Comprehensive coagulation factor profiling in acute-on-chronic liver failure: a stepwise progression of hemostatic imbalance

 CC BY 4.0
CC BY 4.0
Comprehensive coagulation factor profiling in acute-on-chronic liver failure: a stepwise progression of hemostatic imbalance
Introduction
Acute‑on‑chronic liver failure (ACLF) is a complex and life‑threatening syndrome that occurs in patients with chronic liver disease. It is characterized by acute decompensation, multiorgan failure, and a high short‑term mortality rate.1 The pathophysiology of ACLF is closely linked to systemic inflammation, endothelial dysfunction, and profound alterations in coagulation.2 Traditionally, patients with advanced liver disease have been considered to be at an increased risk of bleeding due to thrombocytopenia and reduced levels of coagulation factors. However, emerging evidence suggests that ACLF is characterized by a rebalanced hemostasis, where both hypo- and hypercoagulable features coexist, leading to an increased risk of both bleeding and thrombotic complications.3,4
Standard coagulation tests, such as prothrombin time (PT), activated partial thromboplastin time (APTT), and international normalized ratio (INR), are frequently used in clinical practice to assess coagulation abnormalities in liver disease. However, these tests primarily reflect the procoagulant factor deficit and fail to provide a comprehensive evaluation of hemostasis, as they do not assess the contributions of anticoagulant proteins, platelets, fibrinolysis, or endothelial function.5,6 Recent studies using global hemostatic assays, such as viscoelastic tests (thromboelastometry, thromboelastography), have demonstrated that despite prolonged PT and APTT, thrombin generation remains preserved in ACLF, suggesting that these patients are not inherently at a high risk of spontaneous bleeding.7,8
One of the key drivers of coagulation abnormalities in ACLF is endothelial dysfunction, which manifests as elevated von Willebrand factor (vWF) levels and reduced disintegrin‑like metalloproteinase with thrombospondin type 1 motif, member 13 (ADAMTS13) activity, contributing to a prothrombotic state.9 vWF is a marker of endothelial activation, and has been increasingly recognized as a prognostic biomarker in ACLF, correlating with disease severity, organ failure, and mortality.10,11 Previous studies suggested that the vWF‑to‑ADAMTS13 ratio may serve as an important predictor of adverse outcomes in patients with ACLF.12
Despite these advancements in understanding the hemostatic derangement in ACLF, prior studies have mostly focused on isolated markers of coagulation dysfunction, while detailed coagulation factor profiling in a well‑characterized ACLF cohort remains limited. Moreover, few studies have examined how these abnormalities evolve across different ACLF severity grades (ACLF 1, 2, and 3). Given the increasing recognition that ACLF patients are at a risk of both bleeding and thrombosis, a more comprehensive evaluation of coagulation factor levels is warranted.
In this study, we aimed to provide a detailed characterization of coagulation factor deficiencies and global hemostatic alterations in a large cohort of ACLF patients, with particular emphasis on stratification by ACLF severity (grades 1, 2, and 3). We hypothesized that ACLF worsening would be associated with progressive coagulation factor depletion, increased vWF levels, and a greater imbalance between pro- and anticoagulant factors. By systematically evaluating coagulation factor levels, global hemostatic markers, and endothelial dysfunction parameters, this study provides a novel and comprehensive perspective on the coagulation alterations in ACLF, with potential implications for risk stratification, prognosis, and targeted therapeutic interventions.
Patients and methods
Patient selection and study design
This prospective observational study included 50 consecutive patients diagnosed with ACLF, who were either treated at or referred from other centers to a tertiary liver transplant (LT) referral center for evaluation for LT. The diagnosis of ACLF was established based on the European Association for the Study of the Liver – Chronic Liver Failure Consortium (CLIF‑C) criteria.1 ACLF was defined as acute decompensation of chronic liver disease associated with organ failure, characterized according to the CLIF‑C ACLF classification, which stratifies patients based on the presence and severity of organ dysfunctions using the CLIF‑C ACLF score. Patients were categorized into ACLF grades 1, 2, and 3, based on the number and type of organ failures.
Blood sample collection and laboratory analysis
Venous blood samples were collected from all patients at the time of ACLF diagnosis or upon admission to the tertiary center. The samples were immediately transported to the laboratory under standardized conditions to ensure their integrity. Coagulation factor levels and global coagulation parameters were analyzed using a 1‑stage clotting assay on the ACL TOP 550 analyzer (Werfen, Barcelona, Spain) with commercially available reagents. The following coagulation parameters were assessed: PT, INR, APTT, fibrinogen concentration (Clauss method), thrombin time, and antithrombin activity. The activity levels of coagulation factors II, V, VII, VIII, IX, X, XI, and XII were determined using specific 1‑stage clotting assays. The vWF antigen was measured using an immunoturbidimetric assay with monoclonal antibodies, while vWF activity was assessed immunologically using the ristocetin cofactor method. All analyses were performed according to the manufacturer’s instructions, and internal quality controls were applied to ensure reproducibility and accuracy of results.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics package, version 29.0 (IBM Corp., Armonk, New York, United States). Continuous variables were tested for normality of distribution using the Shapiro–Wilk test. Data were presented as median and interquartile range (IQR) for non‑normally distributed variables, while categorical variables were expressed as absolute numbers and percentages. Comparisons between groups were performed using the Mann–Whitney test for 2‑group comparisons and the Kruskal–Wallis test for multiple‑group comparisons. In the case of statistical significance in the Kruskal–Wallis test, post hoc comparisons were performed using the Dunn test with the Bonferroni correction. The χ2 test or Fisher exact test was used to compare categorical variables, as appropriate. In Figures, 95% CIs are presented for median values. The CIs were calculated using bootstrap resampling. A P value below 0.05 was considered significant.
Ethics
This study was conducted in accordance with the principles of the Declaration of Helsinki. As all procedures were part of standard clinical care and data were analyzed retrospectively in a fully anonymized manner, approval by the local bioethics committee was not required.
Results
Characteristics of the study group
The study included 50 consecutive patients diagnosed with ACLF on admission or the time of transfer from another center. The median (IQR) age of the patients was 49 (38.75–57) years, with a male predominance (72%). The most frequent underlying liver condition was alcohol‑associated liver disease (64%), followed by cryptogenic cirrhosis (8%) and other etiologies, such as autoimmune hepatitis, hepatitis B, hepatitis C, primary sclerosing cholangitis, Wilson disease, and metabolic dysfunction–associated steatotic liver disease. Regarding organ failure severity, 48% of the patients were classified as ACLF grade 1, while 32% and 20% were in ACLF grades 2 and 3, respectively. The median (IQR) Model for End‑Stage Liver Disease score was 31.19 (27.25–38.3), and the median (IQR) CLIF‑C ACLF score was 49.74 (43.39–56.7). LT was performed in 36% of the patients. Among the transplanted individuals, the 1‑year post‑transplant mortality rate was 33.3%, and the median (IQR) post‑transplant survival was 912.5 (111.75–1501) days. The mortality rate at 30 and 90 days in the entire cohort was 52% and 56%, respectively. Group characteristics are presented in Supplementary material, Table S1.
Coagulation profile in the whole acute‑on‑chronic liver failure group
The global hemostatic parameter analysis showed significant abnormalities consistent with liver failure. The median (IQR) INR was 2.2 (1.99–2.66); PT, 26.85 (24–32.03) s; APTT, 41.85 (37.35–54.4) s, and APTT ratio, 1.4 (1.25–1.82). The median (IQR) fibrinogen concentration was 158 (86.5–217) mg/dl, with a marked reduction in antithrombin levels (median [IQR], 20% [13%–30%]). The median (IQR) D‑dimer level was 2797 (1556.5–5481.5) ng/ml (Supplementary material, Table S2). Regarding coagulation factor activity, factors II, V, VII, IX, X, and XI were profoundly decreased. The median (IQR) activity was as follows: factor II, 28.4% (23%–39.3%); factor V, 32% (24.3%–44%); factor VII, 12.5% (8%–18.3%); factor IX, 50% (36.25%–68.25%); factor X, 44% (32%–61.25%); and factor XI, 41% (22%–55%). Factor VIII activity was significantly elevated (median [IQR], 247.3% [151.7%–378.2%]). The median (IQR) vWF antigen level was markedly increased at 250% (250%–877.2%), and the median (IQR) vWF activity was 390% (390%–590.7%; Supplementary material, Figure S1). Reference ranges for all laboratory parameters are listed in Supplementary material, Table S2.
Comparison of coagulation parameters in acute‑on‑chronic liver failure grade 1 vs grades 2+3
When stratified by ACLF severity, the patients with ACLF grade 1 had lower INR values (median [IQR], 2.06 [1.69–2.19]) than those with ACLF grades 2+3 (median [IQR], 2.54 [2.2–2.93]; P <0.001). Similar differences were observed with respect to PT (24.95 vs 30.2 s; P <0.001), APTT (39.15 vs 45.5 s; P = 0.004), and antithrombin levels (15.5% vs 23%; P = 0.02). Among the coagulation factors, factor VII levels were significantly lower (median [IQR], 9% [6.75%–14%] vs 16% [12%–21.5%]; P = 0.002), whereas factor VIII levels were higher (median [IQR], 340% [214.65%–521%] vs 167% [120.1%–299.6%]; P = 0.01) in the patients with ACLF grades 2+3 than in those with ACLF grade 1. vWF antigen levels were significantly increased in the ACLF grade 2+3 subgroup, as compared with the ACLF grade 1 subgroup (median [IQR], 443.8% [250%–1121.4%] vs 250% [250%–590.13%]; P = 0.04), similarly to vWF activity (median [IQR], 431.5% [390%–892%] vs 390% [388.95%–503.08%], respectively; P = 0.02; Supplementary material, Table S3).
Comparison of coagulation parameters in acute‑on‑chronic liver failure grade 1 vs grade 2 vs grade 3
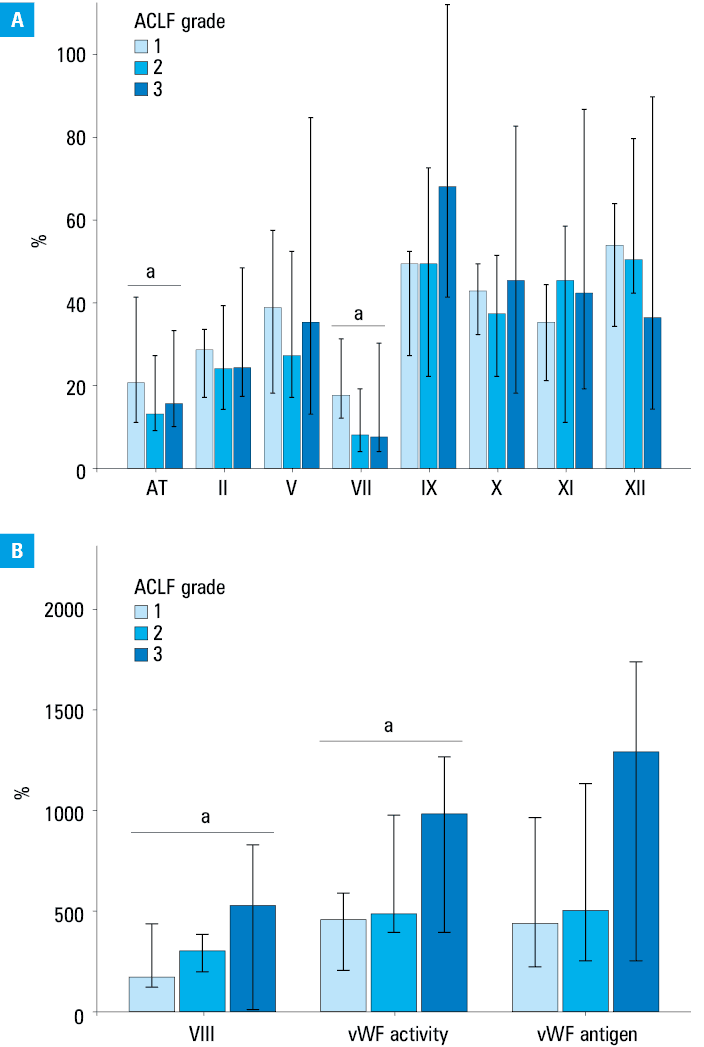
A stepwise worsening of coagulation abnormalities was observed across all ACLF grades (Figure 1). INR increased progressively from 2.06 in ACLF grade 1 to 2.44 in ACLF grade 2 and 2.75 in ACLF grade 3 (P <0.001). Similar trends were noted for PT (24.95 s vs 29.35 s vs 32.35 s, respectively; P = 0.002), APTT (39.15 s vs 46.65 s vs 45.25 s, respectively; P = 0.02) and antithrombin levels (23% vs 14% vs 16%, respectively; P = 0.04). Regarding coagulation factors, factor VII levels were the lowest in ACLF grade 3 (8.5%), as compared with ACLF grade 1 (16%) and grade 2 (11%; P = 0.005). Factor VIII levels increased with ACLF severity, reaching 412% in ACLF grade 3, as compared with 167% in ACLF grade 1 (P = 0.04). Similarly, vWF antigen levels were the highest in ACLF grade 3 (median, 731%), as compared with ACLF grade 1 (250%) and grade 2 (320%; P = 0.08). Significant differences between vWF activity levels were observed among the 3 subgroups, with the highest levels in the ACLF grade 3 patients (572.1% vs 390% in both grades 1 and 2; P = 0.03; Supplementary material, Table S4).
Discussion
Our study provides the so far most comprehensive analysis of coagulation factor activity levels in a large cohort of ACLF patients, stratified into ACLF grade 1, 2, and 3 subgroups. While previous studies have evaluated individual coagulation markers or global hemostatic parameters, this is the first work to systematically measure a broad spectrum of coagulation factors in a well‑characterized ACLF population. The observed differences in coagulation parameters across severity grades highlight the extent of hemostatic imbalance in advanced ACLF. These findings indicate that ACLF is not a uniformly hypocoagulable state but rather a dynamic and complex imbalance, where both pro- and anticoagulant components coexist. Prior studies using thromboelastometry and thrombin generation assays have demonstrated that ACLF patients maintain the thrombin generation capacity despite low coagulation factor levels, further supporting this concept.3,4,7
The results of our study demonstrated a significant reduction in coagulation factor activity (factors II, V, VII, IX, X, and XI) in ACLF, with marked differences observed between clinical severity groups. Although we did not perform a formal analysis of trend, the distribution of results across ACLF grades suggested that more severe forms of ACLF were associated with more profound coagulation disturbances. These findings align with prior research showing that conventional coagulation tests (INR, PT, APTT) do not accurately reflect the bleeding risk in ACLF. Instead, global hemostatic assays, such as viscoelastic tests, have been shown to be superior tools for assessing coagulopathy in ACLF, as they consider both pro- and anticoagulant pathways.6-8,13 Of particular interest, factor VIII levels were markedly elevated, especially in ACLF grades 2 and 3, which is consistent with the well‑documented endothelial activation and systemic inflammation observed in ACLF. Elevated factor VIII levels, in conjunction with low protein C and antithrombin levels, suggest a shift toward a prothrombotic state that may contribute to microvascular thrombosis and disease progression.12,14 Previous studies demonstrated that the factor VIII‑to‑protein C ratio was an independent predictor of liver‑related events in ACLF, supporting the growing recognition that thrombotic complications may play a critical role in disease progression.14
A particularly striking finding of our study is the significant elevation of the vWF antigen level and vWF activity, both of which correlated with ACLF severity. This adds to the accumulating evidence that vWF is a key marker of endothelial dysfunction and a strong predictor of mortality in ACLF.9-12 Prior research demonstrated that vWF levels correlated with systemic inflammation, organ failure, and short‑term mortality in ACLF patients, reinforcing its prognostic relevance.10,11 The imbalance between vWF and ADAMTS13 activity, which has been proposed as an emerging prognostic biomarker, reflects microvascular thrombosis and endothelial injury, further highlighting the role of endothelial dysfunction in ACLF pathogenesis.9
While several prior studies have evaluated coagulation abnormalities in ACLF, this study stands out as the most comprehensive evaluation of coagulation factor levels in a large ACLF cohort with detailed subgroup analysis. It is the first to assess the activity of a wide range of coagulation factors across different grades of ACLF, confirming the marked worsening of coagulation parameters in advanced disease. These findings complement prior research on global hemostatic dysfunction in ACLF.5,8 Moreover, the strong association between vWF levels and ACLF severity underscores its potential as a prognostic biomarker in ACLF.9-12 Our study also offers new insights into the interplay between factor VIII elevation and endothelial dysfunction, supporting recent evidence that ACLF is characterized by both hypo- and hypercoagulable mechanisms.14
In contrast to the traditional notion that ACLF is purely a bleeding disorder, our findings align with the modern paradigm that ACLF patients are at a risk of both bleeding and thrombosis, depending on the dynamic hemostatic balance.3,4,7 This is supported by recent studies utilizing thromboelastometry, which demonstrate that patients with ACLF exhibit preserved thrombin generation despite abnormal INR and APTT values.7 The limitations of conventional coagulation tests in ACLF are increasingly recognized, and our study reinforces the necessity of using global coagulation assays (thromboelastography, rotational thromboelastometry) for more accurate risk assessment.6,8
The strong association between vWF level and activity elevation and ACLF severity suggests potential therapeutic implications, as interventions targeting endothelial dysfunction and microvascular thrombosis could improve outcomes in ACLF.5,9 Future research should integrate vWF and the factor VIII‑to‑protein C ratio into ACLF prognostic models to improve mortality prediction. Investigating endothelium‑targeted therapies, such as ADAMTS13 supplementation or plasma exchange, is also crucial. Additionally, studies should assess dynamic coagulation changes to clarify the shifting hypo- and hypercoagulability balance in ACLF.
Despite the strengths of our study, including its large cohort and comprehensive coagulation profiling, some limitations must be acknowledged. As it was a single‑center study, the findings may not be fully generalizable to all ACLF populations. Furthermore, while we measured detailed coagulation factor levels, we did not incorporate thromboelastometry data, which could provide additional insights into the functional aspects of coagulation. Additionally, our study primarily assessed coagulation parameters at the time of ACLF diagnosis; future research should evaluate longitudinal changes in coagulation factor activity and vWF levels to explore their evolving role in ACLF prognosis.
Conclusions
This study provides a comprehensive and novel evaluation of coagulation factor alterations in ACLF, demonstrating significant differences in coagulation factor activity and vWF levels between clinical severity subgroups. Although no formal trend analysis was performed, the results indicate that more severe forms of ACLF are associated with greater hemostatic imbalance. These findings confirm that ACLF represents a dynamic state of hemostatic imbalance, where both bleeding and thrombosis risks coexist. The strong association of vWF level elevation with ACLF severity highlights its potential as a prognostic biomarker and therapeutic target. Future studies should explore vWF‑directed interventions and global hemostatic assays to optimize risk stratification and treatment strategies in ACLF.
- Moreau R, Jalan R, Gines P, et al. Acute‑on‑chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144: 1426‑1437. | Crossref
- Bernal W, Jalan R, Quaglia A, et al. Acute‑on‑chronic liver failure. Lancet. 2015; 386: 1576‑1587. | Crossref
- Lisman T, Porte RJ. Rebalanced hemostasis in patients with liver disease: evidence and clinical consequences. Blood. 2010; 116: 878‑885. | Crossref
- Tripodi A, Mannucci PM. The coagulopathy of chronic liver disease. N Engl J Med. 2011; 365: 147‑156. | Crossref
- Zanetto A, Campello E, Bulato C, et al. Global hemostatic profiling in patients with decompensated cirrhosis and bacterial infections. JHEP Rep. 2022; 4: 100493. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION