Therapeutic challenge of advanced melanoma: exceptional response to combined immunotherapy

 CC BY 4.0
CC BY 4.0
Therapeutic challenge of advanced melanoma: exceptional response to combined immunotherapy
A 30‑year‑old patient was referred to the Maria Skłodowska‑Curie National Research Institute of Oncology in Warsaw with massive, nonoperable nodal involvement, which hindered upper extremity movements. Histopathologic and molecular analyses confirmed the diagnosis of BRAF V600E‑mutant melanoma of unknown primary origin, metastasized to the right axillary lymph nodes, with the largest lesion measuring 74 mm × 46 mm (cTxN3bM0, American Joint Committee on Cancer, 8th edition; Figure 1A). Apart from a positive family history of melanoma, the patient had no other identifiable risk factors. Following clinical evaluation, she was qualified for combined immune checkpoint inhibitor (ICI) therapy with ipilimumab and nivolumab, initiated on October 6, 2022.
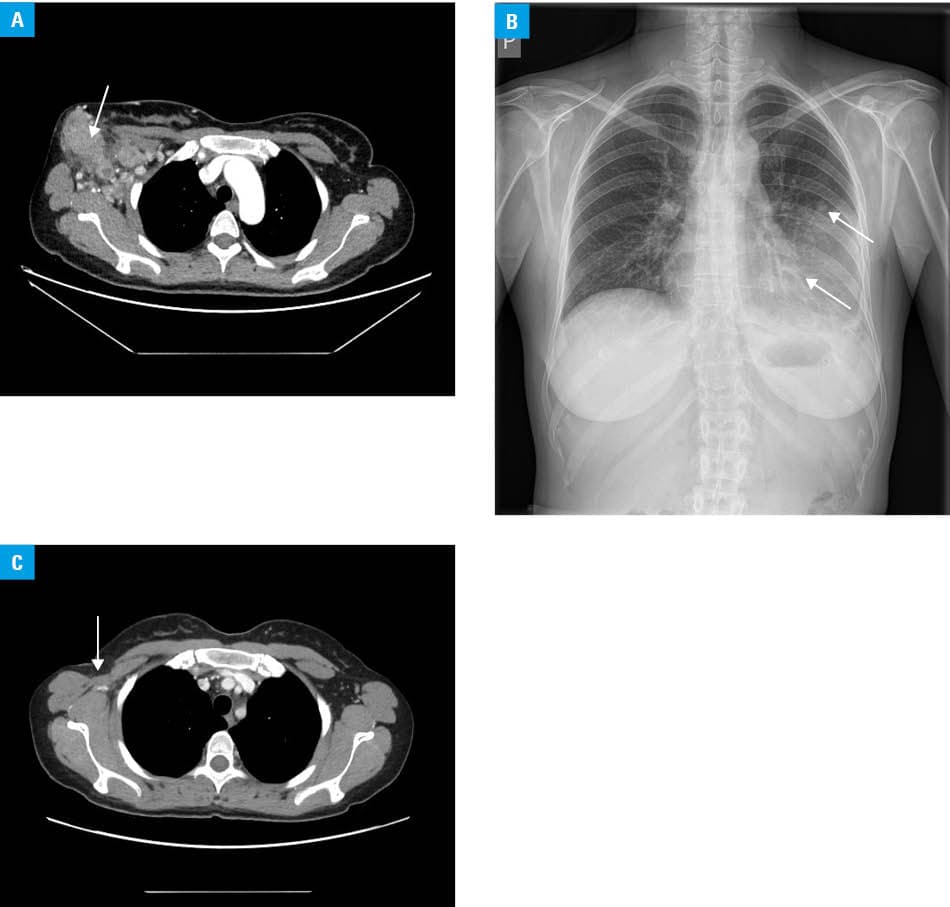
During the first 3 months of combined ICI treatment, the patient experienced several immune‑related adverse events, including gastrointestinal toxicity and hepatotoxicity manifesting with hyperbilirubinemia (27.6 µmol/l; reference range, 5–21 µmol/l), while liver enzyme levels remained within normal limits. The most clinically significant adverse event was immune‑mediated pneumonitis, which resulted in exertional dyspnea and decreased oxygen saturation (94%). Chest radiography showed pulmonary infiltrates and atelectasis in the left lingular region (Figure 1B). Despite these complications, the patient demonstrated a favorable therapeutic response and achieved a significant reduction in tumor size, enabling surgical resection.
Right axillary lymphadenectomy resulted in the removal of 44 lymph nodes, 5 of which showed metastatic involvement with areas of tumor necrosis. The patient continued systemic treatment with nivolumab monotherapy. Due to the development of thyroiditis, manifesting as hyperthyroidism and exacerbation of psoriasis, the treatment was discontinued after 6 months of pseudoadjuvant therapy. The patient completed a total of 10 immunotherapy cycles. Post‑treatment positron emission tomography did not identify any lesions with high metabolic activity. Follow‑up computed tomography confirmed radiologic stability, with no recurrence observed (Figure 1C).
In the early stages of melanoma, surgery alone can lead to successful treatment and high survival rates, which decrease substantially once the cancer metastasizes.1 ICIs have remarkably improved treatment outcomes in advanced melanoma, resulting in significantly better objective response, progression‑free survival, and overall survival rates.2 The presented case of stage IIIC melanoma, achieving a complete response with combined immunotherapy followed by surgical resection, represents a particularly rare and favorable outcome.
Immune‑related adverse events affect approximately 40% of patients receiving checkpoint inhibitors and frequently involve multiple organs. Importantly, they often lead to treatment interruptions and high‑dose corticosteroid therapy, which can complicate and even compromise ongoing cancer treatment. This underscores the importance of vigilance regarding the diverse spectrum of immune‑related toxicities, including not only pneumonitis, hepatitis, or thyroiditis, as seen in our patient, but also rarer complications, such as checkpoint inhibitor–induced panhypophysitis with central diabetes insipidus.3,4
This case highlights the transformative potential of immunotherapy in advanced melanoma, where complete responses in highly advanced stages remain exceptional. It underscores the critical importance of a multidisciplinary approach and awareness in the management of immune‑related adverse events, which enables treatment continuation and sustained therapeutic benefit.
- Davis LE, Shalin SC, Tackett AJ. Current state of melanoma diagnosis and treatment. Cancer Biol Ther. 2019; 20: 1366‑1379. | Crossref
- Hodi FS, Chiarion‑Sileni V, Gonzalez R, et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4‑year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018; 19: 1480‑1492. | Crossref
- Keam S, Turner N, Kugeratski FG, et al. Toxicity in the era of immune checkpoint inhibitor therapy. Front Immunol. 2024; 15: 1447021. | Crossref
- Cylke‑Falkowska K, Czajka‑Oraniec I, Stelmachowska‑Banaś M, Zgliczyński W. Immune checkpoint inhibitor‑induced central diabetes insipidus in the course of panhypophysitis. Pol Arch Intern Med. 2024; 134: 16672. | Crossref
ARTICLE INFORMATION