Coronary revascularization in patients with ST-segment elevation myocardial infarction and multivessel disease: 2-year follow-up from a large multicenter registry
Key words: complete revascularization, multivessel coronary artery disease, rehospitalization, ST-segment elevation myocardial infarction

 CC BY 4.0
CC BY 4.0
Coronary revascularization in patients with ST-segment elevation myocardial infarction and multivessel disease: 2-year follow-up from a large multicenter registry
Introduction: Multivessel coronary artery disease (MVD) occurs in one‑third of patients with ST‑segment elevation myocardial infarction (STEMI) who undergo primary percutaneous coronary intervention (pPCI). However, long‑term prognosis and readmission rates in this high‑risk group remain unclear.
Objectives: We aimed to evaluate the long‑term risk of cardiovascular events and readmissions in STEMI patients with MVD.
Patients and methods: This prospective observational study included 1513 patients enrolled in the Silesian Cardiovascular Database between 2017 and 2020. We analyzed demographic, clinical, and angiographic characteristics along with prognosis during 2‑year follow‑up.
Results: A total of 439 patients with MVD were identified in the registry. Among them, 2‑vessel disease (2‑VD) was detected in 329 patients (74.9%) and 3‑vessel disease (3‑VD) in 110 (25.1%). During 2‑year follow‑up, overall survival and the incidence of major adverse cardiovascular events (death, MI, stroke) were similar in both groups. In multivariable analyses, previous MI (hazard ratio [HR], 1.63; 95% CI, 1.01–2.63; P = 0.04) and the left main coronary artery as the infarct‑related artery (IRA; HR, 3.22; 95% CI, 1–10.38; P = 0.049) increased the risk of unplanned cardiac readmissions, whereas clopidogrel use (HR, 1.45; 95% CI, 1.07–1.95; P = 0.01) increased the risk of all‑cause readmissions. PCI of a non‑IRA during the index hospitalization was associated with a lower risk of both unplanned cardiac (HR, 0.61; 95% CI, 0.42–0.9; P = 0.01) and all‑cause (HR, 0.61; 95% CI, 0.46–0.82; P = 0.001) readmissions.
Conclusions: Two‑year overall survival and event‑free survival were similar in STEMI patients with 2‑VD and 3‑VD. The use of more potent antiplatelets instead of clopidogrel as well as non‑IRA revascularization during the index hospitalization appear to be important for minimizing readmission rates.
What's new?
This study provides new insights into the prognosis of patients with ST‑segment elevation myocardial infarction and multivessel coronary artery disease. We found that the extent of atherosclerosis, defined as the number of coronary arteries with significant lesions, did not seem to affect overall survival, the incidence of major adverse cardiovascular events, or unplanned cardiac and all‑cause readmissions during 2‑year follow‑up. We also identified the use of more potent antiplatelets instead of clopidogrel along with revascularization of noninfarct‑related arteries during initial hospitalization as important targets that could help minimize readmission rates in this group of patients.

Introduction
Contemporary management in the acute phase of ST‑segment elevation myocardial infarction (STEMI) is based on early primary percutaneous coronary intervention (pPCI) in the infarct‑related artery (IRA) combined with dual antiplatelet therapy (DAPT).1 Park et al2 demonstrated that approximately 30% to 50% of patients enrolled in the Korea Acute Myocardial Infarction Registry had significant atherosclerotic lesions in more than 1 coronary artery. In our recent report, multivessel coronary artery disease (MVD) was present in 32.9% of STEMI patients.3 These individuals have an adverse prognosis, as compared with those with single‑vessel disease (SVD).4 According to previous studies, complete revascularization (CR) reduces the risk of major adverse cardiac events (MACEs), such as cardiovascular mortality, new MI, and ischemia‑driven revascularization.5,6 Therefore, the latest guidelines of the European Society of Cardiology1 upgraded the recommendation for non‑IRA revascularization during the index procedure or within 45 days after discharge in hemodynamically stable patients. Following our preliminary report,3 our objective was to evaluate the long‑term prognosis after pPCI in STEMI patients with MVD included in the Polish Registry of Acute Coronary Syndromes (PL‑ACS).
Patients and methods
The principles of the PL‑ACS have been presented elsewhere.3,7 Briefly, this is a national, multicenter, prospective observational registry that includes data on patients with ACS. By the end of 2022, we were able to collect data on 674 461 patients. Follow‑up data were extracted from the Silesian Cardiovascular Database—a digital tool designed to report data on ACS to the National Health Fund. Data on STEMI patients treated with pPCI in 18 centers between 2017 and 2020 were analyzed. During that period, information regarding lesion significance was available for 1513 individuals. After excluding 68 patients (4.5%) who died during hospitalization and 1006 individuals (69.6%) with MI and SVD, the final study group comprised 439 patients (30.4%) with MVD. MVD was defined as a presence of at least 2 significantly stenosed coronary arteries (≥50% diameter stenosis on visual angiographic assessment), including the culprit lesion and at least 1 significant lesion in a non‑IRA territory. The patients were classified into the 2‑vessel disease (2‑VD) and 3‑vessel disease (3‑VD) groups according to the number of coronary arteries with atherosclerotic plaques (Figure 1). Four revascularization strategies were considered: culprit vessel only during the index pPCI, immediate or staged CR during the index hospitalization, and elective CR after discharge following the index hospitalization. All patients provided written informed consent to participate in the study. All procedures were performed according to the current guidelines.8,9 The study was approved by the Ethics Committee at the Jan Kochanowski University in Kielce (6/2017).
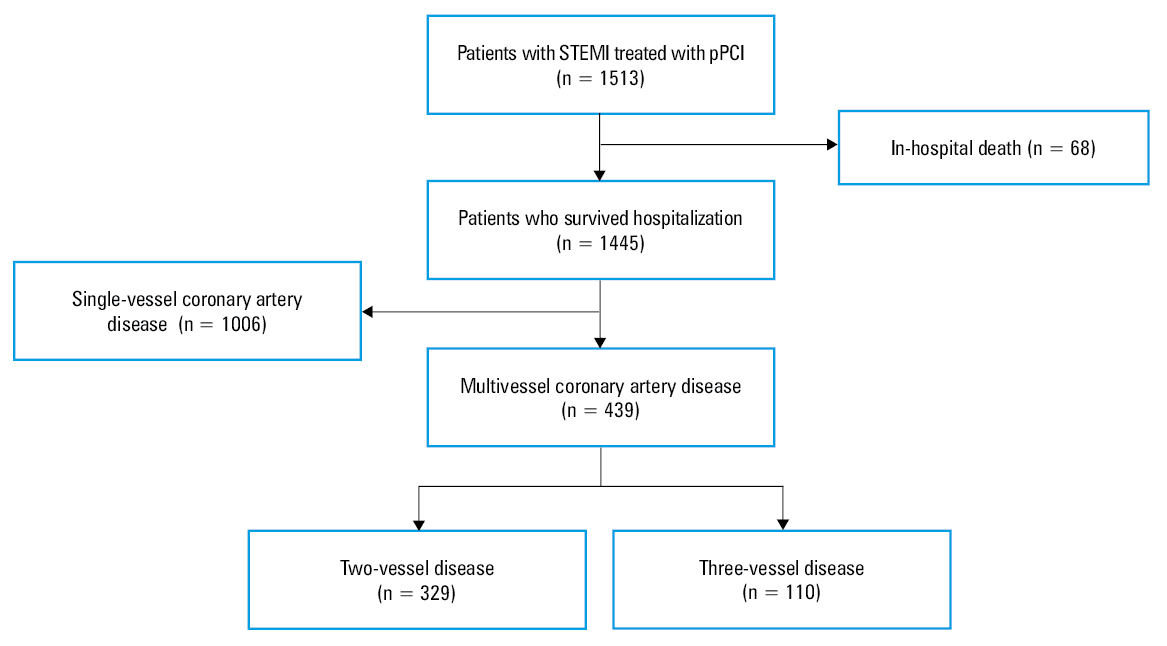
Abbreviations: pPCI, primary percutaneous coronary intervention; STEMI, ST‑segment elevation myocardial infarction
Demographic, clinical, and angiographic characteristics of the patients, together with data on pharmacotherapy and vascular access site were collected. Coronary anatomy was identified as previously described.3 The patients were followed for up to 24 months to assess the risk of MACEs, defined as all‑cause mortality, MI, stroke, coronary revascularization, as well as unplanned cardiac or all‑cause rehospitalization. Bleeding during follow‑up was defined as gastrointestinal bleeding or hemorrhagic stroke requiring hospitalization.
Statistical analysis
Categorical variables are presented as numbers and percentages and were compared using the Pearson χ2 test or Fisher test. Continuous variables are expressed as means and SD or medians with interquartile ranges, as appropriate. The normality assumption was verified with the Shapiro–Wilk test. Intergroup differences for the normally distributed variables were assessed using the t test, while the Mann–Whitney test was applied to compare the non‑normally distributed continuous variables. All survival analyses were conducted using the Kaplan–Meier estimator, and differences between subgroups were assessed using the log‑rank test. Univariable and multivariable Cox regression analyses were performed to identify potential independent predictors of all‑cause and cardiac readmissions. All variables were included in univariable regression analyses, and those with P values below 0.3 in the univariable analyses were considered for inclusion in the multivariable Cox regression models. The final multiple model was constructed using the backward stepwise regression method. The results are presented as hazard ratios (HRs) with 95% CIs; the proportional hazards assumption was checked using the Schoenfeld residuals. Two‑sided P values below 0.05 were considered significant. All analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, North Carolina, United States).
Results
Baseline clinical characteristics
The study population comprised 439 patients, 302 men (68.8%) and 137 women (31.2%), at a mean (SD) age of 65.2 (10.4) years. Of these, 329 (74.9%) had 2‑VD and 110 (25.1%) had 3‑VD. The baseline characteristics were similar, except for a higher prevalence of previous MI in the 2‑VD group. On admission, the rates of cardiac arrest and Killip class III or IV were low. DAPT was administered in a vast majority of patients, with a predominance of clopidogrel and ticagrelor. Unfractionated heparin was chosen most frequently in both groups; however, low‑molecular‑weight heparin was used significantly less frequently in the patients with 2‑VD. The rate of glycoprotein IIb/IIIa inhibitor administration was similar in both groups (Table 1).
Variable | 3‑VD group (n = 110) | 2‑VD group (n = 329) | P value | |
Data are presented as number (percentage) of patients unless indicated otherwise.
Abbreviations: 2‑VD, 2‑vessel disease; 3‑VD, 3‑vessel disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DAPT, dual antiplatelet therapy; GP, glycoprotein; IQR, interquartile range; LMWH, low‑molecular‑weight heparin; LVEF, left ventricular ejection fraction; MI, myocardial infarction; NOAC, non–vitamin K antagonist oral anticoagulant; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; UFH, unfractionated heparin; VKA, vitamin K antagonist | ||||
Age, y, mean (SD) | 66.7 (9.8) | 64.7 (10.5) | 0.08 | |
Women | 37 (33.6) | 100 (30.4) | 0.53 | |
Medical history | ||||
Smoking | 42 (41.2) | 146 (50.7) | 0.21 | |
Obesity | 12 (11.9) | 59 (19.7) | 0.07 | |
Previous MI | 8 (7.3) | 52 (15.9) | 0.02 | |
Previous PCI | 11 (10) | 50 (15.2) | 0.17 | |
Previous stroke | 4 (3.6) | 9 (2.8) | 0.64 | |
Dyslipidemia | 58 (58) | 162 (55.7) | 0.69 | |
Diabetes | 28 (26.9) | 94 (29.8) | 0.57 | |
Arterial hypertension | 60 (58.3) | 208 (66.5) | 0.13 | |
Heart failure | 3 (2.7) | 14 (4.3) | 0.46 | |
Atrial fibrillation | 5 (4.5) | 11 (3.4) | 0.57 | |
PAD | 3 (2.8) | 13 (4) | 0.55 | |
CKD | 6 (5.5) | 16 (4.9) | 0.82 | |
COPD | 6 (5.5) | 10 (3.1) | 0.26 | |
Clinical presentation on admission | ||||
Cardiac arrest | 2 (1.8) | 8 (2.4) | 0.71 | |
Killip class | I | 80 (72.7) | 252 (76.6) | 0.4 |
II | 21 (19.1) | 57 (17.3) | ||
III | 4 (3.6) | 4 (1.2) | ||
IV | 5 (4.5) | 16 (4.9) | ||
LVEF, %, median (IQR) | 45 (35–50) | 45 (40–50) | 0.1 | |
In‑hospital treatment | ||||
Acetylsalicylic acid | 106 (96.4) | 315 (95.7) | 0.78 | |
Ticagrelor | 49 (44.5) | 130 (39.5) | 0.35 | |
Prasugrel | 0 | 3 (0.9) | 0.32 | |
Clopidogrel | 54 (49.1) | 172 (52.3) | 0.56 | |
UFH | 109 (99.1) | 325 (98.8) | 0.79 | |
LMWH | 24 (21.8) | 44 (13.4) | 0.03 | |
GP IIb/IIIa inhibitor | 34 (30.9) | 111 (33.7) | 0.59 | |
DAPT and anticoagulants at discharge | ||||
DAPT | 105 (95.5) | 309 (93.9) | 0.55 | |
NOAC | 6 (5.5) | 11 (3.3) | 0.32 | |
VKA | 0 | 3 (0.9) | 0.32 | |
Baseline angiographic and procedural characteristics
Transradial access was used in most patients. The rates of restenosis and in‑stent thrombosis in the 3‑VD and 2‑VD groups were low (0% vs 4.6%; P = 0.02 and 1.8% vs 1.8%; P >0.99, respectively). Chronic total occlusions (CTOs) were identified more frequently in the 3‑VD than the 2‑VD group (25.5% vs 10.6%; P <0.001). The right coronary artery (44.2%) and left anterior descending artery (37.8%) were most frequently identified as IRAs, while non‑IRA lesions were evenly distributed throughout the coronary tree. A higher prevalence of non‑IRA lesions in each coronary artery was found in the 3‑VD group. The patients with 3‑VD more often underwent PCI of the non‑IRA during the index procedure (Table 2). The most common method for detecting non‑IRA lesions was visual assessment. Fractional flow reserve (FFR) measurement and intravascular ultrasound were performed in 8 (1.8%) and 19 (4.3%) cases, respectively.
Variable | 3‑VD group (n = 110) | 2‑VD group (n = 329) | P value |
Data are presented as numbers (percentages).
Abbreviations: CTO, chronic total occlusion; Cx, circumflex branch; D, diagonal branch; IM, intermediate branch; IRA, infarct‑related artery; LAD, left anterior descending artery; LM, left main coronary artery; OM, obtuse marginal branch; RCA, right coronary artery; others, see Table 1 | |||
Vascular access site during the index procedure | |||
Femoral | 20 (18.2) | 95 (28.9) | 0.07 |
Radial | 90 (81.8) | 234 (71.1) | |
Lesion characteristics | |||
In‑stent restenosis | 0 | 15 (4.6) | 0.02 |
In‑stent thrombosis | 2 (1.8) | 6 (1.8) | >0.99 |
Bifurcation | 5 (4.5) | 9 (2.7) | 0.35 |
CTO | 28 (25.5) | 35 (10.6) | <0.001 |
Location of IRA | |||
LM | 4 (3.6) | 2 (0.6) | 0.02 |
LAD | 41 (37.3) | 152 (38) | 0.89 |
Cx | 8 (7.3) | 40 (12.2) | 0.16 |
RCA | 51 (46.4) | 143 (43.5) | 0.6 |
Other (OM, D, IM) | 7 (6.4) | 30 (9.1) | 0.37 |
Location of non‑IRA lesions | |||
LM | 11 (10) | 4 (1.2) | <0.001 |
LAD | 55 (50) | 109 (33.1) | 0.001 |
Cx | 65 (59.1) | 74 (22.5) | <0.001 |
RCA | 56 (50.9) | 96 (29.2) | <0.001 |
Other (OM, D, IM) | 53 (48.2) | 65 (19.8) | <0.001 |
Non‑IRA PCI strategy | |||
During the primary PCI | 28 (25.5) | 48 (14.6) | 0.009 |
During the index hospitalization | 72 (65.5) | 168 (51.1) | 0.009 |
Elective PCI | 37 (33.6) | 75 (22.8) | 0.02 |
Not planned | 20 (18.2) | 86 (26.1) | 0.09 |
Clinical outcomes
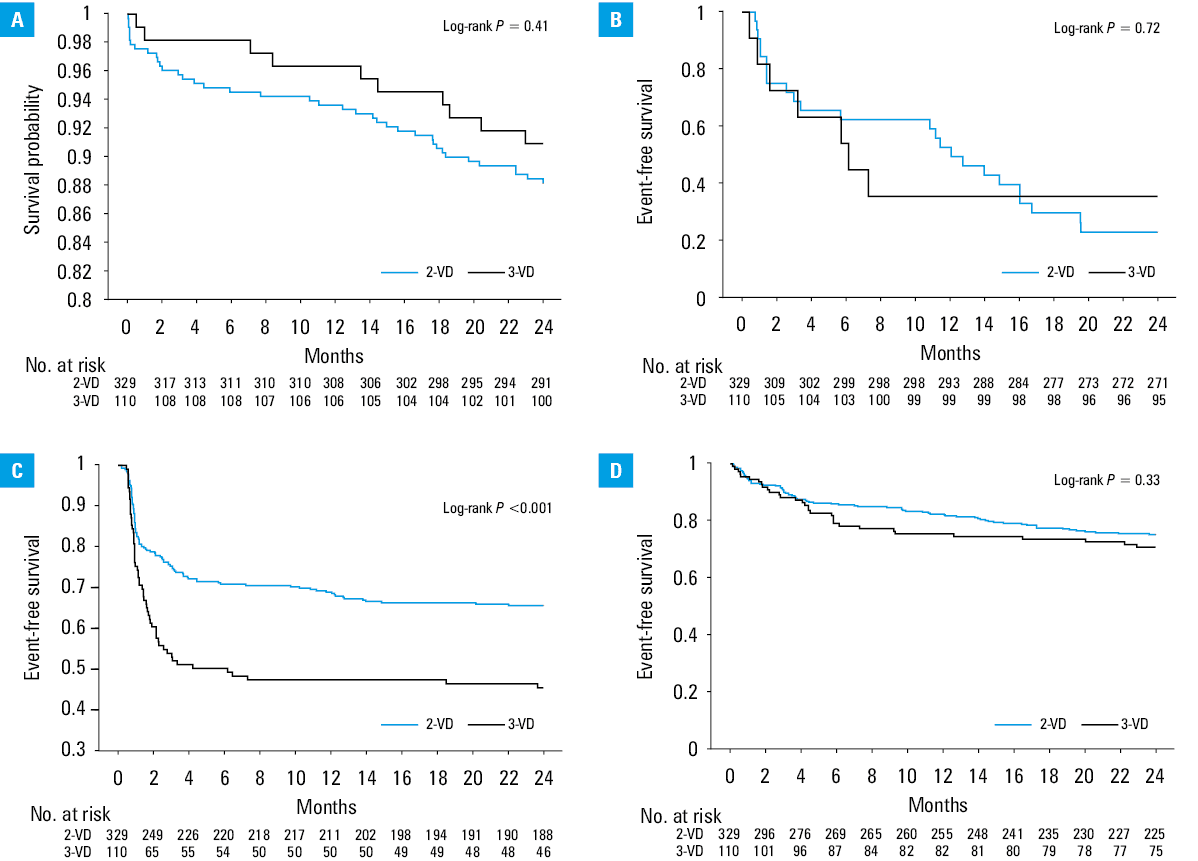
All participants completed the 2‑year follow‑up. In‑hospital complication rates were low and did not differ between the groups. The patients with 3‑VD had a markedly higher rate of repeat PCI than those with 2‑VD, but it included cases of scheduled non‑IRA PCI. Differences in all‑cause mortality, MI, stroke, bleeding, as well as unplanned cardiac and all‑cause readmission rates were insignificant (Table 3, Figure 2). With respect to readmissions, 62.5% of them were due to cardiac causes (STEMI [25.6%] and chronic coronary syndromes [24.5%] as the leading causes) in both groups (Table 3).
Outcome | In‑hospital | 2‑year follow‑up | ||||
3‑VD group (n = 110) | 2‑VD group (n = 329) | P value | 3‑VD group (n = 110) | 2‑VD group (n = 329) | P value | |
Data are presented as numbers (percentages).
Abbreviations: N/A, not applicable; TIA, transient ischemic attack; others, see Table 1 | ||||||
Death | N/A | N/A | N/A | 10 (9.1) | 39 (11.9) | 0.43 |
MI | N/A | N/A | N/A | 7 (6.4) | 24 (7.3) | 0.74 |
PCI | N/A | N/A | N/A | 59 (53.6) | 109 (33.1) | <0.001 |
Stroke/TIA | 1 (0.9) | 0 | 0.08 | 3 (2.7) | 6 (1.8) | 0.56 |
Bleeding | 2 (1.8) | 4 (1.2) | 0.64 | 4 (3.6) | 9 (2.7) | 0.63 |
All‑cause readmission | N/A | N/A | N/A | 42 (38.2) | 134 (40.7) | 0.64 |
Unplanned cardiac readmission | N/A | N/A | N/A | 32 (29.1) | 78 (23.7) | 0.26 |
Abbreviations: see Table 1
In the univariable Cox regression, the risk of all‑cause readmission was higher in the patients with obesity, heart failure (HF), chronic kidney disease (CKD), and those receiving clopidogrel, whereas unplanned cardiac readmissions were more likely in the patients with HF, CKD, and previous MI. Administration of ticagrelor and CR during the index hospitalization were associated with a lower risk of all‑cause readmission and unplanned cardiac rehospitalization. In the multivariable Cox regression, the strongest predictor of unplanned readmission was clopidogrel administration. Previous MI and the left main coronary artery as the IRA increased the risk of unplanned cardiac rehospitalization. The only multivariable predictor associated with a lower rehospitalization rate during 2‑year follow‑up was staged non‑IRA PCI during the index hospitalization (Table 4).
Variable | Univariable HR (95% CI) | P value | Multivariable HR (95% CI) | P value |
Predictors of all‑cause readmissions | ||||
Obesity | 1.54 (1.07–2.23) | 0.02 | – | – |
HF | 2.47 (1.37–4.45) | 0.002 | – | – |
CKD | 2.42 (1.42–4.11) | 0.001 | – | – |
Clopidogrel | 1.43 (1.06–1.93) | 0.02 | 1.45 (1.07–1.95) | 0.01 |
Ticagrelor | 0.61 (0.44–0.83) | 0.002 | – | – |
GP IIb/IIIa inhibitor | 0.69 (0.5–0.97) | 0.03 | – | – |
Non‑IRA in‑hospital staged PCI | 0.62 (0.46–0.83) | 0.002 | 0.61 (0.46–0.82) | 0.001 |
In‑hospital CR | 0.69 (0.51–0.94) | 0.02 | – | – |
Predictors of unplanned cardiac readmissions | ||||
HF | 4.21 (2.31–7.69) | <0.001 | – | – |
CKD | 2.67 (1.43–4.98) | 0.002 | – | – |
Previous MI | 1.59 (0.99–2.57) | 0.053 | 1.63 (1.01–2.63) | 0.04 |
Ticagrelor | 0.6 (0.4–0.9) | 0.01 | – | – |
GP IIb/IIIa inhibitor | 0.64 (0.42–0.99) | 0.04 | – | – |
IRA LM | 2.33 (0.74–7.35) | 0.15 | 3.22 (1–10.38) | 0.049 |
Non‑IRA in‑hospital staged PCI | 0.63 (0.43–0.92) | 0.02 | 0.61 (0.42–0.9) | 0.01 |
In‑hospital CR | 0.66 (0.44–0.97) | 0.04 | – | – |
Discussion
The main finding of our study is that STEMI patients with MVD benefited from non‑IRA PCI during the index hospitalization in terms of a lower rate of rehospitalization due to both cardiac and noncardiac causes.
Presence of a significant atherosclerotic lesion in the non‑IRA territory is associated with unfavorable long‑term and in‑hospital prognosis in MVD, as compared with SVD.4,10,11 Several studies on the impact of MVD on clinical outcomes in Polish patients with STEMI were published.12,13 Our analysis showed a lower incidence of MVD in STEMI patients than reported by Park et al2 and Toma et al.14 In the general population included in the PL‑ACS between 2017 and 2020, the prevalence of MVD (28.4%) and the mean age of the patients (65.2 years) were similar to those reported in our study15; however, we observed a higher proportion of women than other researchers.16,17 The most common IRAs were the right (44.2%) and left anterior descending arteries (37.8%), with a 10.9% contribution of the circumflex branch, which is less common than previously reported.5,6,17
The clinical profile of the patients with 2‑VD and 3‑VD was similar. We provide novel data on comorbidities (ie, obesity, HF, atrial fibrillation, and chronic obstructive pulmonary disease) that impact cardiovascular prognosis and were not previously reported. We identified 24.4% of patients with Killip class greater than I on admission, with no significant differences between the 2‑VD and 3‑VD groups; however, this proportion was greater than previously reported.5,6,17,18
Several studies provided clinical evidence for the superiority of CR over culprit‑only revascularization among STEMI patients with MVD.5,6,19,20 However, they used different methods to detect the significance of the non‑IRA lesion, that is, angiographic visual assessment5,20,21 or FFR evaluation.17,22 The optimal methods for detecting lesion significance in the non‑IRA territory and their impact on the long‑term prognosis remain unclear. Several reports demonstrated a significant benefit of an angiography‑guided approach over an FFR‑guided strategy,18,23 while Lee et al24 confirmed the superiority of functional lesion assessment prior to PCI. Furthermore, in the COMPLETE trial (Complete vs Culprit‑only Revascularization to Treat Multi‑vessel Disease After Early PCI for STEMI),6 FFR measurement was recommended for lesions with 50%–70% diameter stenosis, while stenosis greater than 70% did not require FFR assessment prior to revascularization. Due to the heterogeneity in the definition of lesion significance and the inclusion criteria across studies, extrapolation of the results remains challenging.
Angiographic characteristics of the lesions on diagnostic coronary angiography differed between the analyzed patients groups. In‑stent restenosis was more prevalent in the 2‑VD group, whereas CTO lesions were more frequently observed in the 3‑VD group. The CR rate was similar in both groups. Bangalore et al25 identified the number of diseased vessels and presence of CTO as the strongest predictors of incomplete revascularization (ICR) in patients with MVD.
ICR was associated with a significantly higher risk of MACEs, as compared with CR. However, univariable Cox regression showed that CTO lesions were not associated with an increased risk of readmissions during 2‑year follow‑up.
We observed lower DAPT rates, as compared with the available reports.5,6,17,21,22 In our study, clopidogrel was the most widely used platelet receptor P2Y12 inhibitor, but the rate of ticagrelor administration was also high. However, Polish patients received ticagrelor or prasugrel less frequently than individuals from other countries. The reason for this may be the lack of reimbursement for the guideline‑preferred platelet receptor P2Y12 inhibitors. Most of our data predate the publication of the ISAR‑REACT 5 (Prospective, Randomized Trial of Ticagrelor Versus Prasugrel in Patients With Acute Coronary Syndrome) results,26 which may explain the very low use of prasugrel. Our findings support the need for a broad implementation of novel antiplatelet agents, as clopidogrel remained a significant predictor of readmission in the multivariable analysis.
In‑hospital and long‑term outcomes
We found that multivessel PCI during the index hospitalization was safe and beneficial. Although the PCI rates were higher in the 3‑VD group, this seems to result from the greater number of arteries to treat. No differences in all‑cause mortality, MI, stroke, bleeding, and all‑cause or cardiac readmission rates suggest that non‑IRA PCI should not be postponed without a significant reason. Although the number of procedures per patient was higher in the 3‑VD group as compared with the 2‑VD group, bleeding rates were low and consistent with other reports.5,6,17 In previous reports, HF, MI, and arrhythmias together with old age, female sex, lower socioeconomic status, CKD, and anemia were the most frequently responsible for readmissions after pPCI.27,28 In the current study, age and sex were not associated with readmissions, but we confirmed HF, CKD, peripheral artery disease, and previous MI as significant predictors of all‑cause readmission, with only previous MI remaining a significant predictor in the multivariable analysis, together with non‑IRA PCI performed during the index admission.
Clopidogrel administration was the strongest predictor of all‑cause readmissions, but it did not increase the likelihood of unplanned cardiac readmissions in the follow‑up period. Therefore, DAPT with clopidogrel may serve as a marker of a higher‑risk population, including older patients and those with prior bleeding events, atrial fibrillation, or stroke history. In addition, more intensive antiplatelet therapy with ticagrelor reduced the risk of both all‑cause and cardiac rehospitalization. This confirms that newer potent P2Y12 inhibitors are more effective than clopidogrel in reducing subsequent cardiovascular events, and patients at a higher risk of recurrent ischemic events may benefit most from more intensive antiplatelet therapy.
Limitations
This study has several limitations. First, the sample size was relatively small, and 2‑year follow‑up may be too short to detect a significant number of MACEs. Second, laboratory test results and detailed echocardiographic findings (eg, biomarkers of inflammation or heart function) were not available in our registry. The absence of these data may limit the possibility to determine the underlying pathophysiology of long‑term outcomes in these patients. Third, defining significant stenosis based on a visual assessment of at least 50% diameter reduction is characterized by high sensitivity but low specificity. Angiographic visual assessment does not determine the functional significance of borderline coronary artery stenosis. Physiological assessment of such stenoses is currently the standard for determining revascularization eligibility. Fourth, the study used the International Classification of Diseases, Tenth Revision (ICD‑10) and ICD‑9 codes for diagnoses and procedures reported to the National Health Fund, instead of central adjudication for clinical outcomes. Coding errors cannot be entirely excluded, and incomplete or missing data may bias the conclusions. Fifth, the specific mechanisms behind improved long‑term outcomes in the patients undergoing non‑IRA revascularization were not fully explored (apart from hospital readmissions). Further research should focus on the long‑term benefits of different revascularization strategies, including their impact on hard clinical end points.
Conclusions
The prognosis of patients with STEMI and MVD was similar, regardless of the number of coronary arteries involved, with respect to mortality, subsequent MI, stroke, or bleeding. Using more potent antiplatelets instead of clopidogrel as well as non‑IRA revascularization during the index hospitalization appear to be important in the context of minimizing readmission rates.
- Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023; 44: 3720‑3826.
- Park D‑W, Clare RM, Schulte PJ, et al. Extent, location, and clinical significance of non‑infarct‑related coronary artery disease among patients with ST‑elevation myocardial infarction. JAMA. 2014; 312: 2019‑2027. | Crossref
- Sadowski M, Milewski K, Zandecki Ł, et al. Revascularization in patients with ST‑segment elevation myocardial infarction and multi‑vessel coronary artery disease: preliminary results from a large multicenter national registry. Pol Arch Intern Med. 2022; 132: 16315. | Crossref
- Sorajja P, Gersh BJ, Cox DA, et al. Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur Heart J. 2007; 28: 1709‑1716. | Crossref
- Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete versus lesion‑only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol. 2015; 65: 963‑972.
ARTICLE INFORMATION