Introduction
Inflammatory bowel disease (IBD), which primarily includes ulcerative colitis (UC) and Crohn disease (CD), is a chronic disease of the digestive system.1 The incidence of IBD is stabilizing in many regions; however, due to the young age of onset and low mortality rates, its prevalence continues to increase.2 In Poland, the incidence of UC and CD is 12.5 and 4.7 cases per 100 000 inhabitants, respectively, and the total number of IBD patients exceeds 100 000.3
The fact that IBD has a significant impact on patient quality of life (QoL) is well documented, and many studies have confirmed a reduction in QoL, including sexual life, in this patient group.4-6 Most patients, regardless of the disease severity, have high levels of anxiety and fear.4,5 This is due to the emotional burden associated with factors such as loss of bowel control, impaired body image, fear of sexual inadequacy, social isolation, fear of dependency, the feeling of not reaching one’s full potential, and fear of stigmatization.5
Sexuality is often disturbed in patients with IBD, an important issue given that most diagnoses are made in young adults. At present, it is estimated that the disease contributes to problems with intimate relationships in up to 40% of patients with IBD.6 In men, erectile dysfunction is most common, affecting 10%–53% of patients in selected age groups.7 In women, pleasure disorders, disorders of arousal, orgasmic disturbances, and pain during sexual intercourse occur,7 affecting between 45% and 63% patients from this group.8
There is a clear need for research into patient experiences of coping with the challenges of everyday life, and the extent to which they receive support from health care professionals.6 A better understanding of the factors contributing to poor sexual function in patients with IBD will minimize the adverse psychosocial events.7 To our knowledge, there is currently a limited number of articles investigating the quality of sexual life in IBD patients in the Polish population.
Our study aimed to investigate the impact of IBD on the frequency and types of sexual dysfunction and depression in patients with IBD as compared with healthy individuals, as well as to assess the extent of informational interventions provided by physicians in this context to date. A better understanding of the problems of patients with IBD related to functioning in the sexual domain could facilitate conversations about intimate issues and enable earlier and more appropriate disclosure of relevant information.
Patients and methods
Study design
The study was conducted among patients diagnosed with IBD at the Department of Gastroenterology, University Hospital in Kraków, and individuals with IBD who were members of social groups on the Facebook platform. The control group consisted of healthy volunteers matched for sex and age recruited through social groups on Facebook. Consent to participate in the study was obtained as an integral part of the questionnaire completed by the respondents. The survey was conducted electronically between July 2021 and July 2022, using the Microsoft Forms application on a separate website that did not require registration or provision of personal data. The participants were informed upfront that they could withdraw from completing the survey at any time.
The research instrument was a survey consisting of a general section on sociodemographic data, selected questions on the course of IBD and comorbidities, the Female Sexual Function Index (FSFI) or the International Index of Erectile Function (IIEF‑5), as well as the Beck Depression Inventory (BDI‑II).
The FSFI is a 19‑question self‑reported survey on female sexual function.9 It comprises 6 domains of desire, arousal, lubrication, orgasm, satisfaction, and pain. The maximum score is 36 points, and scores below 26.55 indicate clinically relevant sexual dysfunction.
The IIEF‑5 is a 5‑item questionnaire designed to diagnose the presence and severity of erectile dysfunction.10 It includes items relating to erectile function and sexual satisfaction. The established cutoff score is 21 (range, 5–25), and was discriminated best by the presence or absence of erectile dysfunction (sensitivity, 0.98; specificity, 0.88), which was classified into 5 severity levels, from none (22–25) to severe (5–7).
The BDI‑II is a widely used, self‑reported inventory of 21 items scored from 0 to 3, based on the feelings over the past 2 weeks, developed to measure the severity of depression in adolescents and adults.11 BDI‑II is a comprehensive indicator of the severity of depression, and it is proven to be reliable and valid among different populations and cultural groups. The authors of the original instrument proposed that the cutoff between minimal or no depression and mild depression is 14 points.
Inclusion and exclusion criteria
The inclusion criteria were a diagnosis of IBD and age between 18 and 65 years. The exclusion criteria were partial or incorrect completion of the questionnaire, pregnancy and breastfeeding, diagnosis of diabetes, respiratory failure, circulatory failure, alcohol or drug abuse, or poststroke condition reported in the sociodemographic section of the survey. The participants in the control group had to fulfill the same criteria, and could not have a diagnosis of IBD.
Statistical analysis
Numerical variables were expressed as median and interquartile range (IQR) and compared using the Mann–Whitney test. The χ2 test was used for nominal variables. The Spearman rank correlation coefficient was calculated to determine the presence of correlations between the data sets. Two‑tailed P values below 0.05 were considered significant. Statistical analysis was conducted using online statistical software Statistics Kingdom.12
Ethics
The study received an approval of the Jagiellonian University Bioethics Committee (1072.6120.118.2021).
Results
We collected 111 questionnaires from patients with IBD (study group) and 64 questionnaires from healthy participants (control group). According to the exclusion criteria, 7 patients with IBD and 9 patients from the control group were excluded prior to the statistical analysis. Therefore, 104 patients with IBD and 55 controls were included in further analysis.
General characteristics of the participants
The study group included 73 women (70.2%) and 31 men, and in the control group there were 44 women (80%) and 11 men (P = 0.18). Median (IQR) age was 30 (25–36) years in the IBD group and 28 (25–37) years in the control group (P = 0.78). As many as 81 patients (77.9%) and 44 controls (80%) were in a relationship (P = 0.76).
Characteristics of patients with inflammatory bowel disease
Supplementary material, Table S1 contains detailed data on the studied populations, such as the presence of a stoma, fistulas, remission of the disease, and a history of previous surgery, as well as data on topics related to sex and reproduction that were discussed during medical visits.
We found that 4 patients (4%) talked to their doctors about their sexual problems after IBD diagnosis, and 3 individuals (3%) talked about possible sexual dysfunction related to IBD.
Sexual dysfunctions in women
The women with IBD were more likely to experience discomfort or pain during and after vaginal penetration. The differences between the IBD group and healthy controls in sexual desire or interest were minor (P = 0.06). According to the questionnaire, 57.5% of the women with IBD (n = 42) suffered from sexual dysfunction. Detailed data can be found in Supplementary material, Table S2.
Sexual dysfunction in men
In the male sexual dysfunction part of the questionnaire, the patients with IBD scored lower in a number of the studied parameters, indicating greater severity of sexual dysfunction and poorer quality of sexual life than in the healthy controls. Significant differences between the groups were achieved for problems with maintaining an erection after penetration, as well as maintaining an erection until the end of sexual intercourse. As many as 13 patients with IBD (41.9%) scored 21 points or less, indicating sexual dysfunction. Detailed data can be found in Supplementary material, Table S3.
Psychological condition
When comparing the mental health parameters between the patients with IBD and the control group using the BDI‑II scale, we found a higher score in the individuals with IBD, indicating their poorer mental functioning in each domain assessed by the test. Moreover, all reported differences were significant except for “sadness, suicidal thoughts or wishes” and “loss of interest in sex.” In as many as 66 patients with IBD (63.5%) the questionnaire showed mild, moderate, or severe depression (cutoff of 14 points). Detailed data on mental health can be found in Supplementary material, Table S4.
Comparison of outcomes in the patients with ulcerative colitis and Crohn disease
In women with UC, the median (IQR) levels of sexual interest (4 [2–5] vs 4 [4–5]; P = 0.02), overall satisfaction with sexual life (3 [2–4] vs 4 [3–5]; P = 0.02), and sexual arousal (4 [3–4] vs 4 [4–5]; P = 0.03) were lower than in the controls. We did not perform these analyses in men due to the small group sizes. Detailed data are available in Supplementary material, Tables S5 and S6.
Relationships between the psychological condition and sexual disorders
The relationship between the psychological condition of the patients and the intensity of their sexual dysfunction was investigated separately for women (n = 73) and men (n = 31). In both groups, the occurrence of more severe sexual dysfunction positively correlated with a worse psychological condition (R = –0.334; P = 0.004 for women and R = –0.593; P <0.001 for men). The data are shown in Figure 1A and 1B.
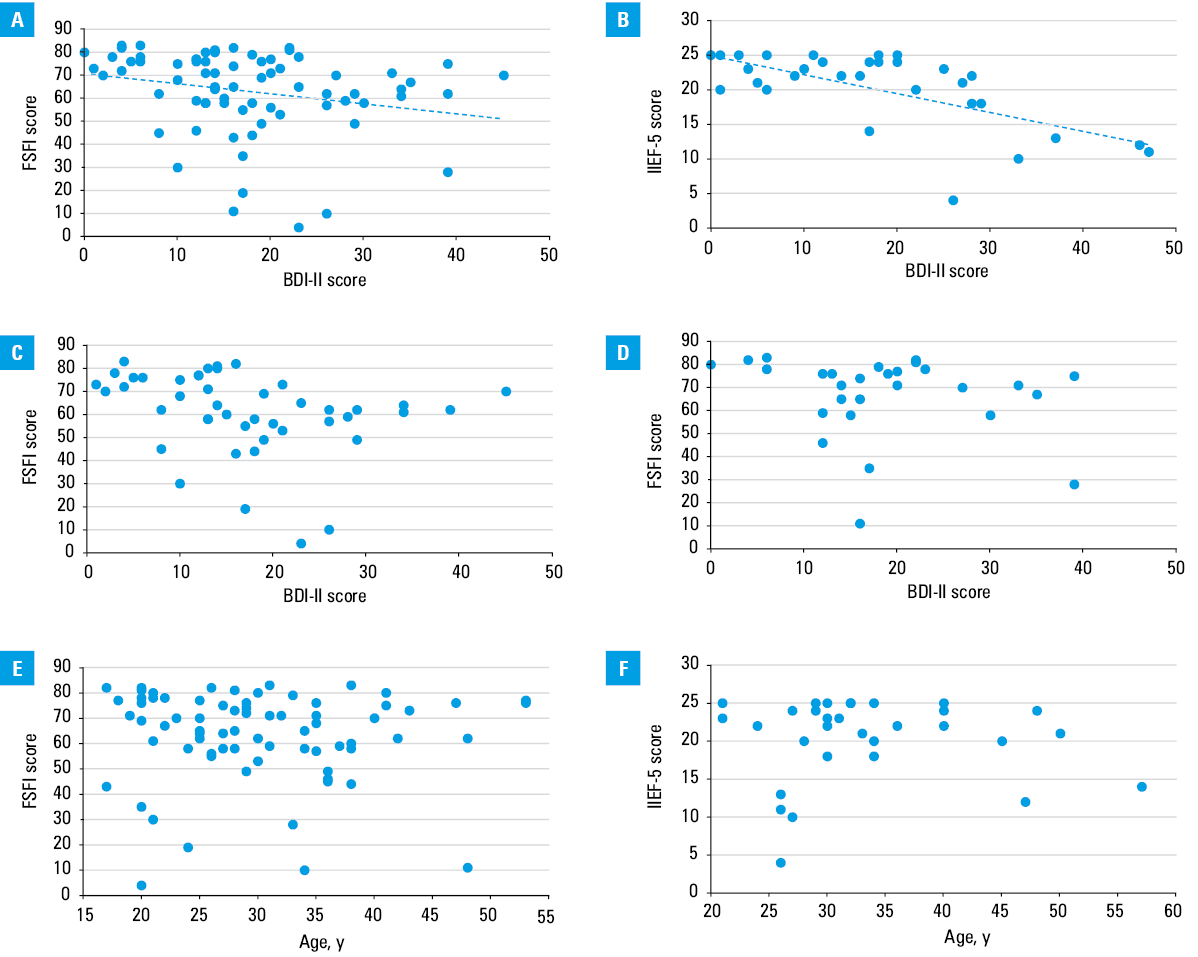
Abbreviations: BDI‑II, Beck Depression Inventory; FSFI, Female Sexual Function Index; IIEF‑5, International Index of Erectile Function
We also investigated the correlation between the psychological condition and sexual disorders depending on the primary diagnosis (CD vs UC). In women suffering from CD (n = 45), the correlation coefficient R was –0.431 (P = 0.003), and in those diagnosed with UC (n = 28) it was –0.226 (P = 0.25). The data are shown in Figure 1C and 1D.
Due to small group sizes, we did not conduct these analyses in men.
Correlation between sexual disorders and age
The severity of sexual disorders did not correlate with age of the patients, as the correlation coefficients were –0.097 (P = 0.41) for women and –0.022 (P = 0.9) for men. These data are shown in Figure 1E and 1F.
Discussion
This is one of the first Polish studies showing the prevalence of sexual dysfunction in IBD patients. In women, discomfort or pain during and after vaginal penetration was most frequently reported, while men had difficulty maintaining an erection to complete an intercourse and after penetration. Our study also showed that the intensity of sexual dysfunction in IBD patients correlated with their psychological condition, which was often worse than in the healthy population.
IBD can affect intimacy, sexual activity, and satisfaction, as well as the development and maintenance of personal relationships.6,13,14 Problems reported by men include erectile function, orgasmic function, sexual desire, and overall satisfaction.15 The most common sexual dysfunctions in women are desire, arousal, and orgasmic disorders, as well as pain during sexual intercourse.7,8 The global prevalence of sexual dysfunction is thought to be between 45% and 63% in women with IBD and 15% and 25% in men with IBD.8
Describing sexual dysfunction in men, it is worth noting that the median (IQR) total score that the IBD patients in our study achieved in the IIEF‑5 questionnaire (22 [18–24] points) remained within the normal range. However, the patients had problems maintaining an erection. A meta‑analysis by Wu et al16 also showed that IBD patients had a significantly increased prevalence of erectile dysfunction. Additionally, this risk was exacerbated by surgery, increased disease activity, and comorbid depression. Men not only complain of decreasing libido and problems with sexual intercourse but sometimes also fear it and even try to avoid it.17 Patient sexual functions may be impaired due to side effects of medications, changes in body image, active inflammation, or surgical procedures.18
When discussing sexuality of women with IBD, it is crucial to acknowledge that sexual problems are prevalent and can impact intimacy, sexual activity, and satisfaction, as well as the formation and maintenance of personal relationships.13 Notably, women with IBD in our study, despite experiencing discomfort or pain during vaginal penetration, have shown remarkable resilience in maintaining satisfaction with their sexual activity, describing themselves as satisfied with their sex life. However, subjective perceptions of attractiveness, femininity, and satisfaction with their appearance are often compromised in women with IBD, leading to dissatisfaction with body image and poorer sexual function.19
According to our study, only a small group of 19.2% of patients have ever talked to their doctor about the impact of IBD on reproduction. This number is still 5 times higher than the number of patients who have spoken to a doctor about sexual dysfunctions. It should be noted that patients with IBD have fewer children than their peers in the general population.14,20
An essential aspect of our study is a worse mental status of IBD patients, as compared with healthy controls, in all analyzed areas. This shows that IBD has a significant impact on the cognitive status of the patients. Furthermore, a survey by Timmer et al15 showed that depressed mood has the most significant impact on the impairment of sexual function, not only in patients with IBD.
It is important to emphasize that conversations about sexual dysfunctions with health care providers are currently infrequent. In our study, only a few patients discussed sexual problems with a doctor after their IBD diagnosis, and even fewer spoke about possible sexual dysfunctions related to IBD.
Sexual problems are common in patients with IBD, but there are effective methods to alleviate them. Several factors, including disease activity, medication side effects, body image changes, surgical procedures, and psychological well‑being may influence sexual dysfunction in IBD.18 In women, pelvic floor physiotherapy and biofeedback can be helpful.13 Pregnancies in patients with IBD should be closely monitored while the inflammatory disease remains in remission. Preconception counselling can be highly valuable.14 In men, phosphodiesterase‑5 inhibitors are the first choice for erectile dysfunction.17 Young men with IBD should also consider sperm banking before surgery.20 In addition, sulfasalazine, a drug that can impair male fertility, should be replaced with mesalamine at least 4 months before attempting conception.20 Close cooperation between the patient and their attending physician is crucial in the treatment of sexual dysfunction. Comprehensive counselling and psychological support, which play a significant role in helping patients understand the pathophysiology of the disease and reduce the anxiety and fear associated with these challenges, should be emphasized.13,20
Conclusions
IBD can adversely impact sexual function in both women and men. Women may experience discomfort or pain during vaginal intercourse, while men might struggle with maintaining an erection. The severity of sexual dysfunction is often linked to depression that affects many IBD patients. Holistic care for IBD patients should address all aspects of their QoL, including sexual health. However, sexual issues remain a challenging and sensitive topic, leading many patients to hesitate about seeking medical assistance. Meeting the needs of patients with IBD requires more open conversations about sexual dysfunctions.
- Ananthakrishnan AN. Environmental risk factors for inflammatory bowel diseases: a review. Dig Dis Sci. 2015; 60: 290‑298. | Crossref
- Windsor JW, Kaplan GG. Evolving epidemiology of IBD. Curr Gastroenterol Rep. 2019; 21: 40. | Crossref
- Zagórowicz E, Walkiewicz D, Kucha P, et al. Nationwide data on the epidemiology of inflammatory bowel disease in Poland between 2009 and 2020. Pol Arch Intern Med. 2022; 132: 16194. | Crossref
- Bernabeu P, Belén‑Galipienso O, van‑der Hofstadt C, et al. Psychological burden and quality of life in newly diagnosed inflammatory bowel disease patients. Front Psychol. 2024; 15: 1334308. | Crossref
- Kim YS, Jung SA, Lee KM, et al. Impact of inflammatory bowel disease on daily life: an online survey by the Korean Association for the Study of Intestinal Diseases. Intest Res. 2017; 15: 338‑344. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION