Rare immune adverse event in the treatment of non–small-cell lung carcinoma: durvalumab-associated optic neuritis

 CC BY 4.0
CC BY 4.0
Rare immune adverse event in the treatment of non–small-cell lung carcinoma: durvalumab-associated optic neuritis
A 69‑year‑old man was admitted to a clinical oncology clinic in December 2022 due to persistent cough unresponsive to antibiotics. Imaging studies showed a right hilar mass, and subsequent biopsy confirmed a diagnosis of non–small‑cell lung cancer (squamous cell carcinoma), stage cT4N2M0. The patient received definitive chemoradiotherapy at a dose of 66 Gy in 33 fractions, concurrent with 2 cycles of cisplatin‑vinorelbine. After confirming no apparent progression on imaging, the patient was found eligible for consolidation immunotherapy with durvalumab, a programmed death ligand 1–blocking antibody, starting in April 2023.1
After 5 courses of immunotherapy, in June 2023, the patient reported decreased visual acuity (VA) in his left eye that lasted for approximately 1 month. Comprehensive examination at a regional ophthalmology department included head and orbital computed tomography and magnetic resonance imaging (MRI), cervical Doppler ultrasonography, a visual field test, and optical coherence tomography (Figure 1A). Metastasis, hemorrhage, and ischemia were ruled out. VA of the left eye was 0.1, and fundoscopy showed left optic disc edema. Immunotherapy‑related optic neuritis (ON) was diagnosed.
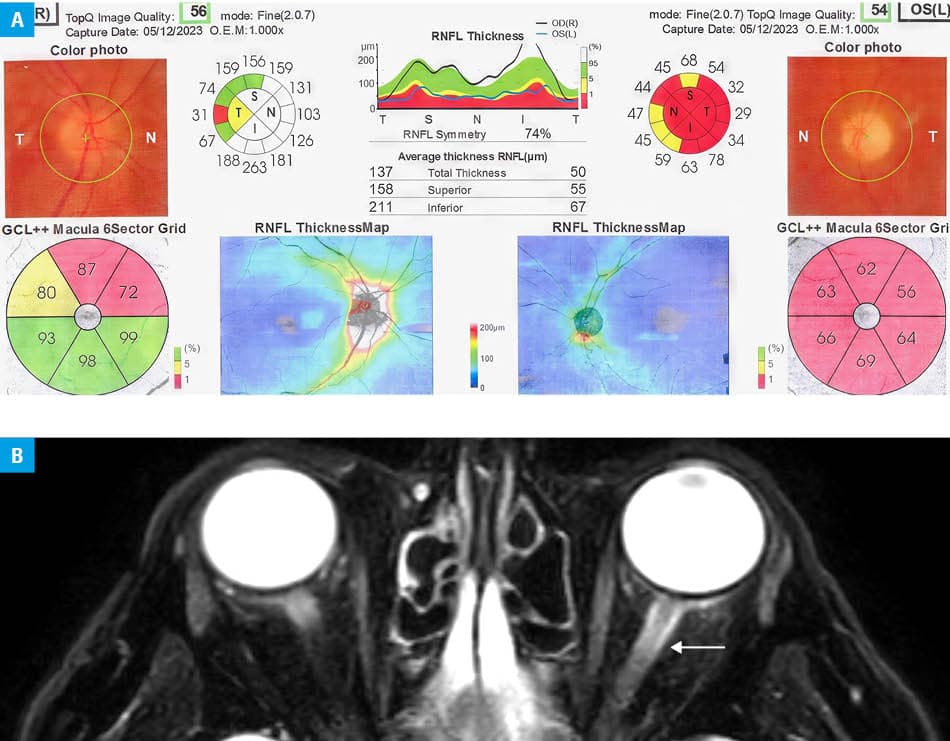
Abbreviations: GCL, ganglion cell layer; RNFL, retinal nerve fiber layer
Treatment with methylprednisolone was implemented at an initial dose of 8 mg daily, reduced to 4 mg after a week, then to 2 mg, and eventually discontinued. At a follow‑up ophthalmologic examination, a reduction of optic disc swelling was observed, but VA improved only to 0.3, presumably due to the long interval between symptom onset and treatment initiation. Five months later, the patient’s vision deteriorated again (VA in the left eye, 0.1). No abnormalities were found on fundoscopy, but minor edematous lesions in the left optic nerve were found on orbital MRI (Figure 1B). Three months later, the patient developed superior vena cava (SVC) syndrome secondary to tumor infiltration into the mediastinum, and underwent SVC stent placement. Despite subsequent lines of chemotherapy (carboplatin / vinorelbine, carboplatin / gemcitabine, and finally docetaxel), the disease continued to progress. He received his last cycle of docetaxel in June 2024, and was followed until his death in March 2025. Up to his last imaging study, the disease had remained limited to the thorax; only then was a solitary intrahepatic lesion identified.
Checkpoint inhibitors are used in the treatment of various malignancies, including melanoma, lung, or bladder cancers. Neuro‑ophthalmologic toxicities are rare, reported only in 0.46% of treated patients.2,3 Most cases of ON occur during treatment with ipilimumab, isolated cases have been reported with pembrolizumab, nivolumab, and atezolizumab. To our knowledge, only a single case of durvalumab‑associated ON has been reported in the literature.2 The mechanism behind these neuro‑ophthalmic complications is not yet explored, with overstimulation of immune responses being the most likely cause.
The leading symptom of ON is unilateral or bilateral loss of visual and / or color acuity. Ophthalmoscopy may demonstrate optic disc swelling, and MRI often shows an increased signal in the affected optic nerve. Comprehensive neurology and ophthalmology evaluation is mandatory to exclude more common etiologies, such as demyelinating disease, ischemia, or thromboembolism. The treatment of ON involves high‑dose corticosteroids, first given intravenously, followed by an oral taper.4,5 In most cases, normal VA is regained within 2 months; however, as observed in our case, delayed diagnosis and treatment might lead to a permanent deficit. Clinicians should be cautious of ocular symptoms reported by patients undergoing immunotherapy and refer them for neuro‑ophthalmologic examination when such symptoms arise.
- Spigel DR, Faivre‑Finn C, Gray JE, et al. Five‑year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in stage III non‑small‑cell lung cancer. J Clin Oncol. 2022; 40: 1301‑1311. | Crossref
- Yu CW, Yau M, Mezey N, et al. Neuro‑ophthalmic complications of immune checkpoint inhibitors: a systematic review. Eye Brain. 2020; 12: 139‑167. | Crossref
- Pietris J, Santhosh S, Ferdinando Cirocco G, et al. Immune checkpoint inhibitors and optic neuropathy: a systematic review. Semin Ophthalmol. 2023; 38: 547‑558. | Crossref
- Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune‑related adverse events in patients treated with immune checkpoint inhibitor therapy: asco guideline update. J Clin Oncol. 2021; 39: 4073‑4126. | Crossref
- Wilhelm H, Schabet M. The diagnosis and treatment of optic neuritis. Dtsch Ärztebl Int. 2015; 112: 616‑626. | Crossref
ARTICLE INFORMATION