Successful treatment of metachronous insulinoma in a patient with multiple endocrine neoplasia type 1 syndrome

 CC BY 4.0
CC BY 4.0
Successful treatment of metachronous insulinoma in a patient with multiple endocrine neoplasia type 1 syndrome
Insulinomas are neuroendocrine tumors (NETs) with an annual incidence of 0.7–4 cases per million.1 The majority of insulinomas present as solitary pancreatic lesions, while extrapancreatic localization is extremely rare (<1%).1 A total of 5%–10% of insulinomas occur with multiple endocrine neoplasia type 1 (MEN1) syndrome.1
We present a case of an 18‑year‑old woman with early‑onset MEN1 syndrome and metachronous insulinoma.
The first manifestation of MEN1 was a pancreatic insulinoma, diagnosed at the age of 11 years when she lost consciousness during hypoglycemic episode triggered by physical exercise. A biochemical diagnosis of insulinoma was confirmed (Supplementary material, Table S1) and a 1.5‑cm lesion within the pancreatic head was visualized on magnetic resonance imaging (MRI). The patient underwent successful tumor enucleation, and the hypoglycemic symptoms resolved. At the age of 16 years, the patient was diagnosed with hypercalcemia in the course of primary hyperparathyroidism (PHPT) and underwent subtotal parathyroidectomy. Genetic testing demonstrated a pathogenic variant (c.1432G>T, p.Glu478Ter) in the MEN1 gene. The same variant was previously identified in her father (diagnosed initially with multiple pancreatic insulinomas, then recurrent PHPT, nonfunctional pancreatic grade 1 NET, nonfunctional left adrenal adenoma, and multiple lipomas) and brother (currently 11 years old, diagnosed with PHPT).
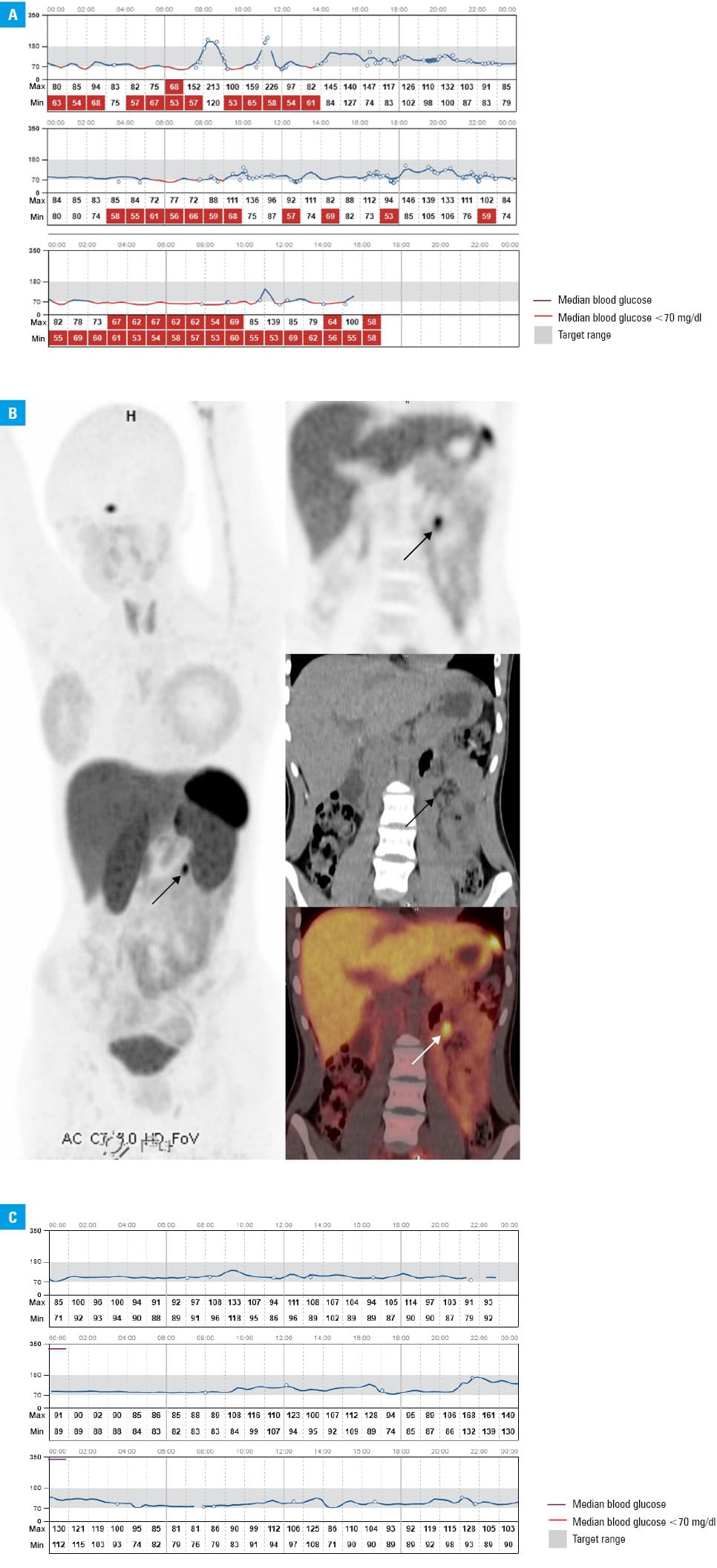
On admission to our center, the patient presented with episodes of tremor, loss of attention, and epigastric pain. A continuous Freestyle Libre 2 glucose monitoring system (CGM; Abbott Diabetes Care, Alameda, California, United States) was implemented, showing frequent hypoglycemic episodes (Figure 1A). Laboratory test results confirmed diagnosis of insulinoma on a fasting test (Supplementary material, Table S1). MRI did not identify any lesions within the pancreas, liver, and visceral lymph nodes. Endoscopic ultrasound (EUS) was also negative. Somatostatin receptor (SSTR) positron emission tomography/computed tomography (PET/CT; [68Ga]Ga‑DOTA‑0‑Tyr3‑Octreotate) showed pathological local uptake in the small intestine (maximum standardized uptake value, 11.5), without a corresponding structural mass on nonenhanced CT (Figure 1B). Enteroscopy showed a 10‑mm lesion in the jejunum. The patient subsequently underwent laparoscopic partial resection of the small intestine. Histopathology identified grade 1 NET located in the submucosal layer of the small intestine, that stained positive for synaptophysin (+++), chromogranin A (++), CD56 (+/–), Ki‑67 below 1%, and pT1 R0. After surgery, the plasma glucose level normalized (Figure 1C) and the patient’s quality of life improved.
To date, fewer than 30 cases of extrapancreatic insulinomas have been reported, predominantly in women, primarily within the gastrointestinal system, with no mention of association with MEN1 syndrome.2 Localization of insulinomas may be challenging because of their typically small size (47% <1 cm). Sensitivity of contrast‑enhanced CT and MRI approaches 90%, while EUS demonstrates sensitivity and specificity of 87% and 98%, respectively.3 Furthermore, EUS enables detection of small tumors below 5 mm.3 PET imaging of SSTR may be unreliable in the case of indolent insulinomas due to their lack of SSTR2 and SSTR5 overexpression.1 However, somatostatin receptor imaging PET/CT is particularly valuable in diagnosing a subgroup of insulinomas, namely, multiple, aggressive, extrapancreatic, and metastatic lesions.2-4 Due to the overexpression of the glucagon‑like peptide 1 receptor (GLP‑1R) in insulinomas (93%), GLP‑1R PET/CT is a useful, complimentary technique, if other imaging modalities fail to locate the lesion.1,3,5 Unfortunately, GLP‑1R PET/CT is not widely available.
Recent development of CGMs has significantly advanced diabetes management. Notably, CGM may be utilized as a complimentary tool for monitoring patients at a risk of hypoglycemia, for example, due to insulinoma. This technology offers multiple advantages, including reduced reliance on fingerstick testing, continuous assessment of glycemic levels, customizable alerts, and access to detailed glucose trends and patterns. Thus, a CGM may be beneficial in detecting hypoglycemia, which should be confirmed by measuring blood glucose concentration for clinical decision‑making.
Our report presents an extremely rare case of a patient with MEN1 syndrome and metachronous insulinoma, initially localized in the pancreas and, after 7 years, in the jejunum.
- Hofland J, Refardt JC, Feelders RA, et al. Approach to the patient: insulinoma. J Clin Endocrinol Metab. 2024; 109: 1109‑1118. | Crossref
- Guerrero‑Pérez F, Vilarrasa N, Huánuco LV, et al. Ectopic insulinoma: a systematic review. Rev Endocr Metab Disord. 2023; 24: 1135‑1146. | Crossref
- Hofland J, Falconi M, Christ E, et al. European Neuroendocrine Tumor Society 2023 guidance paper for functioning pancreatic neuroendocrine tumour syndromes. J Neuroendocrinol. 2023; 35: e13318. | Crossref
- Yang Y, Shi J, Zhu J. Diagnostic performance of noninvasive imaging modalities for localization of insulinoma: a meta‑analysis. Eur J Radiol. 2021; 145: 110016. | Crossref
- Kos‑Kudła B, Rosiek V, Borowska M, et al. Pancreatic neuroendocrine neoplasms ‑ update of the diagnostic and therapeutic guidelines (recommended by the Polish Network of Neuroendocrine Tumours) [in Polish]. Endokrynol Pol. 2022; 73: 491‑548. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION