Extended anticoagulation in patients with cancer-associated venous thromboembolism
Key words: anticoagulation, cancer, direct oral anticoagulation, thrombosis, venous thromboembolism



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Extended anticoagulation in patients with cancer-associated venous thromboembolism
Cancer‑associated thrombosis (CAT) presents a major clinical burden, impacting both survival and quality of life in patients with malignancy. While direct oral anticoagulants (DOACs) and low‑molecular‑weight heparin are recommended for initial treatment, decisions on extending anticoagulation beyond 6 months remain complex due to variable recurrence and bleeding risks. This comprehensive review explores contemporary strategies for long‑term CAT management, focusing on risk stratification, guideline evolution, and individualized patient‑centered care. We highlight the importance of cancer type, disease status, and patient comorbidities—such as renal dysfunction and thrombocytopenia—in guiding therapy duration. Recent studies suggest that reduced‑dose DOAC regimens, particularly apixaban, may have favorable safety profiles without compromising efficacy, offering a potential shift in secondary prevention paradigms. Nonetheless, bleeding risks remain significant, and validated tools for predicting long‑term venous thromboembolism recurrence or hemorrhagic complications are lacking. We advocate for the creation of dedicated cancer thrombosis clinics to support shared decision‑making and tailored management, particularly for frail or high‑risk populations. Finally, we propose a research agenda targeting challenging subgroups—such as patients with brain tumors, gastrointestinal malignancies, or extremes of weight—to refine anticoagulation strategies and improve outcomes. The future of CAT care demands more precise, patient‑centered approaches grounded in evolving science, clinical nuance, and patient preference.
Introduction
Cancer‑associated thrombosis (CAT) remains a significant challenge, affecting approximately 20% of cancer patients and representing the second leading cause of mortality after cancer progression in this population.1,2 Thus, patients with cancer have a 4- to 9‑fold greater risk of venous thromboembolism (VTE).3-5 Moreover, CAT has an amplified mortality risk of more than 2‑fold, as compared with cancer patients without VTE, with worse overall outcomes if VTE is present early in the disease.6-8 Selection of appropriate anticoagulation is imperative to reduce additional complications, as CAT can delay anticancer therapy, cause repeated or extended hospitalization, and impact the quality of life.9 Among patients with cancer, the thrombosis risks are amplified by malignancy‑related hypercoagulability, chemotherapy, cancer‑related surgery, central venous catheters, and immobility.10,11 While the advent of direct oral anticoagulants (DOACs) has simplified the anticoagulation management in the acute phase and initial 6 months of treatment, uncertainties persist regarding the optimal duration of therapy, especially in the context of advanced cancer and metastatic disease.12 Moreover, patients with cancer also have an increased bleeding risk; the annual major bleeding risk affects approximately 1 in 10 patients.13 Multiple hemostatic mechanisms are tightly intertwined in cancer progression, chemotherapy, and anticoagulation. Therefore, understanding the risk factors for CAT recurrence and CAT‑related bleeding helps to inform and individualize management decision‑making.
For the treatment of CAT during the first 6 months, both low‑molecular‑weight heparin (LMWH) and DOACs are recommended as first‑line options.12,14-16 LMWH remains an appropriate choice, particularly in patients with luminal gastrointestinal and genitourinary malignancies to reduce bleeding risk, while DOACs, such as apixaban, edoxaban, and rivaroxaban are effective alternatives.17 Warfarin remains a secondary option reserved for cases where LMWH or DOACs cannot be used.17,18 Treatment should continue for a minimum of 6 months, with regular reassessment to guide ongoing management. There are evolving data to be reconciled regarding options to modify care after the first 6 months of treatment. In this review, we summarize the critical considerations in determining anticoagulation, with a focus on extended (after 6 months) anticoagulation duration for CAT, focusing on risk stratification, treatment strategies, and guideline recommendations to assist clinicians in making informed decisions.
Risk stratification in cancer‑associated thrombosis after initial treatment
CAT, as a leading cause of cancer‑related mortality, requires careful risk stratification to optimize anticoagulation duration while minimizing recurrent thrombotic events and bleeding complications (Figure 1). Various factors play a role in this risk assessment, such as patient characteristics (age, comorbidities, genetics), cancer type (tumor site, stage, metastatic status), and ongoing treatments (surgery, chemotherapy, immunotherapy, central venous catheters) as well as the presence of thrombophilia—particularly antiphospholipid syndrome.19-22
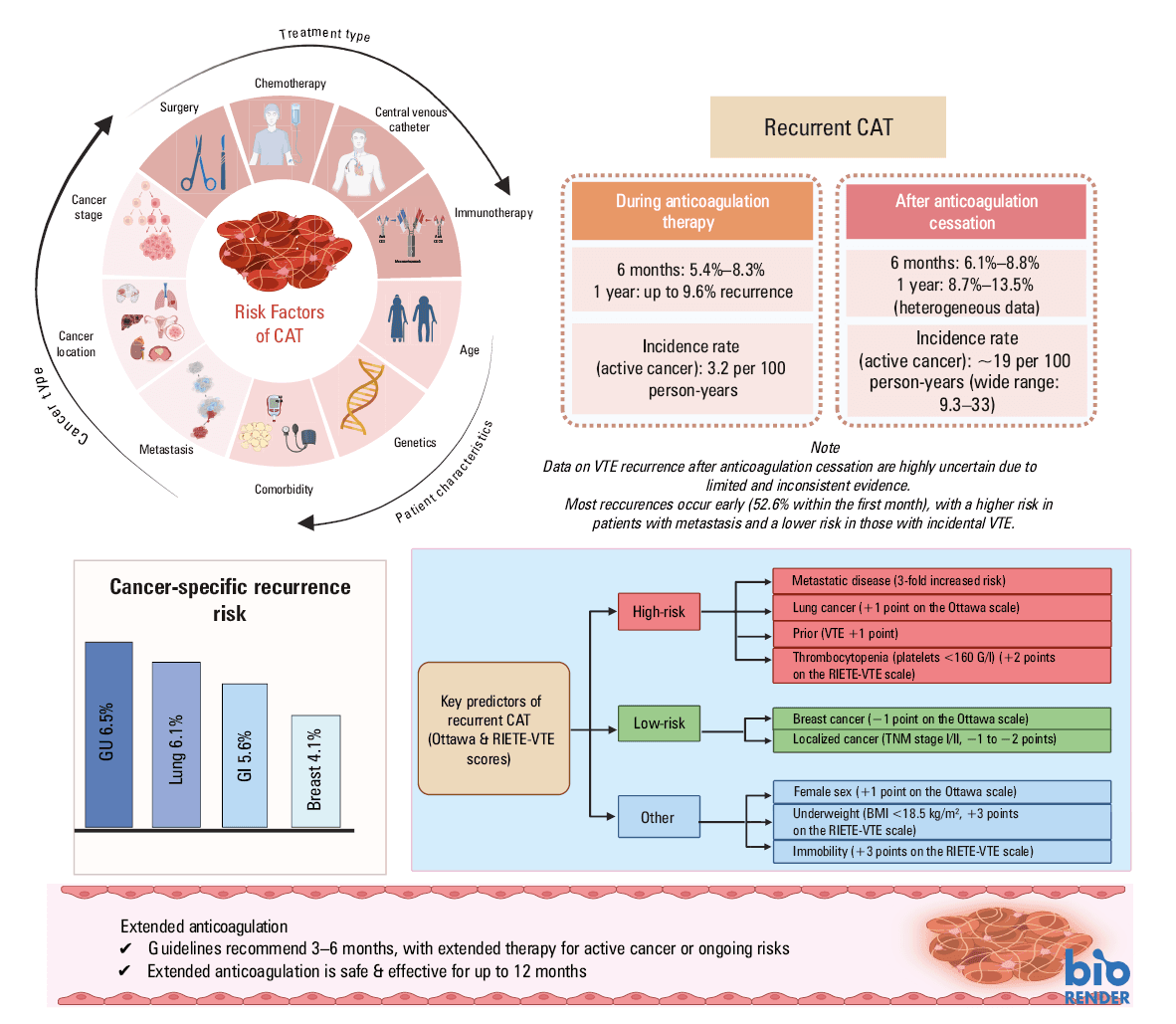
Abbreviations: BMI, body mass index; CAT, cancer‑associated thrombosis; GI, gastrointestinal; GU, genitourinary, VTE, venous thromboembolism
The recent guidelines of the European Society for Medical Oncology (ESMO)15 recommend systematic assessment of CAT risk in newly‑diagnosed patients with cancer as well as in ambulatory patients on anticancer therapy using the Khorana risk score,23 the COMPASS‑CAT model,24 or the Vienna‑CAT score.25 Patients scheduled for abdominal oncological surgery are recommended to receive systematic postoperative pharmacological treatment with LMWH. The Caprini score26 is recommended for VTE risk evaluation in patients scheduled for any nonabdominal oncological surgery. In multiple cohorts, the type of cancer is a major predictor of thrombosis. Thus, the highest incidences are observed in pancreatic and brain cancer, followed by lung, gynecological, and colorectal cancer, with lower values in breast and prostate cancer.27,28 Mechanistically, variables such as tissue factor, podoplanin, neutrophil extracellular traps, plasminogen activator inhibitor‑1, and certain gene mutations may contribute to an increased risk of CAT in specific cancer types.29-33 More recently, polygenic risk scores—based on the analysis of germline single‑nucleotide polymorphisms—have also been shown to predict the incidence of CAT.34 In a study leveraging the United Kingdom Biobank data, polygenic risk stratification identified 13% of individuals with a genetic risk for CAT equivalent to or greater than that conferred by factor (F) V or prothrombin mutations.35
Yet, after CAT has occurred, predicting recurrence on and off anticoagulation remains a challenge. In the first 6 months of treatment, recurrence rates while on anticoagulation range from approximately 4% to 9.6%, with a risk modified by cancer type, disease burden, and anticoagulant used.33,36-38 Thus, in a population‑based cohort study of all Olmsted County, Minnesota, United States, comprising 1533 person‑year follow‑up, brain, lung, and ovarian cancers, myeloproliferative or myelodysplastic disorders were independently associated with an increased risk for VTE recurrence.39 Whether CAT was provoked or unprovoked, it also has been associated with recurrence, whereas outflow obstruction and liver metastases predicted a higher anticoagulation failure rate.39,40 Then, after stopping anticoagulation, the risk of recurrent VTE remained substantial, especially in the first 90 days, during which incidence rate was reported as high as 14.6 per 100 person‑years. This risk gradually declined but did not normalize, particularly in patients with active malignancy.41 The Cancer DACUS (Residual Vein Thrombosis and the Optimal Duration of Low Molecular Weight Heparin in Cancer Patients With Deep Vein Thrombosis) study42 showed that residual vein thrombosis (RVT) may help predict the risk of VTE recurrence in cancer patients after 6 months of treatment with LMWH. Patients without RVT had a very low recurrence rate (2.9%) after stopping LMWH, while those with RVT had a higher recurrence risk, regardless of whether they continued or stopped anticoagulation.42 While these findings require replication for validation, RVT could be a useful marker to guide decisions on whether to provide extended anticoagulation in CAT.
While anticoagulation extended beyond 6 months is supported by available data in patients with active or advanced cancer, it must be weighed against the elevated risk of bleeding, which is consistently higher in cancer than noncancer populations. Major bleeding can occur at rates exceeding 15 per 100 person‑years in patients with extensive malignancy, particularly among those with gastrointestinal cancers, prior bleeding events, anemia, or low albumin levels.38,43 Although bleeding rates beyond 6 months of therapy appear comparable to those observed in the initial period (3%–5.5% in most studies), the cumulative risk underscores the need for careful monitoring and potentially safer anticoagulation options in the long term.38,44,45 Importantly, even in studies where the overall benefit of extended anticoagulation was unclear (eg, Cancer DACUS, COMMAND VTE Registry), recurrence remained high—up to 35% at 5 years—particularly in those who discontinued anticoagulation despite persistent cancer.46,47
Although some of the determinants governing CAT recurrence have been identified, risk prediction remains challenging. Validated tools for long‑term risk stratification for CAT recurrence or bleeding have limited clinical utility. Although extensively used, the Ottawa score shows poor discrimination in identifying recurrence risk.48 This score was developed to stratify the risk for recurrent VTE in CAT during the first 6 months of anticoagulation.45 The original version categorizes patients into low (≤0) and high (≥1) risk based on the cancer type, stage, sex, and prior VTE, while the modified version refines the risk into 3 groups—low (≤−1), intermediate (0), and high (≥1)—by adjusting the weight of early‑stage cancers and adding further granularity.49 In this large validation study involving 11 123 patients from the RIETE registry, the modified Ottawa score showed only modest ability to predict VTE recurrence in cancer patients, with a C‑statistic of 0.58 and limited sensitivity and specificity across risk groups. Given its poor performance, the score is not reliable for guiding clinical decisions, underscoring the need for a new model that incorporates additional or alternative predictors.50 Conversely, in a recent post hoc analysis of the ONCO DVT (Optimal Duration of Anticoagulation Therapy for Isolated Distal Deep Vein Thrombosis in Patients With Cancer Study), extended 12‑month edoxaban treatment reduced thrombotic events, as compared with 3‑month treatment in cancer patients with isolated distal vein thrombosis (DVT) who had intermediate or high modified Ottawa scores, but not in those with low scores. These findings suggest that extended anticoagulation may be most beneficial in patients with higher predicted risk, while offering limited advantage for those classified as low‑risk.51 These data indicate some utility of this scoring tool in selected groups.
More recent efforts, including a machine learning model by Muñoz et al52 and a regression‑based tool by Lanting et al,53 have identified factors such as primary pulmonary embolism, metastatic disease, and DVT at presentation as predictors, yet these models achieve only modest predictive power (area under the curve of about 0.66). There is also limited guidance on balancing bleeding and thrombotic risk over time. Notably, bleeding events in this population are strongly associated with increased mortality—nearly 6‑fold in some cohorts—highlighting the critical need for refined tools and safer, more personalized anticoagulation strategies. Until such models are validated, decisions regarding extended anticoagulation should remain guided by a composite of patient characteristics, cancer activity, bleeding risk, and patient preference.
Evidence for extended therapy and guidelines position
Advances in oncology, including immunotherapy and targeted treatments, have extended patient survival and increased the incidence of VTE, underscoring the need for long‑term anticoagulation strategies that safely reduce bleeding risk while maintaining efficacy. Optimizing the duration of anticoagulation in CAT requires careful balancing the prevention of VTE recurrence with minimizing hemorrhagic complications. Both LMWH and DOACs remain viable options, as supported by clinical trials and guidelines14-16 that increasingly emphasize individualized patient care and novel information on dosing reduction as a care alternative.
Extended low‑molecular‑weight heparin therapy
Extended LMWH therapy is effective over longer periods of time. A prospective, multicenter DALTECAN trial (Evaluation of Dalteparin for Long‑term [One Year] Treatment of Blood Clots in Subjects With Cancer), enrolled patients with CAT treated with subcutaneous dalteparin for 12 months. Among 109 of 334 individuals who completed 12 months of therapy, the VTE recurrence rate was 4.1% during months 7–12.54 Notably, there was a dose reduction strategy to approximately 150 IU/kg per day, from months 2 to 12. Concordantly, in TiCAT (Tinzaparin in Cancer Associated Thrombosis Beyond 6 Months), a prospective, single‑arm multicenter study of 247 patients with CAT treated with tinzaparin, a reduction in recurrence from 4.5% to 1.1% with subcutaneous tinzaparin (175 IU/kg daily) for 12 months was seen.55 Clinically relevant bleeding remained low and stable between months 7 and 12 (0.6%) per patient‑month. Moik et al56 conducted a systematic review that specifically confirmed bleeding rates of 1%–4% with long‑term LMWH therapy, thus substantiating its tolerability. For patients with active cancer or remnants of DVT, LMWH continues to be a solid choice, confirming its position paved by the CLOT (Randomized Comparison of Low‑Molecular‑Weight Heparin versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) trial.57
Extended direct oral anticoagulant therapy
The SELECT‑D trial (Anticoagulation Therapy in Selected Cancer Patients at Risk of Recurrence of Venous Thromboembolism) was the first to demonstrate that rivaroxaban reduced VTE recurrence to 4% after 6 months (vs 14% on placebo), although the trial was limited by a relatively small sample size.36 The ONCO‑PE trial (Optimal Duration of Anticoagulation Therapy for Low‑risk Pulmonary Embolism Patients With Cancer) in Japan randomized 178 patients with CAT to 6 or 18 months of rivaroxaban (15 mg daily) and achieved substantially reduced VTE recurrence on prolonged anticoagulation (odds ratio, 0.25, 95% CI, 0.1–0.7) with no measured increase in the risk of major bleeding.58 In the Hokusai VTE Cancer trial, edoxaban was compared with dalteparin in CAT, and patients were treated for up to 12 months. In a post hoc analysis of the trial, in the patients continuing treatment beyond 6 months, the composite outcome of recurrent VTE or major bleeding between months 6 and 12 occurred in 2.4% of edoxaban users and 2.2% of those on dalteparin (hazard ratio [HR], 1.05; 95% CI, 0.4–3.1). Recurrent VTE and major bleeding rates were low and similar between groups.59,60
Attention to dose was evaluated in 2 recent studies. In the EVE trial (Apixaban in Preventing Secondary Cancer Related Venous Thrombosis in Cancer Patients Who Have Completed Anticoagulation Therapy), in 360 cancer patients with prior VTE, low‑dose apixaban (2.5 mg twice daily) showed similar safety and efficacy to standard‑dose apixaban (5 mg twice daily) during extended anticoagulation over 12 months. Rates of bleeding (8.9% vs 12.2%), recurrent VTE or arterial thrombosis (5% in both groups), and all‑cause mortality (13% vs 12%) were comparable.61
The intensity of the antithrombotic treatment determines the benefit / risk ratio for the extended anticoagulation in patients with CAT.
A multicenter, randomized, double‑blind, noninferiority API‑CAT trial (Study for Apixaban Cancer Associated Thrombosis) compared the efficacy and safety of apixaban at a reduced (2.5 mg twice daily) or full dose (5 mg twice daily) for 12 months in 1766 patients with active cancer and acute VTE who had completed at least 6 months of anticoagulation.62 The patients with major bleeding accounted for 3.8% of the reduced‑dose group and 4.1% of the full‑dose group. Median (interquartile range) treatment duration was 11.8 (8.3–12.1) months. Recurrent VTE occurred in 18 patients (cumulative incidence, 2.1%) in the reduced‑dose group and in 24 (cumulative incidence, 2.8%) in the full‑dose group (adjusted subhazard ratio, 0.76; 95% CI, 0.41–1.41; P = 0.001 for noninferiority). Clinically relevant bleeding occurred in 102 patients (cumulative incidence, 12.1%) in the reduced‑dose group and 136 (cumulative incidence, 15.6%) in the full‑dose group (adjusted subhazard ratio, 0.75; 95% CI, 0.58–0.97; P = 0.03). Mortality was 17.7% in the reduced‑dose group and 19.6% in the full‑dose group (adjusted HR, 0.96; 95% CI, 0.86–1.06). Extended anticoagulation with reduced‑dose apixaban was noninferior to full‑dose apixaban for the prevention of recurrent VTE in the patients with active cancer. The reduced dose led to a lower incidence of clinically relevant bleeding complications, as compared with the full‑dose regimen. These findings support the use of lower dose apixaban, 2.5 mg twice daily, for secondary prevention of VTE in patients with active cancer.62
Moreover, Larsen et al63 found that reduced‑dose apixaban after 6 months of ongoing treatment was safe, as very low rates of recurrent VTE and major bleeding were seen after 12 months. In aggregate, these findings suggest that extended anticoagulation strategies with a dose‑reduction approach may offer a favorable balance between the prevention of recurrent thrombosis and the risk of bleeding in CAT patients who require long‑term treatment.
While DOAC dose reduction for extended anticoagulation has not been studied in all scenarios, clinical judgement remains essential. It is critical to carefully evaluate individual patients who were usually excluded from trials in which even with dose‑reduction regimens, their bleeding risk may be prohibitive beyond 6 months, such as those with severe liver disease (eg, Child–Pugh class C liver cirrhosis), significant drug‑to‑drug interactions, recent major bleeding or surgery, history of intracranial bleeding, or limited life expectancy.
The American Society of Hematology (ASH),12 American Society of Clinical Oncology,64 ESMO,15 and the International consensus Statement14 recommend an initial 3–6‑month anticoagulation with extended therapy for active cancer or continued risk factors (ie, recurrent VTE, residual DVT). ASH recommends discontinuation for patients with unstable cancer in remission, recent life‑threatening hemorrhage, active gastrointestinal malignancies, or those who are close to end‑of‑life, emphasizing the patient‑centered approach. The results of the API‑CAT trial62 are expected to change the practice regarding the intensity of the antithrombotic treatment in secondary prevention of CAT, since low‑dose apixaban (2.5 mg twice daily) is safer and as effective as the therapeutic‑dose regimen.
Patient‑centered decision‑making and advocating for cancer thrombosis clinics
CAT is associated with significant morbidity, increased rate of hospitalizations, interfering and / or delaying potentially curative therapies for cancer, such as surgeries or other invasive procedures; often leading to low quality of life.65 Yet, poor awareness and knowledge about its diagnosis and treatment often limit timely CAT prevention and access to care.65
Given the complexity of CAT, the patient‑centered approach—ideally within a specialized CAT clinic—can help guide the nuanced, individualized decisions needed for optimal care. Management extends beyond thrombosis alone, as patients often face intersecting pathological, pharmacological, economic, and psychosocial challenges. Decisions such as the duration of anticoagulation, intensity of the antithrombotic treatment, or whether to use a DOAC or LMWH frequently fall into areas of clinical uncertainty, where high‑quality evidence is limited. In these cases, shared decision‑making is essential, grounded in ethical principles that prioritize patient autonomy, safety, and fairness.66
While DOACs are widely recommended, LMWH remains the preferred option in patients with unresected gastrointestinal or genitourinary cancers due to higher bleeding risks.14,67 Yet, the burden of daily injections—often associated with distress or reduced quality of life—calls for compassionate, tailored discussions that weigh patient preferences alongside clinical risks. Indeed, when queried, patients prefer an oral over parenteral anticoagulant therapy.68 Adherence rates are higher among cancer patients managed with oral anticoagulants.69 To better support this process, there is a pressing need for improved patient‑reported outcome measures specific to CAT. Such tools will help ensure care aligns with what matters most to patients, especially in areas where evidence leaves room for interpretation.
Challenges in interruption and discontinuation
Bleeding risk in patients with CAT remains a major clinical challenge, regardless of whether LMWHs or DOACs are used.70-72 Both classes of anticoagulants present unique safety concerns, influenced by cancer‑specific factors, such as primary tumor site (eg, unresected gastrointestinal or genitourinary malignancies), stage, and progression, as well as patient comorbidities, including thrombocytopenia, renal or hepatic dysfunction, invasive procedures, and potential drug‑drug interactions with anticancer therapies. A recent meta‑analysis of over 3600 patients showed that while DOACs reduced VTE recurrence as compared with LMWHs, they were associated with a higher risk of clinically relevant nonmajor bleeding, particularly in high‑risk tumor types.73 Importantly, bleeding complications are not uncommon, with major bleeding rates reaching 4.3% at 6 months in certain high‑risk groups. However, no externally validated bleeding risk prediction model exists for CAT, requiring clinicians to rely on individual assessments incorporating modifiable factors and shared decision‑making.
In this context, managing CAT demands a multidisciplinary, patient‑centered approach that accounts for the delicate balance between thrombosis prevention and bleeding risk. The risk of thrombosis recurrence and the risk of bleeding may rapidly change during the cancer trajectory. Both are influenced by cancer evolution, aggressiveness, and responsiveness to the anticancer therapies. Some anticancer agents, particularly the most modern targeted anticancer therapies, multiply the risk of CAT.74 On the other hand, anemia, thrombocytopenia, renal insufficiency, and liver dysfunction are among the primary bleeding risk factors that influence the choice of the optimal antithrombotic agent.
Risk assessment must include individualized consideration of cancer status, anticoagulant pharmacodynamics,75 and functional status. In patients with limited life expectancy or prior major bleeding, guidelines increasingly support anticoagulation discontinuation, especially in palliative setting.71,72 Furthermore, perioperative and periprocedural management of DOACs in CAT remains an evolving area with limited data, requiring careful evaluation of cancer- and procedure‑specific risks. The coexistence of CAT and chronic kidney disease (CKD) presents another major gap in evidence, particularly in advanced CKD or dialysis‑dependent patients, where DOAC safety and efficacy data are scarce.76,77 While apixaban is often favored, more prospective studies are needed to support anticoagulation strategies in this complex subgroup. There is limited information on the use of DOACs in patients with cancer and severe liver disease. For cancer patients with Child–Pugh scale C cirrhosis, LMWH should likely be the preferred agent.78 Ultimately, better predictive tools, including bleeding risk scores and patient‑reported outcomes, are urgently needed to guide treatment duration and intensity in this high‑risk population. Table 1 displays specific clinical scenarios while considering LMWHs, DOACs, or VKAs for extended anticoagulation therapies in CAT.
Clinical scenario | Anticoagulation strategy |
Abbreviations: AF, atrial fibrillation; APLS, antiphospholipid syndrome; CKD, chronic kidney disease; DOAC, direct oral anticoagulant; ESLD, end‑stage liver disease; ESRD, end‑stage renal disease; HIT, heparin‑induced thrombocytopenia; LMWHs, low‑molecular‑weight heparins; RRT, renal replacement therapy; VKA, vitamin K antagonist; others, see Figure 1 | |
GI postsurgical malabsorption / post‑Whipple surgery (pancreaticoduodenectomy) | Consider LMWHs; careful consideration of DOACs and monitor drug levels |
Nonresectable luminal GI, GU, or gynecological malignancies | Consider LMWHs; avoid DOACs |
Postgastrectomy | Consider LMWHs; carefully consider DOACs and monitor drug levels |
Valvular AF | Consider LMWHs; avoid DOACs |
Thrombotic APLS | Consider LMWHs, consider VKAs; avoid DOACs |
Drug‑to‑drug interactions (eg, ketoconazole, clarithromycin, phenytoin, rifampin, carbamazepine) | Consider LMWHs; avoid DOACs |
Prior history of thrombotic HIT | Avoid LMWHs; consider DOACs |
Prior history of recurrent CAT/VTE | Consider either LMWHs or DOACs; avoid VKAs |
ESLD/Child–Pugh class C liver cirrhosis | Consider LMWHs; avoid DOACs and VKAs |
Advanced CKD Stage IV/V/ESRD on RRT | Consider DOACs; carefully consider LMWHs and monitor drug levels |
Future perspectives in the treatment of cancer‑associated thrombosis
Despite significant advances in the use of LMWHs and DOACS, particularly FXa inhibitors, for the treatment of CAT, important clinical gaps remain. As a result, there is a critical need for safer anticoagulants that maintain efficacy while minimizing the bleeding risk. A promising area of research is the development of FXI/XIa inhibitors, a novel class of anticoagulants designed to inhibit thrombosis without significantly impairing hemostasis.79,80 These agents target the intrinsic coagulation pathway, specifically FXI, which plays a key role in pathological clot formation but appears to be less essential for normal hemostasis. Preclinical models and early‑phase trials have suggested that FXI/XIa inhibitors may successfully decouple thrombosis from bleeding risk.81-83
Abelacimab, a once‑monthly subcutaneous FXI inhibitor, has emerged as a promising agent in anticoagulation, showing significantly lower rates of major and clinically relevant nonmajor bleeding, as compared with rivaroxaban in the phase 2 AZALEA‑TIMI 71 trial (Safety and Tolerability of Abelacimab [MAA868] vs Rivaroxaban in Patients with Atrial Fibrillation), which enrolled patients with atrial fibrillation.84 Building on these results, 2 ongoing phase 3 trials—ASTER (A Study Comparing Abelacimab to Apixaban in the Treatment of Cancer‑associated VTE) and MAGNOLIA (A Study Comparing Abelacimab to Dalteparin in the Treatment of Gastrointestinal / Genitourinary Cancer and Associated VTE)—are evaluating abelacimab in CAT, with MAGNOLIA specifically focusing on patients with gastrointestinal and genitourinary cancers with a high bleeding risk. If successful, these studies may support the use of FXI inhibitors as a safer, more convenient alternative to existing therapies in CAT, especially in high‑risk or frail populations.85
Significant unmet needs remain—particularly for frail patients and those with renal impairment, who are often excluded from trials and lack tailored treatment options. As other FXI/XIa inhibitors progress through clinical pipelines, future research must prioritize these vulnerable subgroups to ensure that novel therapies deliver broad, equitable benefits. Improving predictive tools and integrating safer anticoagulants into individualized care pathways will be essential to advancing outcomes in complex CAT populations. Table 2 shows high‑bleeding risk CAT patients in which FXI/XIa inhibitors may deserve further investigation.
Abbreviations: AC, anticoagulation; DAPT, dual antiplatelet therapies; others, see Figure 1 |
|
Conclusions
The core challenge in CAT management is balancing the ongoing risk of recurrence with major bleeding, especially after the first 6 months of anticoagulation. While extended therapy with DOACs, such as apixaban, remains effective, uncertainties persist around duration, dosing, and safety in high‑risk groups.
Emerging therapies, such as FXI inhibitors, may offer safer alternatives, particularly for frail or renally‑impaired patients. Until then, individualized care—ideally delivered through specialized thrombosis clinics—must prioritize patient preferences, shared decision‑making, and continual reassessment. The future of CAT care lies in more precise, patient‑centered strategies that evolve with both science and the person behind the diagnosis.
- Lyman GH. Venous thromboembolism in the patient with cancer: focus on burden of disease and benefits of thromboprophylaxis. Cancer. 2011; 117: 1334‑1349. | Crossref
- Heit JA, Spencer FA, White RH. The epidemiology of venous thromboembolism. J Thromb Thrombolysis. 2016; 41: 3‑14. | Crossref
- Khorana AA, Francis CW, Culakova E, et al. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007; 110: 2339‑2346. | Crossref
- Heit JA, Silverstein MD, Mohr DN, et al. Risk factors for deep vein thrombosis and pulmonary embolism: a population‑based case‑control study. Arch Intern Med. 2000; 160: 809‑815. | Crossref
- Mulder FI, Horvàth‑Puhó E, van Es N, et al. Venous thromboembolism in cancer patients: a population‑based cohort study. Blood. 2021; 137: 1959‑1969. | Crossref
ARTICLE INFORMATION