A patient with Loeys–Dietz syndrome double-seropositive for antiglomerular basement membrane and antineutrophil cytoplasmic antibodies

 CC BY 4.0
CC BY 4.0
A patient with Loeys–Dietz syndrome double-seropositive for antiglomerular basement membrane and antineutrophil cytoplasmic antibodies
Patients with concomitant antiglomerular basement membrane (anti‑GBM) and antineutrophil cytoplasmic antibodies (ANCAs) remain a therapeutic challenge.1 Although data are limited, evidence suggests that ANCA vasculitis develops first and triggers the production of anti‑GBM antibodies, resulting in pulmonary and renal manifestations.2 Exposure to GBM antigens may result in the production of atypical anti‑GBM antibodies, targeting components other than α3 chain of type IV collagen, and an atypical ANCA pattern with a predominance of antiproteinase 3 antibodies.3 The presence of both anti‑GBM antibodies and ANCAs has been reported to increase the risk of severe complications, including end‑stage kidney disease.
Loeys–Dietz syndrome (LDS) is a rare connective tissue disease, with prevalence estimated at 1:50 000. Mutations in genes encoding transforming growth factor β receptors (TGFβRs) or their ligands have been shown to be implicated in the pathogenesis of this disorder.4 Due to impaired TGFβ signaling, patients with LDS are at a high risk of valvular and cardiac defects, arterial complications (particularly aneurysms and dissections throughout the arterial tree), and autoimmune disorders of the respiratory and gastrointestinal tracts.4 In the available literature, we found only 1 case report presenting the coincidence of anti‑GBM antibodies and ANCA‑negative crescentic glomerulonephritis related to aortic graft infection in a patient with LDS.5
We present a case of a 34‑year‑old woman with type 2 LDS (confirmed TGFβR2 mutation) and a history of bicuspid aortic valve and aortic root replacement surgery (7 years ago), who reported hemoptysis for 2 months before hospitalization.
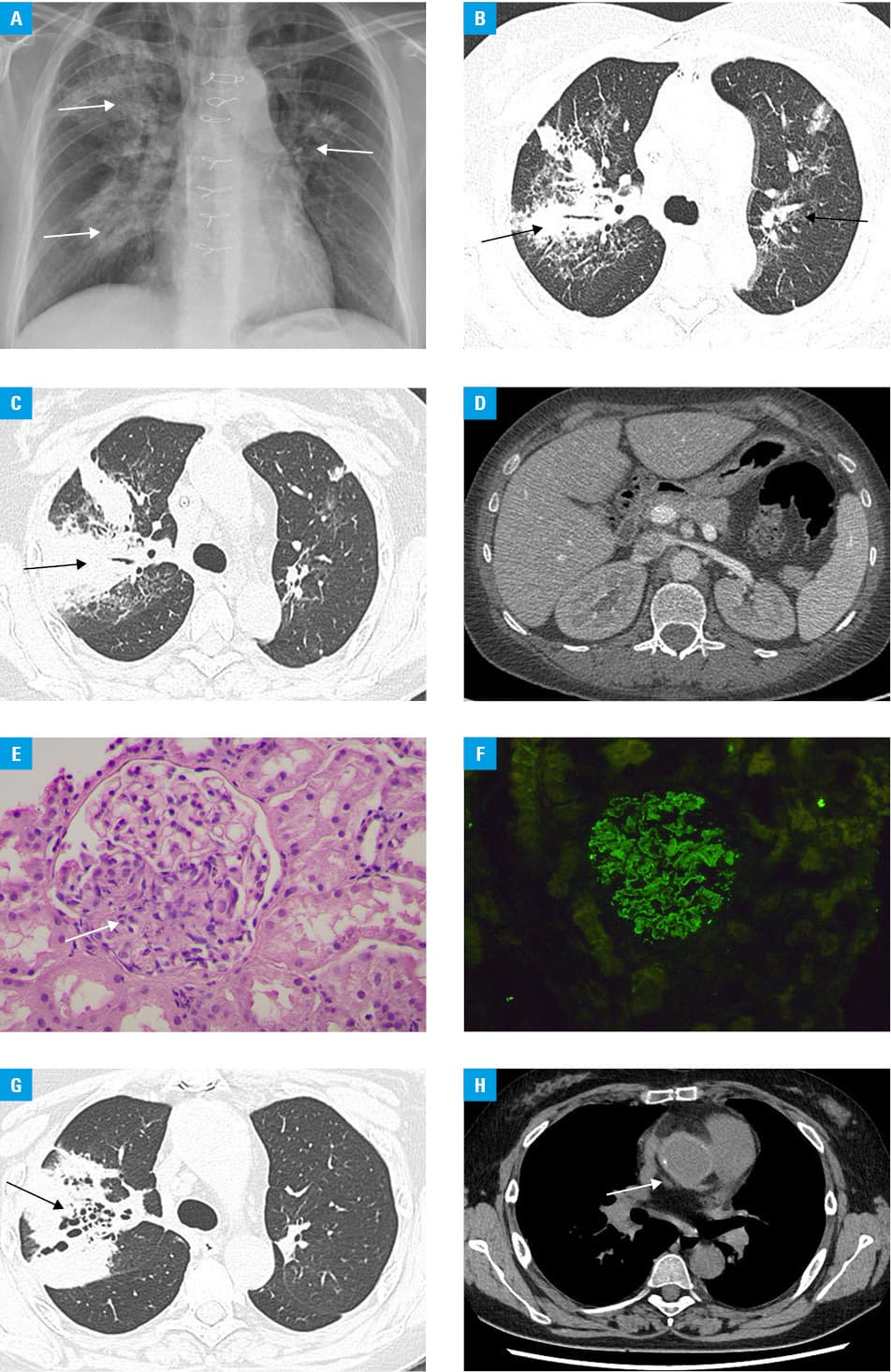
On admission, the patient presented with erythrocyturia and proteinuria, normal kidney function (serum creatinine concentration of 0.81 mg/dl; reference range <0.95 mg/dl), elevated levels of inflammatory markers, and diffuse alveolar hemorrhage visualized on X‑ray and computed tomography imaging (Figure 1A–1C), which was confirmed on bronchoscopy. Kidney size was within the normal range (Figure 1D). Immunological tests showed the presence of anti‑GBM antibodies and proteinase 3 ANCA. Due to the progression of renal damage, kidney biopsy was performed, showing proliferation of Bowman capsule cells (crescents; Figure 1E), normal interstitium, positive linear immunofluorescent staining for immunoglobulin G and complement component 3 (Figure 1F), segmental foot process effacement with local GBM rupture, and presence of deposits within the GBM on electron microscopy. Treatment involved administration of methylprednisolone, followed by oral prednisone, and intravenous cyclophosphamide (a total dose of 2520 mg). Simultaneously, 9 therapeutic plasma exchanges were performed but were complicated by severe immunoglobulin and fibrinogen deficiencies requiring their substitution. Broad‑spectrum antibiotic and antifungal treatments were initiated. After 4 months, the treatment required intensification due to the progression of lung involvement (Figure 1G) and suspected aortic graft infection (Figure 1H). After 6 months of multitargeted therapy, the patient had stable kidney function (serum creatinine, 0.95 mg/dl), mild proteinuria and erythrocyturia, and no pulmonary manifestations of vasculitis.
Patients who are double‑seropositive for anti‑GBM antibodies and ANCAs require multidisciplinary treatment and careful monitoring for potential disease‑related complications. No need for kidney replacement therapy may predict favorable kidney outcomes in such individuals.
- Shin JIl, Geetha D, Szpirt WM, et al. Anti‑glomerular basement membrane disease (Goodpasture disease): from pathogenesis to plasma exchange to IdeS. Ther Apher Dial. 2022; 26: 24‑31. | Crossref
- Ge Y, Zhu J, Yang G, et al. Clinical characteristics and outcome of double‑seropositive patients with anti‑glomerular basement membrane antibodies and anti‑neutrophil cytoplasmic antibodies. Int Immunopharmacol. 2024; 138: 112607. | Crossref
- Levy JB, Hammad T, Coulthart A, et al. Clinical features and outcome of patients with both ANCA and anti‑GBM antibodies. Kidney Int. 2004; 66: 1535‑1540. | Crossref
- MacCarrick G, Black JH, Bowdin S, et al. Loeys‑Dietz syndrome: a primer for diagnosis and management. Genet Med. 2014; 16: 576‑587. | Crossref
- Zhou X‑J, Liu L‑J, He P‑X, Zhou F. Glomerulonephritis triggered by chronical aortic graft infection in a male with Loeys‑Dietz syndrome: a case report. Medicine (Baltimore). 2019; 98: e15496. | Crossref
ARTICLE INFORMATION