A 75‑year‑old man, Fitzpatrick skin type II, with advanced ascending colon cancer (T4 N2b M1) harboring a BRAF V600E mutation, developed an extensive eruption of over 200 melanocytic nevi approximately 2 months after initiating combined therapy with encorafenib (BRAF inhibitor) and cetuximab (epidermal growth factor receptor [EGFR] inhibitor). The lesions appeared predominantly on the trunk and upper extremities. Videodermatoscopy showed multiple newly‑formed melanocytic nevi, and 2 epigastric lesions were excised for histologic evaluation (Figure 1A–1D).
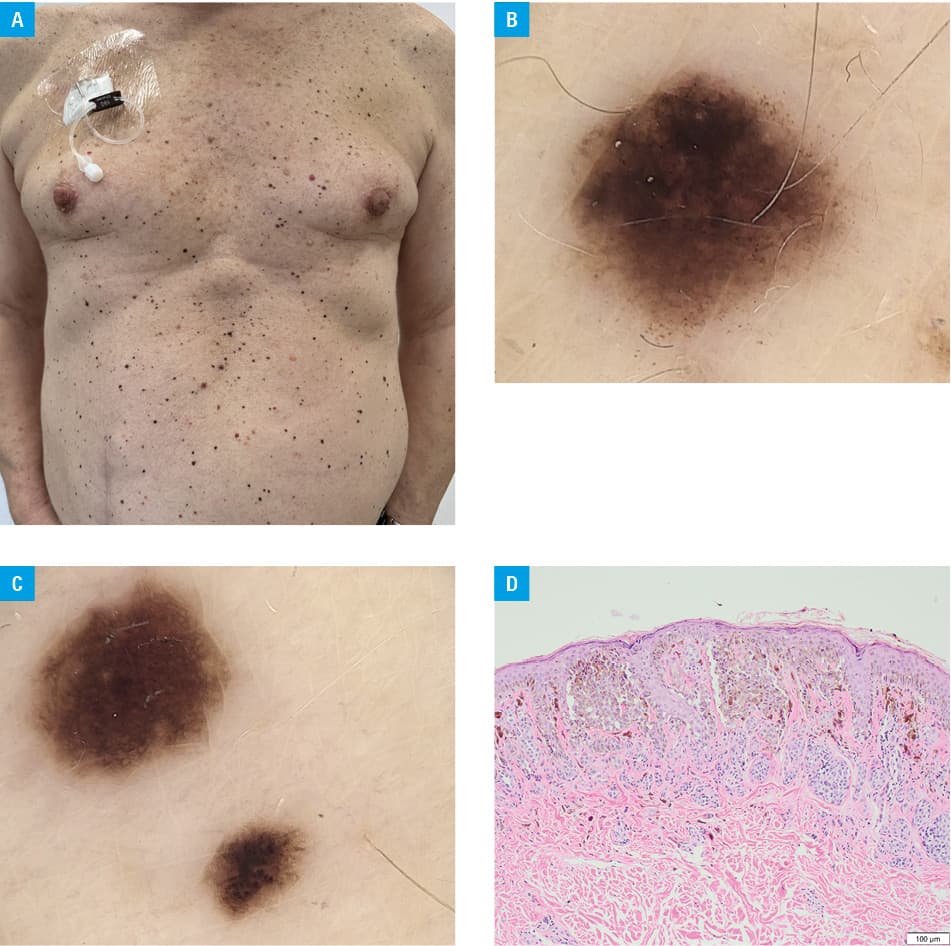
Histopathologic examination demonstrated compound pigmented lesions with mild dysplasia in the basal layer of the epidermis, without malignant transformation. Immunohistochemistry for BRAF V600E (clone VE1) confirmed absence of the V600E mutation. The differential diagnosis included drug‑induced lentigines (timing and histology were inconsistent) and eruptive Spitz nevi (which would show epithelioid nests on histology). Given the possibility of malignant transformation in eruptive melanocytic nevi (EMN), the patient was scheduled for regular dermatologic follow‑ups, including dermoscopic evaluations every 3 months.
The sudden onset of numerous melanocytic nevi is a recognized but uncommon dermatologic side effect of BRAF inhibitors. This phenomenon is attributed to the paradoxical activation of the mitogen‑activated protein kinase (MAPK) pathway (RAS‑RAF‑MEK‑ERK) in melanocytes without the BRAF mutation, leading to uncontrolled proliferation and pigmentation changes.1 While MAPK activation in wild‑type melanocytes is the principal driver, concurrent EGFR inhibition can alter keratinocyte–melanocyte crosstalk and may lead to increased expression of stem cell factor and endothelin‑1, which can enhance melanocyte migration and proliferation.2 Of note, there are currently no reports of eruptive nevi secondary to cetuximab monotherapy. Lesions can vary in presentation, from new nevi formation to enlargement and darkening of pre‑existing nevi. Although these lesions are typically benign, the unusual nature of EMN and the potential for underlying genetic mutations, regular annual screening for dysplastic nevi and melanoma are recommended, despite a lack of concrete evidence of EMN directly transforming into melanoma.1 Given the increasing use of BRAF‑targeted therapies, clinicians should be aware of these dermatologic effects and implement routine skin surveillance to identify and manage potentially atypical lesions.
A brief summary of previously reported cases of EMN following BRAF‑inhibitor therapy is presented in Supplementary material, Table S1 for reference.3-6 These cases further emphasize the importance of dermatologic monitoring in patients undergoing targeted oncologic therapy.
- Perry BM, Nguyen A, Desmond BL, et al. Eruptive nevi associated with medications (ENAMs). J Am Acad Dermatol. 2016; 75: 1045‑1052. | Crossref
- Xu P, Yang L, Lai S, et al. Effects of EGFR‑TKI on epidermal melanin unit integrity: therapeutic implications for hypopigmented skin disorders. Pigment Cell Melanoma Res. 2024; 37: 514‑529. | Crossref
- Lam K, Gates GA, Bach DQ, Cheng K. Eruptive melanocytic nevi in the setting of encorafenib, cetuximab, and binimetinib combination therapy: a case report. Case Rep Dermatol. 2024; 16: 133‑139. | Crossref
- Meneguzzo A, Lazzarotto A, Alaibac M. Eruptive melanocytic nevi secondary to encorafenib for BRAF mutant metastatic colorectal cancer. In Vivo. 2020; 34: 441‑445. | Crossref
- Mikami H, Akasaka E, Nakano H, Sawamura D. Eruptive melanocytic nevi associated with encorafenib and cetuximab combination therapy. J Dermatol. 2023; 50: e173‑e174. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION