Climate change and pollution: impact on blood pressure and kidneys
Key words: blood pressure, kidney injury, heat, particulate matter, water

 CC BY 4.0
CC BY 4.0
Climate change and pollution: impact on blood pressure and kidneys
Climate change and pollution have become major burdens for human health, and they will represent a growing issue in the future if nothing is planned to limit them. Epidemiologic evidence has clearly demonstrated significant associations between exposure to extreme climatic events, such as heat stress and pollution (air, noise, or toxic substances) and the occurrence of cardiovascular events. Indeed, climate and pollution have been shown to interfere with blood pressure regulation and to increase the risk of hypertension, and hence of cardiovascular complications, such as stroke, myocardial infarction, peripheral artery disease, or heart failure. For a long time, little attention has been paid to the renal impact of climate change and pollution, even though kidney function is very sensitive to these types of insults and mediates several of the clinical consequences of heat stress or pollution. Recently, more emphasis has been placed on the bidirectional relationship between the environment and kidney diseases. On the one hand, environmental change has an impact on the patterns of kidney diseases, and on the other hand, kidney replacement therapies, mainly chronic hemodialysis, are responsible for substantial carbon emissions and resource depletion. The purpose of this review is to discuss these kidney‑related issues to increase awareness of health care providers.
Introduction
In recent decades, there has been increasing evidence, mainly epidemiologic, that climate change and pollution pose a major burden for human health, and will become a challenging health issue in the future if no preventive interventions or measures are put in place.1,2 For example, several studies have demonstrated that exposure to excessive heat during heat waves, which are now more and more frequent, is associated with the development of acute illnesses leading to an increased risk of hospitalizations, and eventually death, due to cardiovascular events as well as to respiratory and kidney and electrolyte‑related complications.1-3 In a systematic review and meta‑analysis of 62 studies (30 included in the meta‑analysis), Faurie et al3 have reported that every 1 degree Celsius increase in temperature was associated with an increase in heat‑related morbidity and mortality by 18% (relative risk [RR], 1.18; 95% CI, 1.16–1.19) and 35% (RR, 1.35; 95% CI, 1.29–1.41), respectively. As expected, the risk was higher for people aged over 65 years.
Similarly, the accumulation of fine particulate matter with a diameter below 2.5 µm (PM2.5) in the ambient air or the contamination of water, soil, and food with pesticides, heavy metals, or plastics has been associated with the development of a host of acute and chronic adverse health outcomes in the population leading to an increased global morbidity and premature mortality.4-7
Ambient air pollution is the leading environmental risk factor, as a very large proportion (>90%) of the world population is exposed to air pollution, but the role of pollutants contaminating water and soils should not be neglected. Regarding the health impact of these environmental factors, 60% of pollution‑related diseases are cardiovascular ones, but pollution has also been associated with respiratory diseases, depression, anxiety disorders, and cancers.7,8 Of note, the health susceptibility and vulnerability to climate changes and pollution are particularly high among at‑risk populations, such as infants, pregnant women, older persons, patients with chronic diseases, and populations with a low socioeconomic status.6
The purpose of this brief review is to discuss the impact of climate change and environmental pollution on blood pressure (BP) regulation and hypertension. In addition, the contribution of these environmental factors to the development of kidney diseases will be discussed with a special emphasis on chronic dialysis as an important source of waste and pollutants.
Impact of climate change and pollution on blood pressure and hypertension
In recent European hypertension guidelines, environmental factors are clearly identified as significant reversible risk factors involved in the pathophysiology of hypertension.9,10 They also impact the regulation of BP. Physiologically, BP follows several rhythms according to, for example, the time of the day (circadian rhythm) or the season (seasonal variations). These rhythms are influenced by several internal and external factors, such as light, position, temperature, physical activity, food intake, and sleep. In this context, indoor as well as outdoor temperatures are known to modulate BP. Thus, an inverse linear relationship between outdoor temperatures and BP has been reported, with BP increasing with low temperatures and decreasing during hot seasons.11 The relationship between temperature and cardiovascular mortality is rather U‑shaped as exposure to extreme heat, as observed during heat waves, as well as low temperatures, is associated with an increased risk of cardiovascular events.12 The main reason is that heat stress reduces orthostatic tolerance and increases the risk of syncope because of the elevated skin blood flow and the venous pooling in the cutaneous circulation, leading to a reduction of total peripheral resistances, a decrease in venous return, and an increase in heart rate and workload. Heat stress has little impact on healthy people but represents a high risk for those with impaired thermoregulation, such as older individuals or patients with elevated BP. As discussed below, the ability to maintain an adequate fluid balance is crucial to reduce the risks associated with excessive temperatures. Among the mechanisms whereby acute heat episodes may increase the risk of cardiovascular events, one should mention sleep disturbances. Indeed, higher outdoor or indoor temperatures are generally associated with degraded sleep quality,13 and heat‑induced sleep alterations have been associated with a higher risk of hypertension,14,15 and short sleep duration (<5–6 h/night) is associated with an increased risk of death from coronary heart disease or stroke.16 However, long sleep durations (>8–9 h/night) were also associated with a higher cardiovascular risk.16 In this respect, high nocturnal temperatures have been associated with both higher nocturnal and daytime BP during the following days.17 The use of air conditioning is one way to prevent reductions in BP and to lower heat‑related mortality particularly among older patients.18 Thus, an increased use of air conditioning resulted in a reduction of the excess of deaths due to heat by 16.7% in Canada, 20% in Japan, 14.3% in Spain, and 16.7% in the United States. These Figures were partly due to the change in indoor temperature. In a large survey, a decrease in indoor temperature by 1 degree Celsius was associated with a reduction in systolic BP of 0.48 mm Hg (95% CI, –0.72 to –0.25).19
Pollution, whether from ambient air, traffic noise, or toxic substances, can also raise BP and favor the development of hypertension, as reviewed recently by Hahad et al.20,21 Numerous studies and several meta‑analyses have demonstrated that short‑term exposure to fine particles (PM <2.5 µm) results in a rapid increase in BP, and that the prohypertensive effect may persist leading to an increase in incident and prevalent hypertension if individuals are chronically exposed to these particles.20,22 Of note, passive exposure to smoking was found to be associated with masked hypertension.23 In the general population, short‑term exposure to PM smaller than 10 µm has been associated with a higher night‑time BP and a blunted systolic BP dipping.24 These effects were most pronounced in the hypertensive population. Significant interactions between the outdoor temperature and the cardiovascular risk due to exposure to fine particles have been reported.25 For example, a low temperature and a high air pollution act synergistically to increase BP in healthy adults.
Studies have also demonstrated that environmental noise exposure represents a significant risk factor for the development of hypertension, with a dose‑response relationship between the intensity of the noise and the risk of hypertension.20,26 Each 10 dB(A) increment of noise increases the risk of hypertension by about 6%.26 The recent COVID‑19 lockdown, which resulted in the complete interruption of air traffic in some areas, has provided a unique opportunity to assess the impact of aircraft noise exposure on cardiovascular parameters comparing 2 levels of noise. For example, before the COVID‑19 lockdown, sustained aircraft noise exposure was found to be related to higher office and night‑time diastolic BP, more advanced arterial stiffness, and unfavorable left ventricle diastolic function changes but not to an increased prevalence of hypertension.27 Moreover, the same authors reported a major impact of aircraft noise exposure during the night on sleep and ambulatory BP, noise‑exposed participants presenting distinctive sleep disturbances and an increased risk of insomnia.28 Insomnia among the noise‑exposed participants resulted in higher 24‑hour and night‑time systolic BP. During the 4‑month COVID‑19 lockdown, the decline in noise exposure (reduction from 61.7 to 47 dB during the day and from 55.4 to 43.4 dB during the night) was associated with a significant decreases in 24‑hour systolic and diastolic BP as well as pulse wave velocity in the exposed group, thereby demonstrating the negative impact of air traffic on individuals living in the surrounding of airports.29,30 This observation reminds us that most environmental impacts on health, as, for example, those associated with pollution, are reversible and even minor improvements in air quality can ameliorate public health.31
The role of kidneys in mediating the effects of climate change and pollution on the cardiovascular system
The link between climate change, pollution and cardiovascular health is complex and not yet fully understood. Numerous pathogenic mechanisms, derived essentially from epidemiologic studies, have been evoked but causal effects remain difficult to prove due to the multiplicity of confounding factors.32,33 Activation of neurohormonal systems, such as the sympathetic nervous system or the renin‑angiotensin system, systemic inflammation, endothelial dysfunction, release of cytokines, production of reactive oxygen species, or accumulation of nanoparticles in tissues are the most frequent mechanisms put forward to explain the cardiovascular impact of climate change and pollution, irrespective of its origin.32,33 When looking in more detail at these mechanisms, it appears that almost all of them act on or through kidney function. Hence, the kidneys may play an important role linking the climate change and pollution and cardiovascular events. In fact, this is not entirely surprising considering the crucial role of kidneys (in conjunction with the skin) in body temperature regulation and fluid and electrolyte maintenance.34 Moreover, the kidney is a target organ of heavy metal toxicity, because they filter, reabsorb, and concentrate divalent ions.35
As reviewed by De Vita et al,32 the renal response to stress constitutes an important intermediate factor linking extreme weather conditions and cardiovascular complications, including the risk of developing hypertension. This is also true when considering the impact of pollution on cardiovascular health.33 Indeed, although the initial insult of air pollution comes from the inhalation of small toxic particles, the pollution‑induced activation of inflammatory processes and neurohormonal systems has direct effects on kidney functions leading, for example, to sodium retention and the development of hypertension. This is illustrated by our observation that pollution‑induced alterations of the circadian rhythm of BP were preceded by a reduced ability of the kidney to excrete sodium during daytime suggesting disturbed circadian rhythms of renal sodium handling.24
Climate change and pollution and risk of acute and chronic kidney diseases
Climate change, which increases the frequency and intensity of extreme weather events, is a well‑recognized cause of acute kidney injury (AKI).34,36 It also represents a risk factor for developing chronic kidney diseases (CKD).37 The clinical presentation of heat‑associated diseases varies from a simple reversible dehydration associated with electrolyte abnormalities due to excessive sweating and insufficient water intake, to heat stroke, a more dramatic life‑threatening complication resulting in a high rate of emergency hospitalizations and a high risk of death.36 The classic renal manifestations of heat stroke are presented in Figure 1. The publication of a “CKD epidemic” affecting young male agricultural workers from communities of the Central America in 2014 has exemplified the renal consequences of a hot environment when combined with a strenuous work, insufficient access to water, and often an additional exposure to toxic products, such as plant protection chemicals and pesticides.38 In this epidemic, young individuals without traditional CKD risk factors (diabetes, hypertension, etc.) developed renal interstitial fibrosis, which could progress to end‑stage kidney disease (ESKD) and the need of renal replacement therapy. This entity is now recognized as chronic interstitial nephritis of agricultural communities. Since this original publication, multiple cases of the so‑called CKD of unknown origin have been reported in other hot areas of the planet, such as India or Sri Lanka, and the pathophysiology of the disease is now better understood.39 Today, heat‑related CKD is considered a global health issue accounting for more than 40 000 deaths annually.40,41
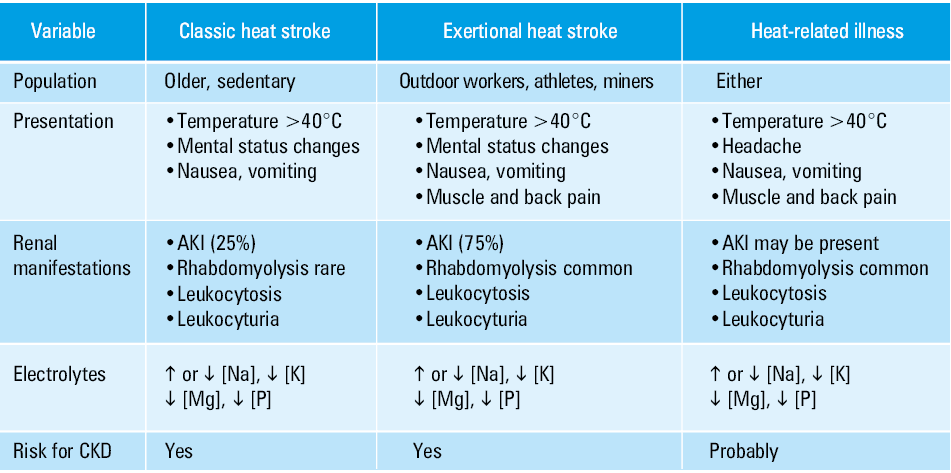
Abbreviations: ↑, increase; ↓, decrease; AKI, acute kidney injury; CKD, chronic kidney disease
One renal disease strongly influenced by changes in temperature is kidney stone disease. The incidence and prevalence of kidney stones increase when the weather is hot with the strongest associations estimated for lags of only a few days.42 There is clearly a global north‑south gradient in the incidence of kidney stone disease due to the temperature and humidity levels.43,44 Moreover, there is sex difference in the incidence of kidney stones, with a higher risk in men than in women.44 However, a recent trend is an increase in kidney stone incidence in women.45 Studies have shown that kidney stone episodes increase several folds in workers exposed to high ambient temperatures, when compared with individuals working at room temperature.46 Since heat and dry climate are significant risk factors for lithogenesis, the incidence of kidney stones is projected to increase significantly in the next decades in relation to climate change.43,47,48
The impact of climate change on kidney events is not limited to the association with heat stress. Indeed, recent observations indicate that pollution participates in increasing the incidence of CKD and favoring CKD progression. When compared with cardiovascular or respiratory diseases, the association between pollution and kidney function has long been overlooked. In the United States, investigators have evaluated the association of the concentration of PM below 2.5 µm and the risk of incident estimated glomerular filtration rate (eGFR) lower than 60 ml/min/1.73 m2, incident CKD, eGFR decline by 30% or more, and ESKD over a median follow‑up of 8.52 years in a large cohort of 2 482 737 veterans.49 In this analysis, a 10 mg/m3 increase in PM2.5 concentration was associated with significantly greater risks of eGFR below 60 ml/min/1.73 m2 (+21%), CKD (+27%), an eGFR decline by at least 30% (+28%), or ESKD (+26%). Moreover, in the users of the Medicare system aged over 65 years, high annual air pollution levels were associated with an increased risk of the first hospital admission related to diseases of the kidney and urinary system or CKD.50
As reviewed recently by Lao et al,51 short‑term exposure to air pollution increases the risk of kidney disease–related events, such as hospital admissions and death. As discussed previously, during long‑term exposure to pollutants, the pathogenic mechanisms activated by pollution, particularly inflammation, can contribute to the worsening of existing kidney diseases, which are also due to the activation of inflammatory processes. In a recent analysis of 2 cohorts of patients with glomerular diseases, participants exposed to higher levels of pollutants had lower eGFR, were older, and had more likely a low socioeconomic status.52 In a fully‑adjusted model combining both cohorts, kidney disease progression was clearly associated with PM2.5 concentration (hazard ratio, 1.55; P = 0.0489). In the analyses of the Atherosclerosis Risk In Communities (ARIC) cohort, a prospective community‑based cohort following 15 792 adults across 4 sites in the United States, PM2.5 levels were not associated with eGFR at baseline, but an increase in annual average PM2.5 level by 1 μg/m3 was associated with higher urinary albumin excretion and a greater risk of incident CKD.53 In Chinese analyses of a very large series of patients with renal biopsies (n = 71 151), a sustained exposure to high concentrations of PM2.5 was associated with an increased risk of membranous nephropathy but not immunoglobulin A nephropathy.54
Taken together, these observations suggest that pollution should receive more attention in the assessment of the causes of CKD and of the reasons why CKD is progressing despite well‑controlled parameters such as BP or albuminuria.
Finally, apart from heat and pollutants, other climatic factors linked to kidney diseases may be considered.55 This is the case, for example, of alterations in rainfall patterns with more frequent flooding, which can lead to water contamination and to an increased incidence of infectious diarrhea, a known cause of AKI, particularly among children. In tropical and subtropical regions, mosquitoes can proliferate at warmer temperature, and this can increase substantially the rate of vector‑borne diseases, such as leptospirosis, dengue, malaria, or Zika.56 Today, some of these infections have been diagnosed in European regions that had never been exposed to them before. When AKI occurs in these diseases, the mortality rate may be relatively high.
Renal replacement therapy and pollution and climate change
When CKD patients reach the latest stage of their disease, for example, ESKD, they can either receive a kidney transplant or be included in a chronic dialysis care program (hemodialysis or peritoneal dialysis), 2 life‑saving therapies. There are several links between ESKD therapies and climate change and pollution. The first is the availability of these treatments in low‑income countries, as dialysis and transplantation are not universally available. The issue is particularly concerning in the countries frequently exposed to climate disasters, such as hurricanes, floods, bushfires, or heatwaves and also to water shortages.57 In these climatic environments, the access to renal care, when available, may suddenly be compromised and renal patients become very vulnerable if they cannot follow their treatment on a regular basis. Similar events sometimes occur in high‑income countries with similar health consequences, as observed recently in some European countries (Germany,58 Spain59). The second link is the impact of extreme heat events on the risk of death among patients receiving dialysis. In a very large retrospective survey in the United States, Blum et al60 have shown that extreme heat events (defined as a time‑updated heat index [a humid‑heat metric] exceeding 40.6 °C for ≥2 days or 46.1 °C for ≥1day) increase the risk of death of dialysis patients by 18%, with a higher mortality risk in southern states.60 These data confirm the fragility of dialysis patients when facing extreme heat events.
As stated by Barraclough et al,61 there is a bidirectional relationship between the environment and kidney diseases. On the one hand, environmental change has a growing impact on the patterns of kidney diseases, as discussed above. But on the other hand, kidney replacement therapies, especially chronic hemodialysis, are responsible for substantial carbon emissions and resource depletion, and are far from being environment‑friendly procedures. There are at least 3 major environmental issues with the provision of chronic hemodialysis to ESKD patients: 1) the use of very high volumes of water, 2) the generation of a large amount of care‑related waste, and 3) the consumption of power.61 Table 1 shows the average Figures for chronic hemodialysis and peritoneal dialysis for these 3 components. Note that for peritoneal dialysis (PD), automated PD consumes more energy than continuous ambulatory PD.62 In addition, one could also consider the energy needed to transport patients to dialysis centers or to deliver dialysis material to patients treated at home. Finally, dialysis machines contain plastic, metal, mixed materials, and electronic components with a negligible potential of recycling, thereby contributing to waste production.63 In 2013, we calculated the annual volume of water and the production of waste at our dialysis center taking care of 80 patients. In 1 year, the center used the equivalent of 2 Olympic swimming pools of water and produced 55 tons of care waste.64 If these Figures are multiplied by the number of patients on dialysis worldwide (around 3 664 000 patients in 2020), this represents an enormous ecological burden. For example, with 3.7 million patients on hemodialysis, the annual water consumption would be estimated at over 280 million m3. One issue is that in most dialysis centers, the water rejected from the reverse osmosis system just goes down the drain. Regarding material waste, for economic and safety reasons, no trend toward reducing single‑use equipment to lower waste production is anticipated. In Australia, a survey published in 2019 showed that only 10% of the units used renewable sources of energy, and 25% recycled reverse osmosis reject water for use elsewhere.65 Therefore, the problem remains unresolved.
Variable | Hemodialysis | Peritoneal dialysis |
Numbers adapted from58-60
Abbreviations: APD, automated peritoneal dialysis; CAPD, continuous ambulatory peritoneal dialysis | ||
Water usage | 300–600 l/session
46 000–93 600 l/year | 8–12 l/day
2920–4380 l/year |
Waste production | 1.5–1.8 kg/session
~390 kg/year | 1.8–2.5 kg/day
~617 kg/year |
Power usage | 6.2–20 kWh/session | – |
Carbon footprint | 4–10 CO2 eq/patient/year | CAPD, 1245 kg CO2 emission/year |
APD, 1992 kg CO2 emission/year | ||
Waste associated with the material | Dialysis machines | Plastic bags |
Total weight of a machine | 125–145 kg | APD, 34 kg/CO2 emission |
Plastic | 34–40 kg (28%) | 180 l water/1 kg plastic |
Metal | 19–27 kg (15%–19%) | – |
Electrical and electronic material | 8–20 kg (6%–13%) | APD, 213 kg CO2 emission |
CAPD, 0 | ||
Mixed material | 56–64 kg (40%–50%) | – |
However, the recognition of the large carbon footprint of chronic hemodialysis by some nephrology experts has been at the origin of the concept of green nephrology, with the creation in 2009 of the first network of dialysis stakeholders in the United Kingdom aiming at improving the sustainability of dialysis. This program anticipated very important cost savings (>10 million USD). Thereafter, several national and international initiatives and recommendations have been published to support this green nephrology concept.61,66-69 Interestingly, the concept has now been extended to intensive care units (ICUs) with the creation of green ICU projects to reduce waste and develop sustainable ICUs.70
The global trend toward sustainable hemodialysis was somehow successful in demonstrating the multiplicity of opportunities for improvements at all levels of dialysis management, as illustrated in Table 2. Thus, in France, the implementation of a continuous monitoring system measuring electricity, water consumption, and care‑related waste production combined with updates of energy sources and water treatment systems has enabled to reduce the consumption of electricity by 29% and of water by about 50% over a 13‑year period.71 In addition, the care‑related waste decreased from 1.8 to 1.1 kg per session. To reduce the need for water, several new dialysis machines are being developed that could offer the possibility to perform home dialysis with a minimum volume of water (<10 l per session) using the sorbent technology.61,72 Ultimately, the availability of wearable or implantable dialysis systems could circumvent the obstacle of water consumption.
Problem | Strategy | Opportunities |
Water usage | Reuse or recycle | Gardening, toilets, steam production, agriculture (after filtration) |
Reduce the use of water |
| |
Power usage | Alternative sources of electricity |
|
Waste production |
|
|
Global issues | Increase awareness and education |
|
Develop low‑energy, low‑waste technologies |
| |
| – | |
|
|
Meanwhile, valuable suggestions have been proposed for the most effective use of the dialysis water applying the “3R” (reduce, reuse, recycle) concept, such as the use of the waste water for gardening, aquaponics, or even simply for toilet flushing.73 This water, after treatment, could also be used as a fertilizer in agriculture.74,75 Innovative solutions have also been proposed to vary the source of energy, using for example solar energy or heat pumps, and to reduce the amount of dialysis‑care waste introducing waste management programs in dialysis units.76
Conclusions
Today, there is less and less doubt that climate change and pollution, essentially generated by human activities, have deleterious effects on health, increasing the morbidity and mortality associated with respiratory and cardiovascular diseases. Talking about environment and pollution in health is not just a fashionable topic.77 Several outstanding reviews have demonstrated that nephrology is no exception.36,50,56,61,72
A large, multinational survey of 4654 health professionals has assessed the views of climate change as a human health issue.78 From this survey, it appears that health care professionals generally understand and agree that climate change and pollution are important and represent a growing source of health harm. Nevertheless, few participants were engaged in specific activities to limit the impact of climate change or pollution on health. Their lack of engagement was explained essentially by personal, professional, and societal barriers, with time constraints being the most frequently reported barrier. In the field of nephrology, another cross‑sectional survey was performed among health care providers to understand the knowledge, attitude, and practice of professionals on the relation between climate change and kidney health.79 More than 900 people from 108 countries, with 64% from lower- or middle‑income countries, participated in the survey. Nearly all of them agreed that climate change is happening but less than half of them had knowledge on the impact of climate and environmental changes on kidney health and of the environmental effect of kidney care. Interestingly, the participants from low- and middle‑income countries had a greater awareness and knowledge about climate issues than those from high‑income countries. Globally, few renal health care providers (14%) were involved in climate change and kidney health initiatives. The results of these surveys demonstrate that there is still a long way to go to implement sustainable nephrology, particularly in low- and middle‑income countries, where the situation is the most challenging.80 But now that we know the risk, it is time to act.
- Bell ML, Gasparrini A, Benjamin GC. Climate change, extreme heat, and health. N Engl J Med. 2024; 390: 1793‑1801. | Crossref
- Ebi KL, Capon A, Berry P, et al. Hot weather and heat extremes: health risks. Lancet. 2021; 398: 698‑708. | Crossref
- Faurie C, Varghese BM, Liu J, Bi P. Association between high temperature and heatwaves with heat‑related illnesses: a systematic review and meta‑analysis. Sci Total Environ. 2022; 852: 158332. | Crossref
- Beelen R, Raaschou‑Nielsen O, Stafoggia M, et al. Effects of long‑term exposure to air pollution on natural‑cause mortality: an analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet. 2014; 383: 785‑795.
- Lelieveld J, Evans JS, Fnais M, et al. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature. 2015; 525: 367‑371. | Crossref
ARTICLE INFORMATION