced gastric cancer, planned for neoadjuvant chemotherapy followed by radical gastrectomy
INT, n = 68
CON, n = 68 |
| 49–63 d before chemotherapy | 77–91 d after chemotherapy | GPC | Lower in INT (P = 0.02) |
ALB | Higher in INT (P < 0.001) | |||||
PA | Higher in INT (P = 0.01) | |||||
LOS | Shorter in INT (P = 0.003) | |||||
Authors, year, and country | Type of study and population | Intervention | Duration of intervention | Length of observation | Measured outcomes | Results |
Abbreviations: BW, body weight; FC, functional capacity; IQR, interquartile range; POS, prospective observational study; others, see Table 1 | ||||||
Gade et al,23 2016, Denmark | RCT; n = 35 patients scheduled for elective surgery for pancreatic cancer
INT, n = 19
CON, n = 16 |
| 7 d before surgery | 30 d after surgery | GPC | No significant difference (P = 0.5) |
LOS | Shorter in INT, but not significant (P = 0.17) | |||||
FC | No significant difference | |||||
BW | No significant difference | |||||
Bibby et al,24 2023, United Kingdom | POS; n = 137 patients scheduled for pancreatic cancer surgery | – | – | Patients monitored from the time of diagnosis until 12 months after surgery | GPC | 17.5% of patients had complications |
PG‑SGA | Higher need for intervention postsurgery (90.6%) but improved at 6–12 months (26.4%) | |||||
BW | 76.7% lost ≥5% postsurgery | |||||
LOS | Median 12 days (IQR, 3–49) | |||||
Authors, year, and country | Type of study and population | Intervention | Duration of intervention | Length of observation | Measured outcomes | Results |
Burden et al,25 2011, United Kingdom | RCT; 125 patients scheduled for elective curative surgery for colorectal cancer
INT, n = 59
CON, n = 66 |
| 10 d before surgery (condition for inclusion in the study) | 84 d after surgery | GPC | No significant difference (P = 0.78) |
IC | No significant difference (P = 0.27) | |||||
LOS | No significant difference | |||||
Maňásek et al,26 2016, Czech Republic | RCT; 157 patients with colorectal cancer
INT, n = 52
CON, n = 105 |
| 10 d before surgery and for 14 d after surgery | 168 d after surgery | GPC | Lower rates of wound dehiscence (RR, 0.45), wound infection (RR, 0.23), and anastomotic dehiscence (RR, 0.5) in INT |
BMI | Higher in INT before and after surgery (P = 0.01) | |||||
BW | Lower postoperative weight loss in INT, no data for CON | |||||
LOS | Shorter in INT (P = 0.002) | |||||
Gillis et al,27 2016, Canada | RCT; 43 patients with nonmetastatic colorectal cancer awaiting elective surgery
INT, n = 22
CON, n = 21 |
| 28 d before surgery and 28 d after surgery | 28 d after surgery | GPC | No significant difference (P = 0.75) |
FC | 6MWD similar between groups (P = 0.83) | |||||
QoL | No significant difference (P = 0.76) | |||||
Burden et al,28 2017, United Kingdom | RCT; 101 patients with colorectal cancer
INT, n = 55
CON, n = 46 |
| The intervention lasted from the time the patient was randomized to the day before surgery. The average duration of supplement use was 8 d. | 30 d after surgery | GPC | No significant difference (P = 0.11) |
SSI | Lower in INT (P = 0.04) | |||||
BW | Less postoperative weight loss in INT (P = 0.02) | |||||
LOS | No significant difference (P = 0.63) | |||||
Tesar et al,29 2023, Czech Republic | RCT; 120 patients scheduled for elective colorectal cancer surgery
INT, n = 60
CON, n = 60 |
| 7 d before surgery | 30 d after surgery | GPC | No significant difference (P = 0.73) |
PBC | No significant difference in muscle strength (upper limbs, P = 0.56; lower limbs, P = 0.58) | |||||
ALB | No significant difference (P = 0.09) | |||||
PA | P = 0.46 | |||||
LOS | No significant difference (P = 0.85) | |||||
Lee, et al,30 2023, South Korea | RCT; 161 patients with primary colorectal cancer, scheduled for elective colorectal cancer surgery
INT, n = 79
CON, n = 82 |
| 7 d before surgery | 30 d after surgery | GPC | No significant difference (P = 0.74) |
ALB | No significant difference (P = 0.84) | |||||
IC | No significant difference (P = 0.75) | |||||
BW | Better weight maintenance in INT (P = 0.002) | |||||
LOS | No significant difference (P = 0.63) | |||||
Risk of bias
The risk of bias in the included RCTs was assessed using the Cochrane RoB2 tool (Supplementary material, Table S2). Some concerns were identified in most of the studies, with 3 rated as having a high risk of bias due to deviations from interventions, selective reporting, or outcome measurement issues. Overall, the studies were of high quality. One non‑RCT study was evaluated using the QUADAS‑2 tool, and the risk of bias was assessed as low.
Main findings
Dietary prehabilitation in patients diagnosed with gastric cancer
A study involving 244 patients with gastric cancer who underwent gastrectomy and received 1000 ml/day of oral nutritional supplementation (ONS) found no significant differences in the incidence of surgical site infections (relative risk [RR], 1.09; 95% CI, 0.66–1.78) or LOS (P = 0.4), as compared with the control group.19 In contrast, in a study involving 200 patients with gastric cancer undergoing radiotherapy and receiving 1000 kcal/day of ONS, Wang et al20 reported significant improvements in serum albumin (P <0.05) and prealbumin levels (P <0.05), and a reduction in inflammatory markers, including a significant decrease in CRP levels in the intervention group (P = 0.03), as compared with controls. Similarly, in a study of 127 patients undergoing gastrectomy and receiving 500 ml/day of ONS, Kong et al21 observed a lower overall postoperative complication rate in the intervention than the control group (P = 0.02). Severely malnourished patients (Patient‑Generated Subjective Global Assessment [PG‑SGA], grade C) particularly benefited from ONS, showing fewer major complications and better weight maintenance. A study of 136 gastric cancer patients undergoing chemotherapy and receiving 500 ml/day of ONS, reported a lower rate of postoperative complications, particularly pulmonary infections, in the intervention group (P = 0.02), as well as a significantly shorter LOS among those receiving ONS during neoadjuvant chemotherapy (P <0.001) than in the control group.22
Dietary prehabilitation in patients diagnosed with pancreatic cancer
In a study by Gade et al,23 35 patients undergoing surgery for pancreatic cancer received a 7‑day course of oral immunonutrition (500 ml/day). Although the reduction in postoperative complications was not significant, the intervention group had a significantly shorter median LOS than the control group (11 vs 16 d).23 In a prospective observational study by Bibby et al,24 137 patients undergoing surgery for pancreatic cancer received individually tailored nutritional support (oral, enteral, or parenteral) from the time of cancer diagnosis. Although 76.7% of the patients still lost at least 5% of their body weight within 1 month after surgery, they gained an average of 1.8% of their preoperative body weight during the prehabilitation period. Moreover, both their nutritional status (as assessed by the PG‑SGA) and handgrip strength improved prior to surgery.24
Dietary prehabilitation in patients diagnosed with colorectal cancer
A study involving 125 patients undergoing surgery for colorectal cancer25 found that ONS combined with dietary counseling (for at least 10 d preoperatively) reduced the incidence of wound infections among patients who experienced postoperative weight loss. However, no significant differences were observed in the LOS. Similarly, Maňásek et al,26 in a study of 157 patients undergoing colorectal cancer surgery who received 250 ml/day of high‑protein ONS for 10–14 days preoperatively, reported that ONS administration both before and after surgery resulted in fewer postoperative infections (RR, 0.45), shorter LOS (9.4 vs 12 d; P = 0.002), and reduced treatment costs in the intervention group. In a study by Gillis et al,27 which included 43 patients receiving 1.2–1.5 g/kg/day of high‑protein ONS for 28 days prior to colorectal cancer surgery, the intervention group showed a significant improvement in preoperative walking capacity (6‑minute walk distance [6MWD]; P = 0.02), although no significant postoperative differences were found (P = 0.76). In another study by Burden et al,28 involving 101 patients receiving 250 ml/day of ONS before colorectal surgery, the use of ONS was associated with a reduction in postoperative infections (30% in the intervention group vs 47% in the control group) and smaller weight loss in the intervention group (P = 0.02). Conversely, Tesar et al,29 in a study of 127 patients undergoing total colectomy who received 125 ml of high‑protein ONS twice daily, found no significant differences in in‑hospital mortality, muscle mass, or patient independence, highlighting the need for further research into long‑term recovery outcomes. Finally, Lee et al30 studied 161 patients undergoing colorectal cancer surgery. The intervention group received 250 ml/day of immunonutrition ONS for 7 days preoperatively, while the control group received a standard diet. The authors reported that immunonutrition significantly improved weight recovery 1 month after discharge (P = 0.002), but had no significant effect on postoperative complication rates (P = 0.74).
Discussion
This narrative systematic review synthesizes findings from 11 RCTs and 1 observational study on dietary prehabilitation in gastrointestinal cancers. The included studies were heterogeneous. Unfortunately, there is a limited number of studies on unimodal interventions (nutritional support), as most authors focus on multimodal programs.6-11
It was established that dietary prehabilitation, particularly involving ONS and immunonutrition, was associated with a reduction in postoperative complications and an improvement in nutritional status, especially among malnourished patients.
The European Society for Clinical Nutrition and Metabolism recommends nutritional risk screening within 48 hours of hospital admission, with preoperative nutritional interventions for malnourished or high‑risk patients.31 A review conducted by Looijaard et al32 aimed to assess the effectiveness of physical and nutritional prehabilitation in patients aged at least 60 years old undergoing elective surgery for colorectal cancer. The authors suggest that nutritional and physical prehabilitation may be most beneficial for malnourished individuals who are at a higher risk of complications.
Overall, available studies and reviews show substantial variability in the effects of dietary prehabilitation across different types of gastrointestinal cancers.19-30,33-35
Effectiveness of dietary prehabilitation in gastric cancer
Patients with gastric cancer are particularly prone to malnutrition and cachexia due to tumor location, which hampers food intake and nutrient absorption.36 Our review suggests that immunonutrition and ONS offer moderate benefits, especially for high‑risk, malnourished patients. Wang et al20 reported that immunonutrition improved albumin and prealbumin levels while lowering inflammatory markers (interleukin‑6, tumor necrosis factor α), potentially reducing postoperative complications associated with inflammation. Although no significant reduction in complications was found, benefits may be more evident in higher‑risk groups.19 An interesting aspect seems to be the implementation of multimodal prehabilitation. A Lithuanian RCT37 found that a multimodal prehabilitation program (including diet, psychological support, physiotherapy, smoking cessation) lowered complication risk by 60% within 90 days and improved QoL (RR, 0.4).
Difficulties related to food tolerance persist,38 as some patients are unable to tolerate certain oral formulations.21,39 In such cases, specialized enteral or parenteral nutrition may be more effective. Overall, immunonutrition and ONS can improve surgical outcomes in gastric cancer; however, standardized interventions and further research are needed to optimize composition of the formulations and individualize treatment based on nutritional status.
Effectiveness of dietary prehabilitation in pancreatic cancer
Pancreatic cancer is among the most aggressive gastrointestinal malignancies, often accompanied by advanced malnutrition at diagnosis.40 While dietary prehabilitation, particularly immunonutrition, shows potential benefits, such as shorter LOS and improved nutritional status, data remain limited and inconsistent.23,24 Gade et al23 reported a 5‑day reduction in LOS with immunonutrition, though not significant due to a small sample size. De Luca et al14 highlighted slight reductions in postoperative infections and LOS with medical nutrition, stressing proactive support for severe malnutrition.
Bibby et al24 observed modest preoperative weight gain with dietary support, yet 76.7% of patients lost at least 5% of body weight within a month postsurgery. A study by Christopher et al41 on the effect of exercise and nutritional interventions in patients with liver, pancreatic, and biliary tract cancer and a systematic review42 on multimodal prehabilitation in patients with pancreatic cancer showed that the combination of nutritional interventions and physical exercise improves postoperative outcomes and may prolong survival in pancreatic and related cancers. Future research should optimize formulations and delivery methods, including specialized enteral or parenteral regimens, to address cachexia and malabsorption in pancreatic cancer patients.42
Effectiveness of dietary prehabilitation in colorectal cancer
Dietary prehabilitation, particularly with ONS and immunonutrition, benefits colorectal cancer patients who often face malnutrition and increased complication risks.31,43 Burden et al25,28 showed that preoperative ONS reduced the incidence of wound infections and weight loss in malnourished patients. A review on multimodal prehabilitation3 reported a 24.91‑meter increase in the 6MWD and fewer postoperative complications (RR, 0.27). Gillis et al44 found that nutritional prehabilitation shortened LOS by 2 days, improved 6MWD, and lowered complication rates, though small sample size limited conclusions.
Immunonutrition, including arginine and ω-3 fatty acids, also shows promise. Lee et al30 found it helped to maintain body weight postdischarge, though it did not significantly reduce overall infection rates. A meta‑analysis of 12 RCTs45 investigating the use of immunonutrition to reduce the rate of postoperative infectious complications in patients with colorectal cancer showed a reduction in wound infections (44%) and systemic infections (56%), while enhancing the immune response of CD16+ and CD56+ cells. Ural et al46 showed that supplements enriched with arginine, ω-3 fatty acids, and nucleotides improved weight, BMI, arm circumference, and reduced inflammation.
However, variations in interventions, doses, and durations make comparisons challenging. Standardized protocols and larger trials are essential to confirm long‑term benefits.
Prospects for new therapeutic strategies
Dietary prehabilitation shows potential for patients with gastrointestinal cancers, particularly pancreatic, gastric, and colorectal malignancies. Future approaches may focus on personalized interventions addressing nutritional deficits and metabolic status, guided by biomarkers and advanced screening tools.47 Tailored diets enriched with amino acids (eg, arginine, glutamine) and multimodal programs combining nutrition, exercise, and psychological support demonstrate synergistic benefits.3,8,10,13,14
Immunonutrition, incorporating ω-3 fatty acids, nucleotides, and probiotics, could reduce inflammation and improve gut health.9,14,19,20,23,40,45,46 For severe malabsorption or advanced disease, specialized enteral or parenteral nutrition may ensure adequate intake.31,39,46 Nutrigenomics offers potential for precision interventions aligned with genetic and metabolic profiles.48
Extending nutritional support beyond surgery could enhance recovery, prevent muscle wasting, and improve survival. Clinical trials are needed to validate and standardize these strategies for broader patient groups.
For internal medicine physicians, early identification of malnutrition in oncology patients is crucial. These patients should be referred to a clinical dietitian for the implementation of personalized dietary prehabilitation.
Strengths and limitations
This review encompasses diverse studies on gastric, pancreatic, and colorectal cancers, highlighting various nutritional interventions (eg, oral supplements, immunonutrition) and outcomes such as complications, nutritional status, muscle mass, QoL, and LOS. The inclusion of studies from multiple countries (Japan, China, Denmark, United Kingdom) enhances global applicability.
Due to substantial heterogeneity in the interventions, populations, and outcome measures, a meta‑analysis was not conducted. The findings are presented as a narrative systematic review, grouped by cancer type and clinical outcome indicators. It is also important to consider patient lifestyle factors, including alcohol consumption, as potential modifiers of the effectiveness of dietary prehabilitation. Alcohol may negatively impact nutritional status, metabolic functions, and immune response, which could ultimately limit the effectiveness of the intervention.
Heterogeneity in study populations, cancer stages, and intervention protocols limits the ability to draw definitive conclusions. Small sample sizes reduce statistical power, while the absence of blinding introduces potential bias particularly in subjective outcomes, such as QoL. Short follow‑up periods hinder evaluation of long‑term benefits, and the predominant focus on well‑nourished patients may obscure potential advantages for malnourished individuals. Additionally, inconsistent outcome measures further complicate cross‑study comparisons.
Conclusions
This systematic review suggests that dietary prehabilitation, particularly based on ONS and immunonutrition, may improve postoperative complications, recovery times, and nutritional status in patients with gastric, pancreatic, and colorectal cancers. Despite these promising indications, variability in study populations and methods, small sample sizes, lack of blinding, and brief follow‑up periods limit definitive conclusions. Larger, more rigorous trials with standardized outcomes are needed to establish the long‑term effectiveness of nutritional prehabilitation in oncology.
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024; 74: 229‑263. | Crossref
- Ligibel JA, Bohlke K, May AM, et al. Exercise, diet, and weight management during cancer treatment: ASCO guideline. J Clin Oncol. 2022; 40: 2491‑2507. | Crossref
- Molenaar CJ, van Rooijen SJ, Fokkenrood HJ, et al. Prehabilitation versus no prehabilitation to improve functional capacity, reduce postoperative complications and improve quality of life in colorectal cancer surgery. Cochrane Database Syst Rev. 2023; 5: CD013259. | Crossref
- Daniels SL, Lee MJ, George J, et al. Prehabilitation in elective abdominal cancer surgery in older patients: systematic review and meta‑analysis. BJS Open. 2020; 4: 1022‑1041. | Crossref
- Meneses‑Echavez JF, Loaiza‑Betancur AF, Díaz‑López V, et al. Prehabilitation programs for individuals with cancer: a systematic review of randomized‑controlled trials. Syst Rev. 2023; 12: 219. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION