Myocardial infarction with nonobstructive coronary arteries: clinical characteristics and role of the N-terminal pro–B-type natriuretic peptide to troponin ratio as a novel diagnostic tool
Key words: acute coronary syndrome, myocardial infarction with nonobstructive coronary arteries, myocardial infarction, NT-proBNP/troponin ratio



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Myocardial infarction with nonobstructive coronary arteries: clinical characteristics and role of the N-terminal pro–B-type natriuretic peptide to troponin ratio as a novel diagnostic tool
Introduction: Myocardial infarction (MI) with nonobstructive coronary arteries (MINOCA) encompasses heterogeneous conditions resulting in myocardial damage without significant coronary artery obstruction. Understanding its prevalence and risk factors is essential for developing diagnostic and therapeutic strategies.
Objectives: This study aimed to evaluate the prevalence, outcomes, and risk factors of MINOCA and to investigate the N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) to troponin ratio as a novel early diagnostic tool.
Patients and methods: This single‑center, retrospective study included 194 patients with acute coronary syndrome diagnosed on invasive coronary angiography (ICA) over 6 months. The patients were categorized as MINOCA or obstructive or occlusion MI (OOMI) based on ICA and optical coherence tomography findings. Detailed data on clinical characteristics, laboratory test results, NT‑proBNP/troponin ratio, and the SYNTAX score were collected.
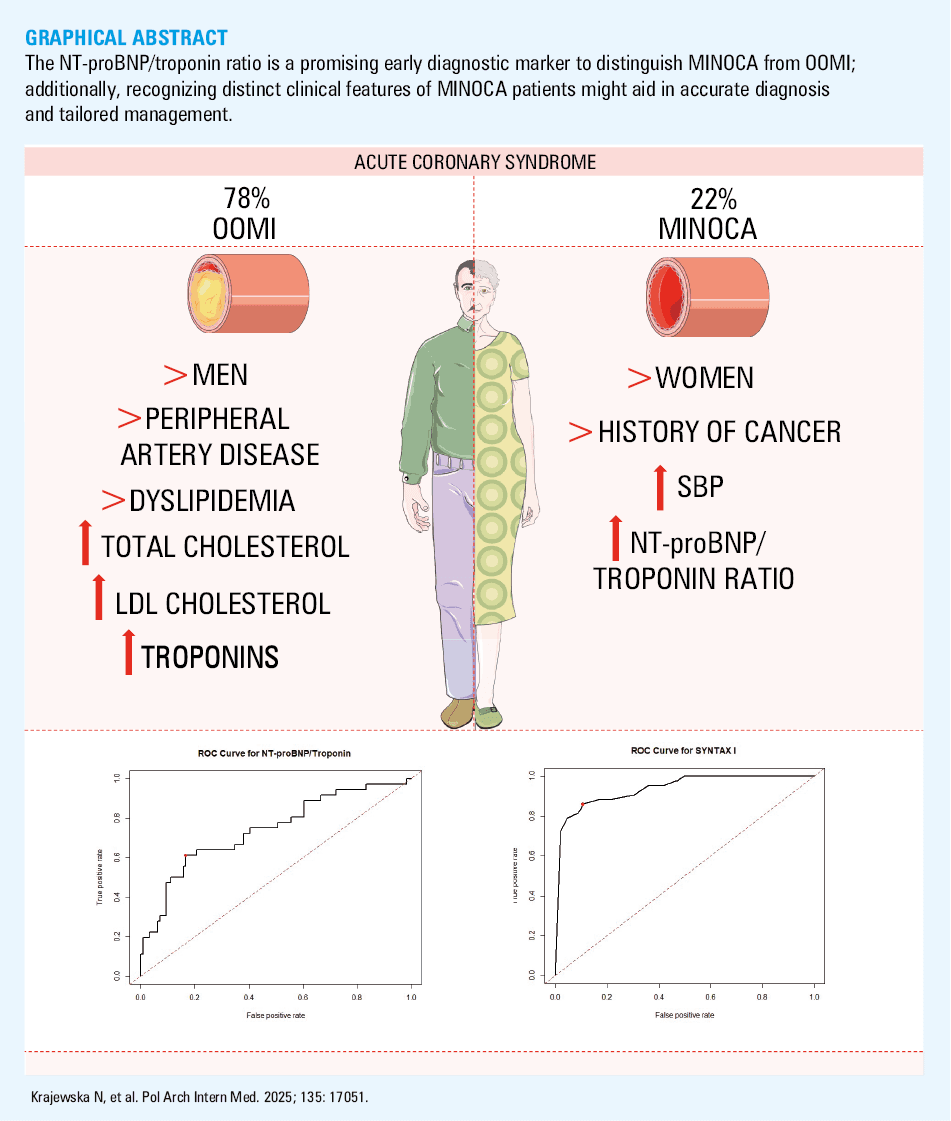
Results: Among the 194 patients, 43 (22%) were diagnosed with MINOCA. Men were more frequently diagnosed with OOMI than MINOCA (120 [79%] vs 24 [56%]; P = 0.003). A history of cancer was more common in the MINOCA than the OOMI group (23% vs 10%; P = 0.04), while peripheral artery disease and dyslipidemia were less prevalent in the patients with MINOCA (9% vs 97%; P <0.001 and 26% vs 49%; P = 0.01, respectively). MINOCA patients had higher systolic blood pressure (SBP) on admission (median [interquartile range, IQR], 154 [140–167] vs 140 [126–158] mm Hg); P <0.04), while patients with OOMI exhibited higher levels of total cholesterol, low‑density lipoprotein cholesterol, and troponin. The NT‑proBNP/troponin ratio was higher in the MINOCA patients than in the individuals with OOMI (median [IQR], 6.53 [1.28–17.25] vs 1.04 [0.15–3.65]; P <0.001). Furthermore, the ratio effectively distinguished MINOCA from OOMI, as reflected by an area under the curve value of 0.739. It was also a significant predictor of MINOCA (odds ratio, 1.153; 95% CI, 1.04–1.34; P = 0.02).
Conclusions: This study provides a comprehensive clinical profile of patients with MINOCA (female sex, a history of cancer, higher SBP), which may help support hypotheses for future prospective studies. The NT‑proBNP/troponin ratio emerges as a promising tool for early differentiation of MINOCA patients, warranting further research.
What's new?
This study presents a comprehensive clinical profile of individuals with myocardial infarction with nonobstructive coronary arteries (MINOCA). Potentially, the N‑terminal pro–B‑type natriuretic peptide to troponin ratio might serve as an early diagnostic tool to differentiate MINOCA from occlusion or obstructive myocardial infarction, leading to faster identification and adequate management of MINOCA. Identifying the at‑risk population through specific clinical characteristics—such as female sex, history of cancer, higher systolic blood pressure on admission, and lower low‑density lipoprotein and total cholesterol levels—could allow for closer monitoring, reduce misdiagnoses and overtreatment, and ultimately improve outcomes for MINOCA patients.
Introduction
Acute coronary syndrome (ACS) is usually caused by narrowing or occlusion of coronary vessels, referred to as obstructive or occlusion myocardial infarction (OOMI), which occurs due to plaque buildup or acute rupture with thrombus formation. However, there is a subgroup of patients who experience ACS without significant stenosis on invasive coronary angiography (ICA). This condition, known as myocardial infarction with nonobstructive coronary arteries (MINOCA), presents distinct diagnostic and therapeutic challenges for clinicians.
MINOCA is a relatively common condition, accounting for approximately 5% to 25% of all MI cases.1 A working diagnosis of MINOCA is established when coronary angiography shows less than 50% obstruction in the coronary arteries or no visible signs of atherosclerosis.2 Due to diverse underlying mechanisms of MINOCA, an accurate diagnosis and effective management can be challenging.
The most frequent causes of MINOCA involve issues in the epicardial coronary arteries, such as plaque rupture, spontaneous coronary artery dissection, epicardial vasospasm, or thrombosis, as well as coronary microvascular dysfunction (CMD), an imbalance between oxygen demand and supply, and other unknown mechanisms.3-5 Identifying the underlying treatable cause is essential for optimizing patient outcomes.6
Currently, there are no specific distinguishing features or risk factors that can reliably differentiate MINOCA patients from those with obstructive coronary artery disease (CAD) during the initial diagnostic phase. This highlights the need for comprehensive research focused on detailed clinical characteristics and the development of early diagnostic tools.
This study aimed to provide a comprehensive clinical profile of MINOCA by assessing its prevalence, outcomes, and associated risk factors. Additionally, we sought to explore the N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP)/troponin ratio as a potential novel early diagnostic tool for identifying MINOCA. The findings intend to lay the groundwork for future advancements in the diagnosis and treatment of MINOCA, ultimately improving patient care and outcomes.
Patients and methods
Study population and design
This single‑center, retrospective study evaluated all patients with ACS who were admitted to the First Department of Cardiology of the Medical University of Warsaw, Poland between January 2023 and June 2023 and underwent coronary angiography. The patients were classified into 2 groups—MINOCA and OOMI—based on the findings from ICA and optical coherence tomography (OCT) imaging. MINOCA was defined as MI with no angiographic evidence of obstructive CAD, but with an ischemic mechanism responsible for the myocardial injury (nonischemic causes, such as myocarditis or takotsubo syndrome, were excluded).
Comprehensive data, including demographic information, clinical characteristics on admission, laboratory test results, as well as OCT findings, were meticulously collected from the hospital’s medical records system.
Ethics
Due to the retrospective study design, the medical ethical committee at the Medical University of Warsaw deemed that informed consent and formal ethical approval were not required. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
N‑terminal pro–B‑type natriuretic peptide / troponin ratio
The NT‑proBNP/high‑sensitivity troponin I (hs‑TnI) ratio was calculated for every patient using the last measurements taken before ICA.
SYNTAX score
For patients with complete data available—including left main coronary artery disease status, sex, presence of chronic obstructive pulmonary disease (COPD), age, and left ventricular ejection fraction—SYNTAX scores I and II were calculated. The calculations were performed using the official SYNTAX score calculator available at https://syntaxscore.org.
Follow‑up end points
Major adverse cardiac events (MACEs) were defined as all‑cause mortality, nonfatal MI, stroke, cardiogenic shock, pulmonary embolism, and heart failure exacerbation. Additionally, we obtained information about rehospitalization, time to the first rehospitalization, and recurrent myocardial incidents (target lesion failure [TLF], target vessel failure [TVF], target vessel revascularization [TVR], target lesion revascularization [TLR]). The patients were followed for 6 months since the admission date or until death, based on hospital medical records.
Statistical analysis
Categorical variables are presented as absolute numbers with percentages and were compared using the χ2 test. If the expected size of any group was smaller than or equal to 5, the Fisher test was performed. Continuous variables are presented as mean (SD) for normally distributed data and median with interquartile range (IQR) for non‑normally distributed variables. If the variables were assumed to be normally distributed, the t test was performed; otherwise, the Mann–Whitney test was used for data comparison. Receiver operating characteristic (ROC) curve analysis was carried out to assess the diagnostic performance of the NT‑proBNP/hs‑TnI ratio. The area under the curve (AUC) was also calculated and optimal cutoff value was determined using the Youden index. Logistic regression analysis was performed to calculate odds ratios (ORs) with 95% CIs, assessing the connection between clinical variables (NT‑proBNP/troponin ratio, total cholesterol [TC], low‑density lipoprotein cholesterol [LDL‑C], systolic blood pressure [SBP], and troponins) and the likelihood of MINOCA. A 2‑tailed P value below 0.05 was deemed significant. All analyses were conducted in R package, version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline clinical characteristics
The study population comprised 194 patients, of whom 151 (78%) had OOMI and 43 (22%) had MINOCA. Men accounted for a higher proportion of the OOMI group than of the MINOCA group (120/151 (79%) vs 24/43 (56%); P = 0.003). However, sex distribution among the MINOCA patients was almost identical (men vs women, 24 [56%] vs 19 [44%]). There were no significant age differences between the groups. Prevalence of comorbidities was also similar, except for the history of cancer (OOMI vs MINOCA, 10% vs 23%; P = 0.04), peripheral artery disease (PAD; OOMI vs MINOCA, 97% vs 9%; P <0.001), and dyslipidemia (OOMI vs MINOCA, 49% vs 26%; P = 0.01; Table 1).
Parameter | OOMI (n = 151) | MINOCA (n = 43) | P value |
Data are presented as number (percentage) unless indicated otherwise.
Abbreviations: COPD, chronic obstructive pulmonary disease; OOMI, obstructive or occlusion myocardial infarction; MINOCA, myocardial infarction with nonobstructive coronary arteries | |||
Demographics | |||
Age | 66 (12) | 68 (11) | 0.54 |
Men | 120 (79) | 24 (56) | 0.003 |
Comorbidities | |||
Chronic coronary syndromes | 41 (27) | 14 (33) | 0.62 |
Arterial hypertension | 106 (70) | 35 (81) | 0.21 |
Chronic kidney disease | 19 (13) | 6 (14) | >0.99 |
Type 2 diabetes mellitus | 40 (26) | 17 (40) | 0.14 |
COPD | 7 (5) | 4 (10) | 0.42 |
Heart failure | 66 (44) | 21 (49) | 0.67 |
History of cancer | 15 (10) | 10 (23) | 0.04 |
Peripheral artery disease | 146 (97) | 4 (9) | <0.001 |
Dyslipidemia | 74 (49) | 11 (26) | 0.01 |
Atrial fibrillation | 21 (14) | 8 (19) | 0.60 |
Smoking | 83 (55) | 16 (37) | 0.06 |
Pack‑years, mean (SD) | 35 (19) | 41 (14) | 0.44 |
Alcoholism | 17 (11) | 3 (7) | 0.57 |
Clinical characteristics on admission
Heart rate (HR), diastolic blood pressure (DBP), ejection fraction (EF), oxygen saturation levels, New York Heart Association class, Canadian Cardiovascular Society score, and ST‑segment elevation MI (STEMI) frequency did not differ between the patients with obstructive CAD and those with MINOCA. However, SBP on admission was higher in the patients with MINOCA than those with OOMI (median [IQR], 154 [140–167] mm Hg vs 140 [126–158] mm Hg; P = 0.04). Additional data are presented in Supplementary material, Table S1.
Laboratory findings
The patients with OOMI had higher levels of TC, LDL‑C, and high‑sensitivity troponin I (hs‑TnI) than the individuals with MINOCA (median [IQR], 173 [136–221] mg/dl vs 147 [123–170] mg/dl; P = 0.02; 99 [76–137] mg/dl vs 67 [56–95] mg/dl; P = 0.003; and 0.834 [0.147–7.290] ng/ml vs 0.088 [0.019–1.285] ng/ml; P <0.001, respectively; reference ranges, TC <200 mgl/dl; LDL‑C <115 mg/dl; hs‑TnI <0.014 ng/ml). Other laboratory parameters, such as high‑density lipoprotein cholesterol, triglycerides, creatinine, estimated glomerular filtration rate, C‑reactive protein, glucose, NT‑proBNP, and glycated hemoglobin were comparable in both groups (Table 2). In the logistic regression analysis TC, LDL‑C, hs‑TnI, and SBP were not significant predictors of MINOCA.
Parameter | OOMIa | MINOCAa | P value |
Data are presented as mean (SD) or median (interquartile range).
a The number of patients varies per variable due to missing data in medical records.
SI conversion factors: to convert total cholesterol, HDL‑C, LDL‑C, and TG to mmol/l, multiply by 0.02586; creatinine to μmol/l, by 88.4; glucose to mmol/l, by 0.05551; CRP to nmol/l, by 9.524; NT‑proBNP to pmol/l, by 0.118.
Abbreviations: CRP, C‑reactive protein; eGFR, estimated glomerular filtration rate; HDL‑C, high‑density lipoprotein cholesterol; hs‑TnI, high‑sensitivity troponin I; LDL‑C, low‑density lipoprotein cholesterol; NT‑proBNP; N‑terminal pro–B‑type natriuretic peptide; TG, triglyceride; others, see Table 1 | |||
Total cholesterol, mg/dl | 173 (136–221) | 147 (123–170) | 0.02 |
HDL‑C, mg/dl | 44 (38–55) | 50 (39–62) | 0.16 |
LDL‑C, mg/dl | 99 (76–137) | 67 (56–95) | 0.003 |
TG, mg/dl | 115 (80–160) | 116 (79–135) | 0.34 |
Creatinine, mg/dl | 1.07(0.88–1.29) | 1.03 (0.87–1.27) | 0.47 |
eGFR, ml/min/1.73 m2 | 68 (24) | 67 (21) | 0.81 |
CRP, mg/l | 3.8 (1.4–11.3) | 4.6 (1.4–15.1) | 0.76 |
Glucose, mg/dl | 115 (101–139) | 105 (98–132) | 0.24 |
hs‑TnI, ng/ml | 0.834 (0.147–7.290) | 0.088 (0.019–1.285) | <0.001 |
NT‑proBNP, pg/ml | 549 (180–2797) | 611 (151–2562) | 0.77 |
N‑terminal pro–B‑type natriuretic peptide / troponin ratio
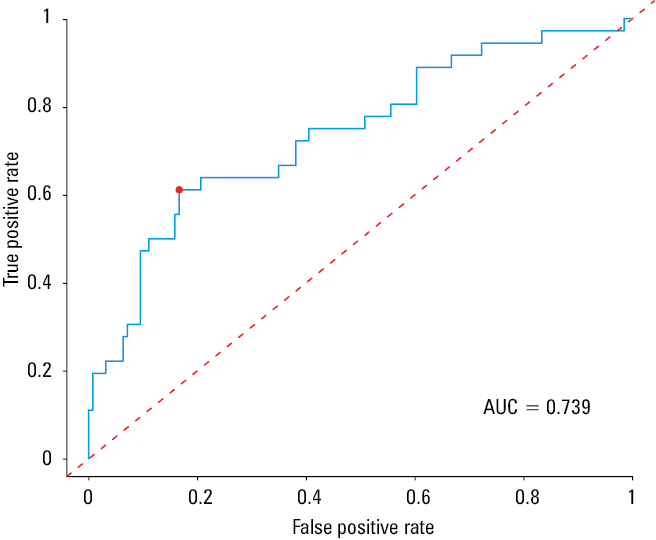
The NT‑proBNP/hs‑TnI ratio was markedly higher in the MINOCA patients than in those with OOMI (median [IQR], 6.53 [1.28–17.25] vs 1.04 [0.15–3.65]; P <0.001; Table 3). ROC analysis demonstrated good discriminatory ability of the NT‑proBNP/hs‑TnI ratio with an AUC of 0.739. The optimal threshold of 5.56 yielded sensitivity of 61% (Figure 1). The NT‑proBNP/troponin ratio was positively associated with MINOCA in the logistic regression analysis (OR, 1.15; 95% CI, 1.04–1.34; P = 0.02; Table 4).
Parameter | OOMI (n = 126) | MINOCA (n = 35) | P value |
Data are presented as median (interquartile range).
SI conversion factors: see Table 2; NT‑proBNP/hs‑TnI ratio in SI units is calculated as (NT‑proBNP [ng/l] × 118) / hs‑TnI [ng/ml].
| |||
NT‑proBNP/hs‑TnI ratio | 1.04 (0.15–3.65) | 6.53 (1.28–17.25) | <0.001 |
Abbreviations: AUC, area under the curve
Variable (n = 129)a | OR (95% CI) | P value |
a The final number of patients included in the analysis was reduced due to missing data in the medical records.
| ||
SYNTAX score I, points | 0.336 (0.141–0.552) | <0.001 |
Total cholesterol, mg/dl | 1.008 (0.920–1.100) | 0.86 |
LDL‑C, mg/dl | 0.965 (0.856–1.080) | 0.53 |
NT‑proBNP/troponin ratio | 1.153 (1.040–1.340) | 0.02 |
SBP | 1.028 (0.990–1.080) | 0.23 |
hs‑TnI, ng/l | 1.000 (1.000–1.000) | 0.41 |
SYNTAX score
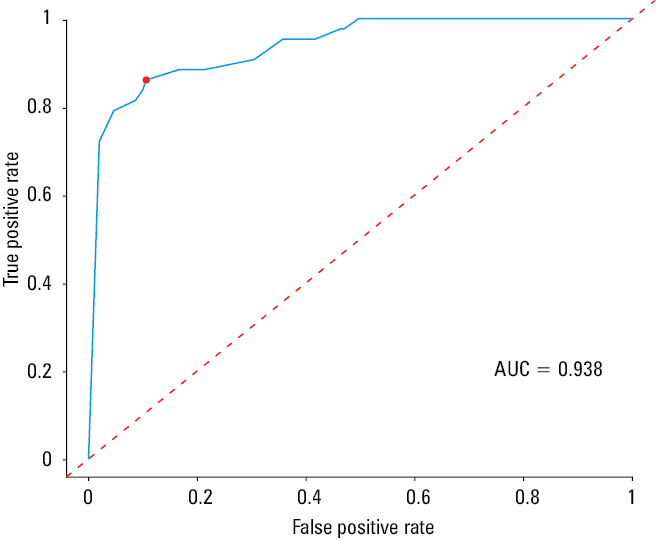
The SYNTAX score I was significantly higher in the patients with OOMI, as compared with those with MINOCA. The average SYNTAX score I for OOMI was 15, while for MINOCA, it was 1.7 (P <0.001). ROC analysis demonstrated very good discriminatory ability of the SYNTAX score I (AUC = 0.938). An optimal threshold of 4.75 yielded sensitivity of 86% (Figure 2). The SYNTAX score I was inversely related to the likelihood of MINOCA (OR, 0.34; 95% CI, 0.141–0.552; P = 0.001). However, no significant differences were found between the 2 groups regarding the percutaneous coronary intervention (PCI) SYNTAX score II, PCI 4‑year mortality, coronary artery bypass grafting (CABG) SYNTAX score II, or CABG 4‑year mortality (Table 5).
Abbreviations: see Figure 1
Parameter | OOMI | MINOCA | P value |
Data are presented as mean (SD) or median (interquartile range).
a Group size: OOMI, n = 151; MINOCA, n = 43
b Group size: OOMI, n = 122; MINOCA, n = 31
Abbreviations: CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention; others, see Table 1 | |||
SYNTAX score Ia, points | 13.5 (7–21.5) | 0 (0–2) | <0.001 |
PCI SYNTAX score IIb, points | 32 (24–44) | 32 (21–39) | 0.26 |
PCI 4‑year predicted mortalityb, % | 8.3 (4–19.9) | 8.5 (3.3–14.2) | 0.43 |
CABG SYNTAX Score IIb | 29 (12) | 27 (10) | 0.48 |
CABG 4‑year predicted mortalityb, % | 6.4 (2.9–13.6) | 5.9 (3.4–9.5) | 0.41 |
Follow‑up
There were no significant differences in the incidence of rehospitalization, TLF, TVF, TVR, TLR, MACEs, and death in 6‑month follow‑up between the patients with OOMI and MINOCA. Additional data are presented in Supplementary material, Table S2.
Discussion
This study offers a comprehensive clinical profile of MINOCA patients, showing that they are more likely to be female, have a history of cancer, and present with higher SBP on admission. As compared with the OOMI cohort, MINOCA patients were less likely to have traditional cardiovascular risk factors, such as dyslipidemia and PAD, as indicated by their lower TC and LDL‑C levels. The NT‑proBNP/troponin ratio shows potential as a tool for early differentiation of MINOCA from obstructive CAD. Based on our findings, NT‑proBNP/troponin ratio cutoff value of 5.56 could serve as a clinical threshold aiding in the diagnosis of MINOCA.
MINOCA has a significant impact on daily clinical practice, accounting for 22% of all ACS cases in our study. This prevalence is higher than commonly reported in the literature, although some studies have documented rates as high as 25%.6-10 Variations in inclusion criteria (eg, all MI cases vs only STEMI or non‑STEMI), evolving diagnostic criteria for MINOCA, increasing use of high‑sensitivity assays, and variability in the interpretation of ICA could contribute to these inconsistencies in prevalence.3,10,11
We observed a higher representation of women among the patients with MINOCA, which aligns with previous studies.6-9,12,13 Our findings are almost identical to those reported in the systematic review by Pasupathy et al,6 where women made up 43% of the MINOCA population, but only 24% of the obstructive CAD population. In our study, these rates were 44% and 20%, respectively. However, unlike other studies,6,7,12 we did not observe an association between younger age and MINOCA.
Traditional cardiovascular risk factors, such as dyslipidemia, have been less commonly reported in patients with MINOCA, which is in line with our study.6,14 We also found that PAD was less prevalent in the MINOCA population; this risk factor was not frequently mentioned in other studies. The prevalence of other cardiovascular risk factors, including diabetes, hypertension, and smoking, is not consistent.6-10,14 We reported no significant differences between the groups regarding these risk factors. Notably, we observed an association between the history of malignancy and MINOCA, whereby cancer might predispose individuals to MINOCA.14,15 There are several factors that might be responsible for this dependency. Cancer is related to the release of inflammatory and angiogenic cytokines that might trigger epicardial or microvascular spasm,16 which is one of the mechanisms of MINOCA. Unobstructive CAD might also be a complication of cancer treatment, either chemo- or radiotherapy. Both of these treatments damage the endothelium, making coronary vasospasm and endothelial dysfunction more likely.17,18 These findings suggest that MINOCA might more often have an inflammation‑driven, rather than atherosclerosis‑driven pathophysiology.
The NT‑proBNP/troponin ratio has been proposed as an early, noninvasive, novel biomarker to differentiate entities of myocardial injury. It has been helpful in identifying possible takotsubo cardiomyopathy (TC) in patients presenting with ACS.19 A similar hypothesis was tested in a study by Budnik et al,20 where NT‑proBNP/TnI, NT‑proBNP/creatine kinase myocardial band mass, and NT‑proBNP/EF ratio were used to distinguish between TC and STEMI. The most accurate marker for early TC detection was the NT‑proBNP/troponin ratio.20 Furthermore, the NT‑proBNP/troponin ratio proved to be useful in differentiating between MI types 1 and 2 at an early diagnostic stage, despite both conditions presenting similarly.21 Our study investigated the utility of the NT‑proBNP/troponin ratio in predicting MINOCA in patients presenting with ACS. The results indicated that the NT‑proBNP/troponin ratio was significantly higher in the MINOCA patients than in those with obstructive CAD. Both MINOCA and OOMI are associated with elevated troponin concentration. However, in patients with OOMI, the levels of this biomarker are significantly higher, likely due to a higher prevalence of STEMI in this group. STEMI relates to larger infarct areas, leading to more substantial elevations in cardiac markers. Hjort et al22 reported a similar NT‑proBNP concentration in both groups, suggesting that the discrepancy in the NT‑proBNP/troponin ratio was primarily driven by differences in troponin levels. These findings are in accordance with our results. Additionally, we observed a good discriminatory ability of the NT‑proBNP/troponin ratio for differentiating between MINOCA and OOMI, and identified it as a significant predictor of MINOCA. We propose a NT‑proBNP/troponin ratio cutoff value of 5.56 as a potential threshold for differentiating between both conditions. This might further support the utility of the NT‑proBNP/troponin ratio in MINOCA differentiation.
As expected, the SYNTAX score I was significantly lower in the MINOCA patients, as compared with the OOMI population. We also demonstrated that SYNTAX score I was inversely related to the likelihood of MINOCA, and had 86% sensitivity for excluding a MINOCA diagnosis. These outcomes are inherent to the scoring system, which allocates points based on the number and severity of obstructed segments in the coronary tree, resulting in higher scores for patients with obstructive disease.
Data on the prognosis of patients with MINOCA remain contradictory. The discrepancies might stem from differences in the populations studied as well as diverse underlying mechanisms of MINOCA.3,11 In our study, there was no difference in outcomes between the MINOCA and OOMI groups. However, our follow‑up period was only 6 months, which might have been insufficient to portray true long‑term outcomes.
Limitations
The retrospective design of this study introduces limitations related to data availability and accuracy. Due to the fact that it was conducted at a single center, the findings reflect a single patient population and may be influenced by center‑specific practices and protocols. Furthermore, we only included patients who underwent coronary angiography, which excludes potential MINOCA cases where this procedure was not performed. Another limitation of our study is the low number of available OCT images, as they were performed in only 5 patients. Additionally, we excluded individuals with final hospital diagnosis of takotsubo syndrome or myocarditis; however we did not collect information on further diagnostic testing, such as cardiac magnetic resonance imaging (MRI). Since MRI is recognized as a valuable tool in differentiating MINOCA, there is a possibility of misdiagnoses in some cases.
The timing of cardiac biomarker measurements and coronary angiography may have varied across patients due to the retrospective nature of the study, introducing variability. Additionally, the 6‑month follow‑up period limits the assessment of long‑term outcomes, and follow‑up data were confined to records from a single hospital, without access to external medical history.
Conclusions
Our study presents a detailed clinical profile of MINOCA patients. Compared with individuals with OOMI, MINOCA patients are more likely to be female, have a history of cancer, and present with elevated SBP on admission. In contrast, traditional cardiovascular risk factors, such as dyslipidemia, PAD, and elevated LDL‑C and TC levels, were more commonly associated with OOMI. The NT‑proBNP/troponin ratio emerged as a promising tool for early differentiation of MINOCA, with a proposed cutoff value of 5.56. However, prospective studies with larger sample sizes are needed to validate these findings, as well as to focus on the diagnostic approaches and long‑term outcomes of MINOCA to improve patient care.
- Niccoli G, Scalone G, Crea F. Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management. Eur Heart J. 2015; 36: 475‑481. | Crossref
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018; 138: e618‑e651. | Crossref
- Tamis‑Holland JE, Jneid H, Reynolds HR, et al. Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the American Heart Association. Circulation. 2019; 139: e891‑e908. | Crossref
- Khan A, Lahmar A, Riasat M, et al. Myocardial infarction with non‑obstructive coronary arteries: an updated overview of pathophysiology, diagnosis, and management. Cureus. 2022; 14: e23602. | Crossref
- Lindahl B, Baron T, Albertucci M, Prati F. Myocardial infarction with non‑obstructive coronary artery disease. EuroIntervention. 2021; 17: e875‑e887. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION