Pulmonary embolism is often associated with deep vein thrombosis of the lower limbs. We present a case of a patient with an atypical cause of pulmonary embolism, the identification of which modified the therapeutic approach.
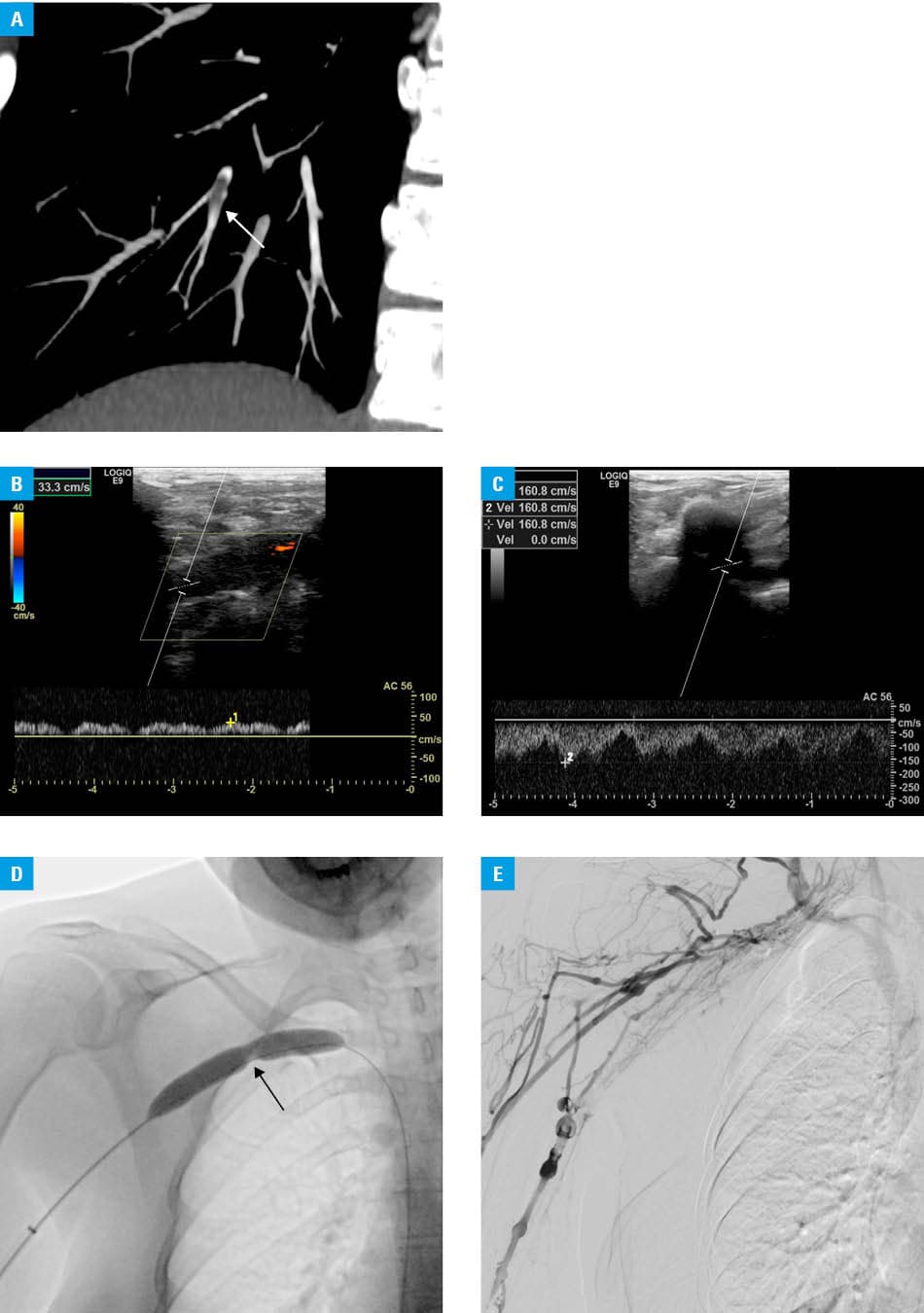
A 39‑year‑old female veterinary physician with arterial hypertension was admitted to a hospital due to rapidly increasing edema, pain, redness, dilation of superficial veins, and paranesthesia of the right arm. The symptoms developed a few days after she sustained an injury while professionally caring for a husky. Computed tomography angiography showed a thrombus in the peripheral branches of segments 9 and 10 of the right lung and segments 6, 9, and 10 of the left lung, as well as dilation of the right subclavian, axillary, and brachial veins (Figure 1A).
On admission, the patient was in a good general condition. Physical examination confirmed patient complaints and additionally identified thickening along the medial side of the arm in the right armpit. The pulse in the right brachial, radial, and ulnar arteries was palpable, indicating no arterial compression.
Biochemical tests showed an elevated D‑dimer concentration (1730 ng/ml; reference range <500 ng/ml). Ultrasonography identified thrombosis of the right subclavian, axillary, and partially brachial veins.
The patient received low‑molecular‑weight heparin, then 2 × 15 mg of rivaroxaban daily, but acceptable improvement was not achieved—pain, paresthesia, and passive hyperemia were still present. Rapid enlargement of edema was provoked by simple physical activities.
The key to treating pulmonary embolism and venous thrombosis in this patient was considering venous thoracic outlet syndrome (vTOS) diagnosed a few months earlier based on computed tomography showing the right subclavian vein compressed to 4.5 mm by the inferior margin of the clavicle, superior part of the first rib, and anterior scalene muscle.1 In the diagnosis of vTOS, Doppler ultrasound of the subclavian vein was performed, showing increased flow velocity during changes in arm position (Figure 1B and 1C).
Due to a lack of improvement, endovascular recanalization of the obstructed right subclavian vein was performed (Figure 1D). A few days later, the patient underwent resection of the first right rib and scalenectomy. Control phlebography showed occlusion of the right subclavian and axillary veins (Figure 1E). However, blood flow was normal due to collateral circulation. The patient received enoxaparin for the postrevascularization period (3 months) and was discharged home in a good condition. The choice of enoxaparin instead of direct oral anticoagulants was justified by the patient’s preference due to previous ineffectiveness of rivaroxaban.2
The objective of this case is to highlight that without fully effective treatment, the patient would have faced disability that would have made her unable to pursue her profession. However, prolonged compression, vein damage, and delay in endovascular treatment may be reasons why the radiological procedure had failed. Historically, systemic anticoagulation was used to treat vTOS, leading to long‑term morbidity in most patients.3 Currently, declotting with catheter‑directed thrombolysis is the preferred initial treatment in symptomatic patients.4 Further treatment includes definitive thoracic outlet decompression surgery—an approach that leads to successful and persistent outcomes.5
- Sanders RJ, Hammond SL, Rao NM. Diagnosis of thoracic outlet syndrome. J Vasc Surg 2007; 46: 601‑604. | Crossref
- De Kleijn RJCMF, Schropp L, Westerink J, et al. Current treatment strategies for primary upper extremity deep venous thrombosis; a retrospective observational multicenter case series. Front Surg. 2022; 22: 1‑7. | Crossref
- Urschel HC, Razzuk MA. Paget‑Schroetter syndrome: what is the best management? Ann Thorac Surg. 2000; 69: 1663‑1668. | Crossref
- Lee JT, Karwowski JK, Harris EJ, et al. Long‑term thrombotic recurrence after nonoperative management of Paget‑Schroetter syndrome. J Vasc Surg. 2006; 43: 1236‑1243. | Crossref
- Davies MG, Hart JP. Endovascular management of acute and subacute venous thoracic outlet syndrome. Front Surg. 2024; 11: 1‑6. | Crossref
ARTICLE INFORMATION