Cryptococcosis is recognized as one of the most common life‑threatening opportunistic fungal infections. It typically occurs through inhalation of fungal spores or, occasionally, through contact with bird droppings, such as those of pigeons, or with contaminated soil.1 We present a case of a 58‑year‑old man with a history of extrinsic allergic alveolitis (EAA), on long‑term immunosuppressive therapy (methylprednisolone 8 mg/day and azathioprine 100 mg/day) for the past 4 years, who developed disseminated cryptococcosis with primary cutaneous manifestations alongside EAA, necessitating prolonged immunosuppressive treatment. He presented to a dermatology department with persistent, widespread skin lesions. The lesions, present for approximately 1 year, consisted of numerous pink‑white and skin‑colored nodules, 2–5 mm in diameter, distributed across the cheeks, chin, nose, around the mouth, neck, upper chest, and upper limbs (Figure 1A). Due to his impaired lung function, he also required continuous oxygen therapy and was being prepared for lung transplant.
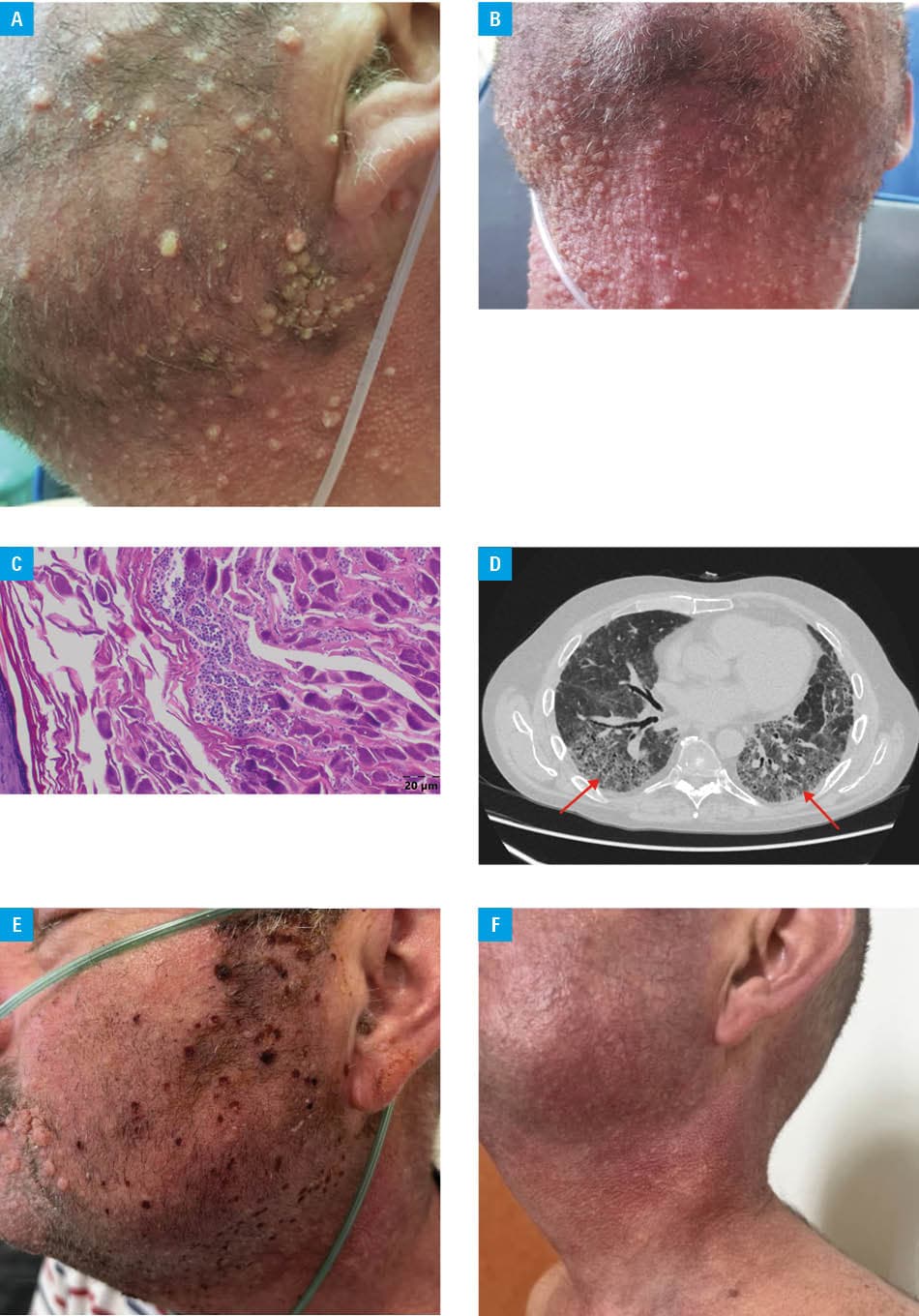
Given the patient’s immunosuppression and disseminated cutaneous involvement, the differential diagnosis included infectious, neoplastic, and granulomatous diseases. Histopathologic examination of the skin biopsy showed spherical fungal cells, likely of the Cryptococcus species, within granulomatous tissue (Figure 1B). A positive Cryptococcus neoformans antigen blood test confirmed the presence of fungus, supporting the diagnosis of cutaneous cryptococcosis.
A pulmonology consultation and high‑resolution computed tomography of the chest (Figure 1C) did not exclude pulmonary cryptococcosis. However, bronchoscopy was not recommended. Additional laboratory tests identified mild megaloblastic anemia, while other parameters, including QuantiFERON‑TB Gold Plus test (QIAGEN, Venlo, Netherlands), HIV in vitro chemiluminescent immunoassay (LIAISON XL MUREX HIV Ab/Ag HT; DiaSorin, Saluggia, Italy), and blood cultures, were negative. Sputum culture yielded predominantly saprophytic flora.
Lumbar puncture was performed due to muscle weakness in the thighs to exclude cryptococcal dissemination to the central nervous system. Cerebrospinal fluid analysis showed clear fluid with normal levels of protein (34 mg/dl; reference range [RR] <40 mg/dl), glucose (65 mg/dl; RR, 45–75 mg/dl), and chloride (125 mmol/l; RR, 112–130 mmol/l), mild pleocytosis (4 cells/µl; RR, 0–5 cells/µl), and negative fungal cultures. Polymerase chain reaction test for C. neoformans DNA was not performed.
The patient was treated with liposomal amphotericin B (100 mg/day intravenously) for 21 days, followed by oral fluconazole (400 mg/day) for 6 months. Additional therapy included sulfamethoxazole‑trimethoprim (480 mg/day) and acitretin (25 mg/day), along with intensive local skin treatment including curettage, electrotherapy, and fractional carbon dioxide laser therapy (Figure 1D). All medications were administered concurrently with ongoing immunosuppressive and oxygen therapy. Complete remission was achieved and has persisted for 14 months (Figure 1E and 1F), with no significant adverse effects reported.
Cryptococcal infections, especially in immunocompromised patients, are often linked to prolonged corticosteroid use, which impairs the phagocytic function of alveolar macrophages, facilitating fungal spread beyond the lungs.2-4 In this case, the patient’s long‑term immunosuppressive therapy for EAA and close proximity to pigeon breeders likely increased his infection risk.5 This case highlights the importance of including cryptococcosis in the differential diagnosis of persistent skin lesions in immunocompromised individuals.
- Noguchi H, Matsumoto T, Kimura U, et al. Cutaneous cryptococcosis. Med Mycol J. 2019; 60: 101‑107. | Crossref
- Mada PK, Jamil RT, Alam MU. Cryptococcus. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan. https://www.ncbi.nlm.nih.gov/books/NBK431060/. Accessed March 20, 2025.
- Dahshan D, Dessie SA, Cuda J, Khalil E. Primary cutaneous cryptococcosis in a patient on fingolimod: a case report. Cureus. 2021; 13: e16444. | Crossref
- Hosoda C, Ishiguro T, Uozumi R, et al. Characteristics of pulmonary cryptococcosis in patients with rheumatoid arthritis. BMJ Open Respir Res. 2021; 8: e000805. | Crossref
- Neuville S, Dromer F, Morin O, et al. Primary cutaneous cryptococcosis: a distinct clinical entity. Clin Infect Dis. 2003; 36: 337‑347. | Crossref
ARTICLE INFORMATION