Uptake of 18F-labeled prostate-specific membrane antigen-1007 in a patient with metastatic pheochromocytoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Uptake of 18F-labeled prostate-specific membrane antigen-1007 in a patient with metastatic pheochromocytoma
We present a case of a 59‑year‑old man with progressive metastatic adrenal pheochromocytoma. The patient had no significant family history of genetic disorders, and his pheochromocytoma was deemed sporadic in origin. Three years prior, he underwent radical nephrectomy and adrenalectomy, and his disease began progressing 1 year ago. Recently, he exhibited no significant response following targeted therapies including sunitinib, bevacizumab, and 131I‑metaiodobenzylguanidine (MIBG). A multidisciplinary team recommended multigene mutation testing; however, the patient declined due to financial constraints, as the cost was not covered by his medical insurance. Computed tomography (CT) was performed. Positron emission tomography (PET)/CT imaging with 68Ga‑labeled somatostatin analogues (68Ga‑DOTA‑SSA) has become the cornerstone for staging and follow‑up of metastatic pheochromocytomas and paragangliomas, establishing its role besides 123I‑MIBG single photon emission CT in theranostics to evaluate eligibility for targeted radionuclide therapy.1 Due to limited availability of 68Ga‑DOTA‑SSA radiopharmaceuticals in our local clinical setting, alternative agents were substituted for this study. Previous incidental observation has suggested the potential expression of prostate‑specific membrane antigen (PSMA) in isolated pheochromocytomas.2 Moreover, a recent study documenting PSMA overexpression in a subset of pheochromocytomas and paragangliomas inspired us to investigate PSMA‑based theranostics for this patient.3 We reviewed the patient’s histopathological findings. Microscopically, the tumor exhibited a classic “zellballen” architecture, composed of well‑circumscribed nests of neoplastic cells surrounded by delicate fibrovascular stroma. The tumor cells displayed polygonal to spindle‑shaped morphology, with abundant granular eosinophilic cytoplasm and round to oval nuclei showing mild to moderate pleomorphism. Scattered sustentacular cells, accentuated by S100 immunostaining, were peripherally distributed around the tumor nests. The tumor cells showed strong and diffuse immunoreactivity for chromogranin A and synaptophysin, confirming neuroendocrine differentiation. The Ki‑67 proliferation index was 5%. Immunohistochemical analysis of the adrenal pheochromocytoma tissue demonstrated that PSMA was expressed by the endothelial cells within the tumor vasculature, rather than by the tumor cells themselves (Figure 1A), aligning with previous findings.3
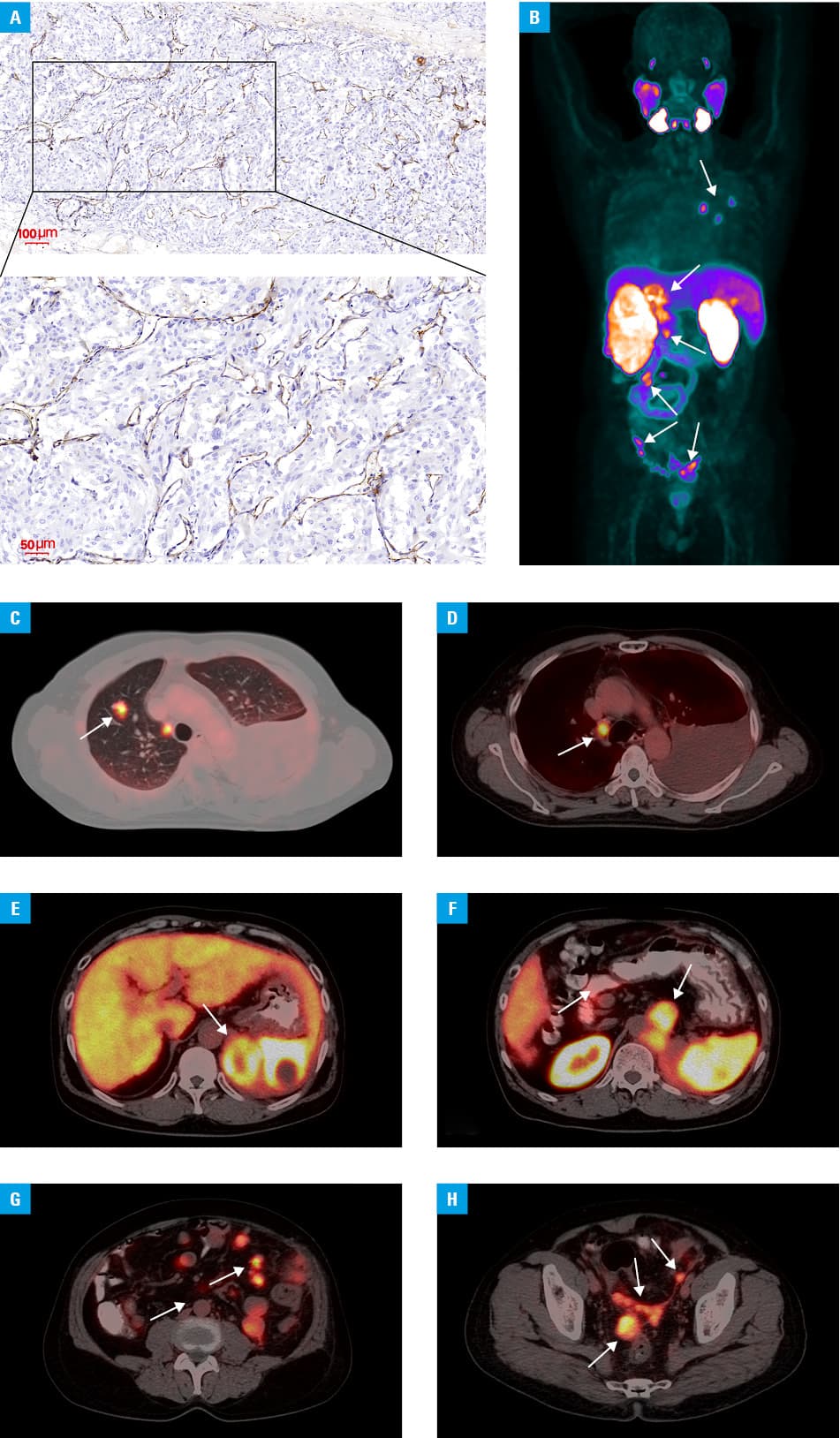
In pursuit of alternative theranostic options, an 18F‑PSMA‑1007 PET/CT scan was performed (Figure 1B). It showed PSMA‑avid recurrence and metastases involving the right lung (Figure 1C), mediastinal lymph nodes (Figure 1D), the surgical site (Figure 1E), the retroperitoneum (Figure 1F), and abdominal and pelvic peritoneal deposits (Figure 1G and 1H). Unfortunately, the patient’s condition deteriorated rapidly, and he died of multiorgan failure before further therapeutic interventions could be attempted.
The expression of PSMA in tumor‑associated neovasculature has broadened the utility of PSMA‑PET imaging across various solid tumors beyond prostate cancer.4,5 Our findings demonstrate pronounced PSMA avidity in metastatic lesions of adrenal pheochromocytoma, suggesting a potential role for PSMA‑targeted radioligand therapy even in the cases of widespread metastases. This approach could potentially facilitate the implementation of theranostic anti‑PSMA radioconjugates targeting the tumor vascular endothelial cells in selected patients with metastatic adrenal pheochromocytoma. Further clinical studies are warranted to validate the therapeutic efficacy of this approach.
- Taïeb D, Jha A, Treglia G, et al. Molecular imaging and radionuclide therapy of pheochromocytoma and paraganglioma in the era of genomic characterization of disease subgroups. Endocr Relat Cancer. 2019; 26: R627‑R652. | Crossref
- Singh D, Kumar R, Mittal BR, et al. 68Ga‑labeled prostate‑specific membrane antigen uptake in pheochromocytoma: an incidental finding in PET/CT scan. Clin Nucl Med. 2018; 43: 688‑690. | Crossref
- Vit O, Patel M, Musil Z, et al. Deep membrane proteome profiling reveals overexpression of prostate‑specific membrane antigen (PSMA) in high‑risk human paraganglioma and pheochromocytoma, suggesting new theranostic opportunity. Molecules. 2021; 26: 6567. | Crossref
- Sasikumar A, Joy A, Nanabala R, et al. (68)Ga‑PSMA PET/CT imaging in primary hepatocellular carcinoma. Eur J Nucl Med Mol Imaging. 2016; 43: 795‑796. | Crossref
- Shetty D, Loh H, Bui C, et al. Elevated 68Ga prostate‑specific membrane antigen activity in metastatic non‑small cell lung cancer. Clin Nucl Med. 2016; 41: 414‑416. | Crossref
ARTICLE INFORMATION