Benefits from statins in anticoagulated venous thromboembolism patients: recent advances
Key words: oral anticoagulation, pleiotropic effect, secondary prevention, statins, venous thromboembolism



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Benefits from statins in anticoagulated venous thromboembolism patients: recent advances
Venous thromboembolism (VTE), encompassing deep vein thrombosis and pulmonary embolism, remains a major cause of morbidity and mortality worldwide. Although oral anticoagulation is the cornerstone of VTE treatment, recurrent events and long‑term complications, such as post‑thrombotic syndrome, persist in a significant proportion of patients. Recent evidence suggests that statins, traditionally used for lipid‑lowering therapy, may exert pleiotropic beneficial effects in patients with VTE, particularly those already receiving anticoagulants. These benefits include anti‑inflammatory, antithrombotic (eg, anticoagulant, antiplatelet, and profibrinolytic actions), endothelial‑stabilizing, and immunomodulatory properties. Clinical and observational studies have highlighted that statin use is associated with reduced risk of recurrent VTE and improved survival, even in the absence of hyperlipidemia.
This review synthesizes the current evidence on the role of statins in anticoagulated patients with VTE, exploring mechanistic insights, clinical trial data, and real‑world findings. We also discuss the potential synergistic effects between statins and anticoagulants, as well as safety considerations, particularly in elderly and polymedicated populations. Furthermore, we address the limitations of existing studies and outline future research directions to establish whether statins should be systematically considered in secondary prevention strategies for VTE.
In conclusion, statins appear to confer significant adjunctive benefits in anticoagulated VTE patients, with an acceptable safety profile. Integration of statins into VTE management may represent a cost‑effective and widely accessible intervention to enhance patient outcomes, though prospective randomized controlled trials are still needed to confirm causality and determine the optimal use.
Introduction
Venous thromboembolism (VTE), encompassing both deep vein thrombosis (DVT) and pulmonary embolism (PE), is a major contributor to global cardiovascular morbidity and mortality, with an incidence of 1–2 cases per 1000 individuals per year in Western populations.1,2 Despite standard treatment with anticoagulation—traditionally with vitamin K antagonists and more recently with direct oral anticoagulants (DOACs)—a substantial risk of recurrence and long‑term complications persists.3-5 These complications include post‑thrombotic syndrome, recurrent PE, and chronic thromboembolic pulmonary hypertension, all of which significantly impair quality of life and long‑term prognosis.6,7
Statins, widely prescribed for their lipid‑lowering properties in the prevention of atherosclerotic cardiovascular disease, have also demonstrated pleiotropic effects. These include anti‑inflammatory, antithrombotic, immunomodulatory, and endothelial‑stabilizing actions that may be highly relevant in the pathophysiology of VTE.8-10 Among their antithrombotic properties, statins exert anticoagulant effects (eg, reduced tissue factor expression, upregulation of the protein C pathway), antiplatelet actions, and profibrinolytic effects, such as improved fibrin clot structure and enhanced fibrinolysis through suppression of plasminogen activator inhibitor‑1 (PAI‑1) levels.11-14 Recent mechanistic insights have suggested that statins may exert anticoagulant effects beyond lipid lowering, including modulation of fibrin clot structure, such as increased clot permeability and reduced density, and enhanced fibrinolysis, as detailed in recent reviews.10,11
Evidence suggests that inflammation, endothelial dysfunction, and disordered coagulation are key contributors to thrombogenesis and recurrence, making these pleiotropic actions of statins particularly promising in VTE management.14,15 A growing body of observational and real‑world evidence supports the potential benefit of statin use in VTE patients. In several cohort studies and post hoc analyses of randomized trials, statin therapy has been associated with a reduced risk of VTE recurrence and improved survival, even in patients without traditional lipid indications.16-18 These findings have prompted growing interest in repurposing statins as adjunctive therapy in anticoagulated VTE patients.
The aim of this review is to synthesize the most recent advances in the understanding of statin use in patients with VTE who are already receiving anticoagulation therapy. We explore mechanistic pathways, clinical data, observational studies, and ongoing research, and highlight both the therapeutic potential and limitations of this approach, in order to provide insight into whether statins could become a standard component of secondary VTE prevention.
Biological rationale for statin use in venous thromboembolism
The potential benefit of statins in anticoagulated VTE patients stems from their ability to influence multiple biological pathways involved in thrombogenesis. Statins inhibit 3‑hydroxy‑3‑methyl‑glutaryl‑coenzyme A reductase, reducing the synthesis of mevalonate and its downstream isoprenoids. This inhibition affects intracellular signaling pathways that modulate inflammation, immune function, and coagulation.19,20
In patients with coronary artery disease treated with high‑dose statins (rosuvastatin 40 mg/d or atorvastatin 80 mg/d), Stępień et al21 reported significant reductions in coagulation factors (Fs) FVII, FVIII, and FXI. Notably, FXI reduction strongly correlated with LDL‑C lowering (β = 0.58; P <0.001). Similar findings were yielded by a study on rosuvastatin 20 mg/d from the Netherlands.22
A key feature of statins is their anti‑inflammatory activity, as evidenced by reductions in circulating inflammatory biomarkers, such as C‑reactive protein (CRP), interleukin‑6 (IL‑6), and tumor necrosis factor α (TNF-α)—mediators known to contribute to the initiation and progression of VTE.23-25 In addition, statins improve endothelial function by enhancing nitric oxide (NO) bioavailability, reducing oxidative stress, and attenuating leukocyte–endothelium interactions. These actions help preserve endothelial barrier integrity, often impaired in patients with VTE. Endothelial injury is a critical component of Virchow’s triad, alongside venous stasis and hypercoagulability, and plays a central role in thrombogenesis.
Statins also demonstrate important anticoagulant properties. They downregulate tissue factor expression, upregulate thrombomodulin and the protein C system, and suppress thrombin generation, even in the presence of anticoagulation therapy. Moreover, they attenuate platelet activation through reduced thromboxane A2 production and inhibition of integrin signaling, while also promoting fibrinolysis by decreasing PAI‑1 levels and improving fibrin clot structure and lysability.26-28
Recent studies have further suggested that statins may reduce markers of neutrophil extracellular traps (NETs), which contribute to immunothrombosis and play a pivotal role in VTE pathophysiology. Moreover, Stępień et al21 reported that high‑dose statins significantly reduce the levels of NET‑related proteins, further supporting their antithrombotic role.
These findings offer additional mechanistic support for the antithrombotic effects of statins.29-31
Together, these pleiotropic mechanisms, anti‑inflammatory, anticoagulant, antiplatelet, and profibrinolytic, highlight a strong biological rationale for the use of statins as adjunctive agents in patients with VTE, particularly those on long‑term anticoagulation. An overview of these effects is presented in Figure 1 and Table 1.
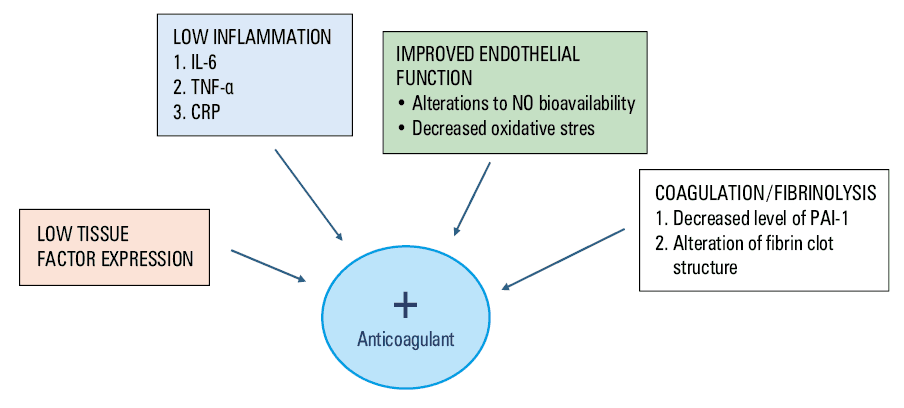
Abbreviations: CRP, C‑reactive protein; IL‑6, interleukin‑6; NO, nitric oxide; PAI‑1, plasminogen activator inhibitor‑1; TNF-α, tumor necrosis factor α
Mechanism | Effect | Clinical relevance in VTE |
Abbreviations: ↑, increase; ↓, decrease; F, factor; LDL‑C, low‑density lipoprotein cholesterol; NET, neutrophil extracellular trap; VTE, venous thromboembolism; others, see Figure 1 | ||
Anti‑inflammatory | ↓ CRP, IL‑6, TNF-α | Attenuates inflammation‑driven thrombus formation |
Endothelial function improvement | ↑ NO bioavailability, ↓ oxidative stress | Stabilizes endothelium and reduces leukocyte adhesion |
Anticoagulant activity | ↓ Tissue factor expression, ↑ thrombomodulin, ↑ protein C pathway | Reduces thrombin generation |
Antiplatelet activity | ↓ Platelet activation, ↓ thromboxane A2, inhibition of integrin signaling | Limits platelet aggregation and microthrombi formation |
Profibrinolytic effect | ↓ PAI‑1, ↑ fibrinolysis, improved clot permeability and lysis | Promotes clot resolution, lowers recurrence risk |
NET inhibition | ↓ NET formation | Reduces immunothrombosis, particularly in cancer‑associated VTE |
Lipid‑lowering dependent effects | ↓ LDL‑C linked to ↓ FXI, ↓ fibrinogen, improved clot architecture | Supports both cholesterol‑mediated and independent antithrombotic effects |
Clinical evidence on statin use in venous thromboembolism
Over the past 2 decades, a growing body of clinical and observational evidence has emerged suggesting that statin use is associated with a reduced risk of VTE, including both primary events and recurrences, even in patients receiving anticoagulation therapy. This section summarizes the most relevant clinical studies on statins in the VTE setting.
Several observational studies have identified a protective association between statin therapy and VTE incidence. In the RIETE registry, patients receiving statins at baseline exhibited significantly lower all‑cause mortality, reduced recurrence rates, and improved overall prognosis, regardless of the anticoagulant used.
Although heterogeneity between studies exists, consistency of the association across diverse populations and settings strengthens the argument for a potential protective effect of statins.
Randomized controlled trials (RCTs), although not specifically designed to evaluate VTE outcomes, have provided supportive data as well. The JUPITER trial (Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin), which assessed the efficacy of rosuvastatin in primary prevention, reported a significant 43% reduction in the risk of symptomatic VTE as compared with placebo.32 In HOPE‑3 (Heart Outcomes Prevention Evaluation‑3) trial, rosuvastatin use was associated with a modest but significant reduction in thromboembolic complications.33 Although VTE was not a primary end point in these trials, the magnitude and consistency of the observed benefits warrant further investigation through dedicated randomized studies.
Despite these promising findings, it is important to acknowledge that most of the available evidence derives from observational analyses and post hoc data. Thus, residual confounding cannot be entirely excluded. However, the consistent observation of benefit across studies, particularly in patients already on anticoagulants, supports further exploration of statins as a complementary strategy in the management of VTE.
Statins and anticoagulants: synergistic or redundant?
The concurrent use of statins and anticoagulants in patients with VTE raises a critical clinical question: do statins provide additive or synergistic benefit beyond that conferred by anticoagulation alone, or are their effects redundant? Emerging mechanistic and clinical evidence strongly supports a synergistic interaction, as these drug classes act on distinct but complementary biological pathways involved in thrombogenesis and inflammation.
While DOACs and vitamin K antagonists target specific components of the coagulation cascade, statins exert upstream effects, modulating endothelial function, systemic inflammation, platelet activation, and thrombin generation.34-36 For example, statins have been shown to downregulate tissue factor expression, upregulate thrombomodulin, enhance the protein C anticoagulant pathway, and promote fibrinolysis through favorable modulation of PAI‑1 levels and fibrin clot structure.10,23,25 These anticoagulant and profibrinolytic effects are increasingly recognized as central to the antithrombotic profile of statins and warrant more emphasis in VTE‑related research.
Experimental studies have confirmed that statins reduce thrombin generation and inflammatory activation even in the presence of concurrent anticoagulation, indicating their nonredundant and possibly additive role. In clinical settings, anticoagulated patients receiving statins have demonstrated lower levels of D‑dimer, CRP, and fibrinogen, biomarkers associated with residual thrombotic risk and systemic inflammation, than those receiving anticoagulants alone.37
Pharmacokinetic considerations are also important when combining these therapies. Hydrophilic statins, such as rosuvastatin and pravastatin, are minimally metabolized by cytochrome P450 enzymes, making them less likely to interact with DOACs. In contrast, lipophilic statins, such as simvastatin and atorvastatin, are substrates of cytochrome P450 3A4 (CYP3A4), the same enzyme that metabolizes rivaroxaban and apixaban. Although this theoretically increases the risk of drug‑drug interactions and bleeding, clinical data have not consistently shown higher rates of adverse events in patients taking both agents.38
In summary, current data support a synergistic model in which statins and anticoagulants act via complementary pathways to reduce thrombotic risk in VTE patients. Their combination appears to be both effective and safe, particularly when pharmacologic interactions are considered and monitored appropriately. Future randomized studies should assess whether specific combinations of statin types and anticoagulants offer enhanced protection and better long‑term outcomes.
Subgroup analyses and special populations
The benefits of statins in anticoagulated VTE patients may not be uniformly distributed across all subgroups. Emerging data suggest that elderly individuals, patients with multiple comorbidities, and those with cancer‑associated thrombosis (CAT) may experience particularly favorable outcomes with adjunctive statin use. These populations often exhibit heightened thromboinflammatory activity and endothelial dysfunction, which may increase their responsiveness to the pleiotropic effects of statins.
In older adults, endothelial senescence, oxidative stress, and chronic low‑grade inflammation are prevalent and contribute to thrombotic risk. Statins, by enhancing nitric oxide bioavailability, reducing vascular inflammation, and improving endothelial stability, may counteract these mechanisms. Studies reported that statin users aged 75 years and older had lower mortality and reduced VTE recurrence as compared with nonusers, independent of lipid levels or cardiovascular comorbidities.39,40
Patients with metabolic comorbidities, such as diabetes mellitus, hypertension, and chronic kidney disease, also appear to benefit from statin therapy. These conditions are often associated with increased PAI‑1 levels, impaired fibrinolysis, and abnormal clot structure. Statins may favorably modify these hemostatic abnormalities, in part through reduction in low‑density lipoprotein cholesterol (LDL‑C), which has recently been linked to lower circulating levels of coagulation factors including FXI, and improved clot lysis.40-47 Furthermore, a growing body of literature demonstrates that lower LDL‑C levels correlate with improved fibrin clot permeability and susceptibility to lysis, that is, key factors in preventing recurrent thrombosis.12,24
Cancer patients represent another high‑risk group. The prothrombotic nature of malignancy, driven by tumor‑derived tissue factor, cytokines, and NETs, renders them susceptible to both VTE and poor outcomes. Preliminary studies suggest that statins may reduce NET formation, as shown in recent publications in 2024, and may improve survival and reduce recurrent thrombosis in CAT populations.
In summary, while statins may provide global antithrombotic benefit in anticoagulated VTE patients, the magnitude of effect appears greatest in certain subgroups. These include the elderly, patients with multimorbidity, and those with malignancy. Further research is warranted to determine whether targeted statin therapy based on individual risk profiles and biomarkers (eg, CRP, IL‑6, NETs) could optimize outcomes in these populations.
Safety and tolerability
The safety profile of statins is generally favorable, and the incidence of serious adverse events is relatively low, even when statins are used in combination with oral anticoagulants. The most commonly reported adverse effects include myalgia, transient hepatic enzyme elevations, and, rarely, rhabdomyolysis. These effects are typically dose‑dependent and more frequent with the lipophilic statins, such as simvastatin or atorvastatin, than the hydrophilic agents, such as rosuvastatin and pravastatin. Meta‑analyses and observational data have reported no compelling evidence for increased intracranial hemorrhage among statin users, although continued surveillance is warranted.
Concerns regarding the potential for increased bleeding when statins are co‑administered with anticoagulants have been addressed in several observational studies. A large retrospective cohort analysis involving over 25 000 anticoagulated patients demonstrated no significant increase in major bleeding among statin users, as compared to nonusers.
Recent mechanistic insights have suggested that statins may exert anticoagulant effects, including downregulation of tissue factor expression, enhancement of the protein C anticoagulant pathway, and favorable modulation of fibrin clot structure, as well as reduction in PAI‑1 levels. These effects may counterbalance any theoretical probleeding risk posed by pharmacokinetic interactions.
Drug‑drug interactions between statins and anticoagulants, especially DOACs, are generally manageable. Statins metabolized via CYP3A4, such as atorvastatin and simvastatin, may theoretically increase DOAC levels, but clinical relevance appears minimal in most cases. Rosuvastatin and pravastatin, with limited hepatic metabolism, are preferred choices when interaction risk is a concern.
From a practical perspective, statins are widely prescribed in elderly and polymedicated patients, enhancing their feasibility for broader use in VTE management. Their favorable safety profile, once‑daily dosing, low cost, and additional cardiovascular benefits support their potential as adjunctive therapy. However, careful monitoring remains warranted, particularly in individuals with hepatic dysfunction, statin intolerance, or those taking multiple interacting medications.
Limitations of current evidence
Despite encouraging findings from observational studies, registries, and secondary analyses of randomized trials, the evidence supporting statin use in anticoagulated VTE patients is not without significant limitations. The vast majority of available data originate from retrospective cohort studies or post hoc subgroup analyses, which inherently carry risks of selection bias, residual confounding, and misclassification. Although many of these studies adjust for known variables, unmeasured confounders, such as indication bias, baseline inflammatory status, and socioeconomic factors, may still affect outcomes and preclude definitive conclusions.
Another limitation lies in the heterogeneity of the patient populations and study designs, which complicates the interpretation and generalizability of results. Differences in age, comorbidities, duration of anticoagulation, type and dosage of statin used, and presence of concurrent cardiovascular disease are often inadequately stratified, making direct comparisons challenging. Moreover, few studies differentiate between lipophilic and hydrophilic statins, which may have distinct pharmacologic profiles relevant to thrombosis prevention.
Importantly, dedicated prospective RCTs assessing the effect of statins on VTE recurrence in patients on anticoagulation are lacking.
Furthermore, several mechanistic insights remain underexplored in clinical settings, including the impact of LDL‑C reduction on coagulation markers (eg, FXI), alterations in fibrin clot structure, and changes in NET formation, all of which have recently been linked to statin use and deserve dedicated investigation.
Finally, registry‑based studies may be influenced by the “healthy user effect,” wherein patients who are prescribed and adhere to statin therapy are often healthier, more adherent to treatment, and more engaged in health care systems than nonusers. This survivorship bias may exaggerate the apparent benefit of statins in observational settings.
In summary, although biologically plausible and supported by consistent observational data, the protective role of statins in anticoagulated VTE patients must be confirmed in rigorously designed RCTs. Until then, clinical decisions should be individualized and grounded in a balanced assessment of risks and benefits.
Future perspectives
The promising yet inconclusive nature of current evidence regarding statin use in anticoagulated VTE patients underscores the urgent need for dedicated, well‑designed prospective clinical trials. Specifically, RCTs targeting this population are essential to overcome the limitations of observational data and to confirm causality. These trials should be adequately powered to detect clinically meaningful reductions in VTE recurrence and mortality, and should stratify outcomes based on statin type, dose, duration of therapy, and concurrent anticoagulant regimens.
A key area of investigation involves identifying patient subgroups most likely to benefit from adjunctive statin therapy. Future studies should include predefined subgroup analyses based on age, comorbidities, baseline inflammatory burden (eg, CRP, IL‑6), cancer status, and genetic predispositions. These data would support personalized therapeutic approaches and help guide clinical decision‑making in complex populations.
Additionally, the role of cholesterol‑lowering–dependent vs independent mechanisms needs to be clarified. Recent evidence suggests that LDL‑C reduction itself may contribute to antithrombotic effects through favorable changes in coagulation profiles and fibrin clot structure. Integration of biomarker‑driven strategies, including measurements of thrombin generation, fibrinolytic markers, and NET‑related parameters, may help identify responsive individuals and enhance the mechanistic understanding of statin action in VTE.
Further research is warranted to evaluate the potential role of statins in CAT, a setting characterized by high thrombotic burden and limited treatment options. Preliminary data have shown that statin use may reduce recurrent events and improve survival in oncologic populations,44,46 but confirmatory trials are lacking.
Another important consideration is the impact of statin therapy on bleeding risk in anticoagulated patients. Future studies should systematically assess bleeding outcomes and investigate whether certain statin‑anticoagulant combinations pose increased hemorrhagic risk.
Finally, cost‑effectiveness analyses and quality‑of‑life assessments should be integrated into clinical trial designs. Given the widespread availability, low cost, and established safety profile of statins, even modest improvements in thrombotic outcomes could translate into significant public health benefits if their use in VTE patients is validated.
In summary, the future of statins in VTE management lies in precision medicine approaches, combining clinical risk stratification with mechanistic insights and real‑world data. Such efforts will clarify the place of statins in the secondary prevention of VTE and potentially expand their role beyond lipid lowering into the domain of antithrombotic therapy.
Conclusions
VTE remains a major global health burden despite the availability of effective anticoagulant therapies. Recurrent events and long‑term complications continue to affect a significant proportion of patients, underscoring the need for adjunctive strategies to improve outcomes. In this context, statins have emerged as promising therapeutic agents due to their pleiotropic properties, which extend well beyond lipid lowering. Their anti‑inflammatory, antithrombotic, endothelial‑stabilizing, and immunomodulatory effects offer a compelling biological rationale for potential use in VTE patients, particularly those already receiving anticoagulation.
Multiple observational studies, registry data, and meta‑analyses have consistently demonstrated an association between statin use and reduced incidence of VTE recurrence, as well as improved survival. Real‑world data from the RIETE registry further reinforce the notion that statins may exert protective effects in this setting. These effects appear especially beneficial in high‑risk subgroups, including elderly patients, those with multiple comorbidities, and individuals with CAT.
Importantly, statins appear to be safe when co‑administered with anticoagulants, including DOACs, and do not significantly increase the risk of bleeding. Nonetheless, caution is warranted in interpreting current findings due to inherent limitations in the available evidence base. Residual confounding, variability in statin types and doses, and selection bias may all influence the observed outcomes. Moreover, dedicated RCTs specifically addressing this question are lacking, limiting the ability to make definitive clinical recommendations.
Looking forward, prospective, adequately powered RCTs are essential to determine whether statins provide an independent and clinically meaningful benefit in the secondary prevention of VTE. Such studies should stratify patients based on clinical characteristics, comorbidities, and inflammatory biomarkers, and also assess bleeding risk and cost‑effectiveness. These data will help clarify the therapeutic potential of statins in a broader spectrum of VTE patients.
In conclusion, current evidence supports the hypothesis that statins may confer additional protective effects in anticoagulated VTE patients. Given their favorable safety profile, low cost, and widespread availability, statins represent a promising adjunctive option in VTE management. If ongoing and future trials confirm their benefit, statins could become an integral component of secondary VTE prevention strategies, extending their use beyond traditional lipid‑lowering indications.
- Yamashita Y, Morimoto T, Kimura T. Venous thromboembolism: Recent advancement and future perspective. J Cardiol. 2022; 79: 79‑89. | Crossref
- Raskob GE, Angchaisuksiri P, Blanco AN, et al. Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol. 2014; 34: 2363‑2371. | Crossref
- Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest. 2021; 160: e545‑e608. | Crossref
- Di Nisio M, van Es N, Büller HR. Deep vein thrombosis and pulmonary embolism. Lancet. 2016; 388: 3060‑3073. | Crossref
- Klok FA, van der Hulle T, den Exter PL, et al. The post‑PE syndrome: a new concept for chronic complications of pulmonary embolism. Blood Rev. 2014; 28: 221‑226. | Crossref
ARTICLE INFORMATION