Pulmonary vein isolation with radiofrequency ablation and pulsed-field ablation: follow-up with real-world data
Key words: atrial fibrillation, catheter ablation, pulmonary vein isolation, pulsed-field ablation, radiofrequency ablation

 CC BY 4.0
CC BY 4.0
Pulmonary vein isolation with radiofrequency ablation and pulsed-field ablation: follow-up with real-world data
Introduction: Currently, the treatment of atrial fibrillation (AF) focuses on restoring sinus rhythm with pulmonary vein isolation (PVI). Pulsed‑field ablation (PFA) is a novel, promising method that requires greater support of real‑world data.
Objectives: Our aim was to assess the rate of arrhythmia recurrence in patients who underwent PVI with either radiofrequency (RF) energy or PFA.
Patients and methods: This retrospective analysis included 210 patients with paroxysmal (76.2%) or persistent AF undergoing PVI at a university hospital. The study group consisted of 108 patients who underwent PFA using the Farawave catheter. RF ablations were performed in 102 patients using a very‑high‑power, short‑duration or index‑guided ablation. The primary end point was no recurrence of arrhythmia.
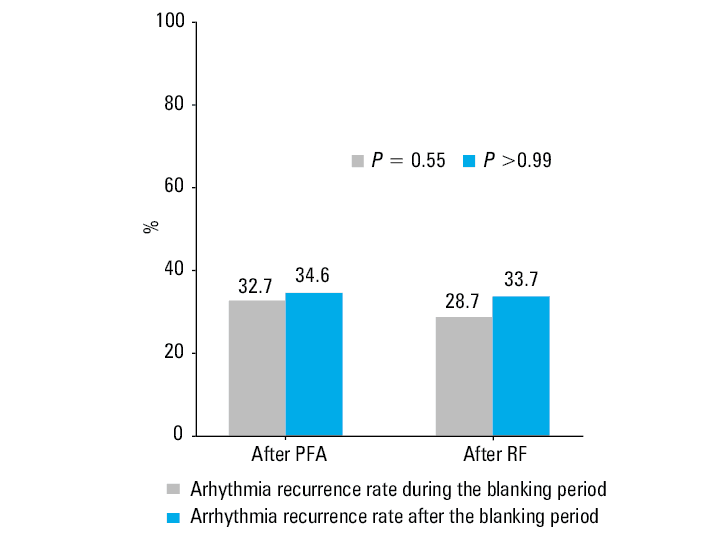
Results: There were no significant baseline differences in patient characteristics. Procedural times were shorter with PFA (55 min) than RF (115 min; P <0.001), while fluoroscopy exposure duration was longer (PFA, 1100 s; RF, 159 s; P <0.001). In the patients who underwent PFA under deep sedation, remifentanil dose was lower than in the RF group under conscious sedation (PFA, 0.2 mg; RF, 0.5 mg; P <0.001). The efficacy of both methods did not differ in the recurrence rate of atrial arrhythmias during the blanking period (PFA, 32.7%; RF, 28.7%; P = 0.55) and afterward (PFA, 34.6%; RF, 33.7%; P >0.99). The overall frequency of adverse events was similar in both groups.
Conclusions: Regardless of the selected method, the efficacy of the procedures remains comparable. There was no significant difference in postoperative adverse events between the groups.
What's new?
Atrial fibrillation is becoming increasingly common, and new treatment methods continue to evolve. Pulsed‑field ablation (PFA) is a novel technique for pulmonary vein isolation that has gained significant attention. Our study demonstrates that PFA procedures are shorter than radiofrequency ablation, although they entail greater fluoroscopy exposure. Importantly, both methods show similar safety profiles and comparable rates of arrhythmia recurrence. The potential clinical benefit of PFA lies in its efficiency, allowing more procedures to be performed in a given time frame, which could help reduce waiting lists. However, further research is needed to fully establish the long‑term advantages and optimize the use of PFA in clinical practice.

Introduction
The development of technological concepts and strategies in electrophysiology over the last few decades has increasingly informed guideline recommendations for catheter‑based ablation in the management of cardiac arrhythmias. The aging population faces chronic diseases that contribute to the growing prevalence of arrhythmias, with atrial fibrillation (AF) occurring most often.1,2 Therefore, heart rhythm control, symptom alleviation, and stroke prevention still pose challenges in contemporary cardiology.
Pulmonary vein isolation (PVI) is a standard ablation strategy for treating AF in symptomatic patients. The procedure is typically performed using thermal methods, such as cryoablation or radiofrequency (RF) ablation, which induce coagulative necrosis.3 A more recent approach for PVI is nonthermal pulsed‑field ablation (PFA), which selectively damages cardiomyocytes by delivering microsecond high‑voltage currents. This causes irreversible electroporation and destabilization of cell membranes, leading to cellular necrosis with minimal effects on the esophagus, phrenic nerve, and pulmonary vein tissue.4
PFA is believed to reduce the risk of serious adverse events (SAEs), such as atrioesophageal fistula, phrenic nerve palsy, pulmonary vein stenosis, and cerebral ischemia due to the unique mechanism of lesion formation.5
The evidence regarding the efficacy and safety of PFA in comparison with thermal methods remains limited, particularly with respect to real‑world data. A multicenter, prospective, randomized controlled ADVENT trial (A Prospective Randomized Pivotal Trial of the FARAPULSE Pulsed Field Ablation System Compared With Standard of Care Ablation in Patients with Paroxysmal Atrial Fibrillation) demonstrated that PFA was noninferior to the RF technique in terms of freedom from atrial tachyarrhythmia in patients with paroxysmal AF after 1 year of follow‑up.4 Real‑world data are still necessary to delineate procedural differences across varying ablation approaches.
The aim of this study was to compare PFA and RF in terms of procedural variables and long‑term outcomes. We focused on evaluating the outcomes, durability, and complication rates in a consecutive cohort of patients undergoing ablation for paroxysmal or persistent AF.
Patients and methods
Study design
A total of 210 consecutive patients with symptomatic paroxysmal or persistent AF were enrolled in this retrospective, observational study. The majority of the participants were not responding to antiarrhythmic drugs, although some had ablation performed as first‑line therapy. The decision regarding the need for the procedure was made in collaboration with the patient after carefully analyzing the advantages and disadvantages of the treatment. Eligibility of all patients was assessed according to the current European Society of Cardiology guidelines5 and baseline characteristics, with PVI being the preferred method for rhythm control.
The exclusion criteria were age below 18 years, a history of surgical or percutaneous ablation for AF, and the presence of appendage thrombus on preprocedural transesophageal echocardiography (TEE). The study procedures were performed between January and December 2023 at a tertiary care center in Poland, where approximately 700 procedures are performed annually for all types of arrhythmias, with the use of RF, cryoablation, and PFA. We compared 2 catheter ablation methods, PFA and RF. RF ablations were performed using a very‑high‑power, short‑duration (vHPSD) catheter, QDot Micro (Biosense Webster, Inc., Irvine, California, United States), or an ablation index (AI)-guided ThermoCool Smarttouch SF catheter (Biosense Webster, Inc.). The PFA procedures were conducted using the Farawave catheter (Boston Scientific, Menlo Park, California, United States). The choice of ablation modality was at the physicians’ discretion. At the time of introducing PFA as a new method in our center, all patients with no history of other atrial arrhythmias meeting the above criteria were eligible for their first procedure.
The patients were referred for a routine postdischarge appointment at an outpatient clinic, where they were assessed for symptomatic improvement and late complications. They were also scheduled for a 24‑hour Holter electrocardiogram (ECG) at 3, 6, and 12 months postablation, followed by an in‑person visit. Additionally, the patients were followed‑up via telephone to gather information on postablation arrhythmic symptoms and potential recurrences, and to determine whether any further cardioversion or other procedures were required if no on‑site visit took place.
Study population
All 108 patients who underwent PFA during the study period were included in the analysis. Two patients died from causes unrelated to treatment (one due to exacerbation of end‑stage kidney failure in the course of autosomal dominant polycystic kidney disease), and 1 was reported to have arrhythmia recurrence 16 weeks after ablation. Follow‑up data for the latter patient could not be obtained; therefore, the patient was excluded from the analysis of freedom from arrhythmia. A total of 102 consecutive patients treated with RF ablation were included in the study, with 1 patient withdrawing their consent to participate in the analysis. This control group was heterogeneous, reflecting the real‑world clinical practice and availability of catheters used in a standard electrophysiological laboratory. Fifty‑three patients (52%) underwent vHPSD procedure, while the remaining 49 individuals were treated with AI‑guided ablation. In this study, we did not focus on the subanalysis of the RF group, since our current aim was to compare the RF and PFA methods. Similar number of patients undergoing each procedure minimizes potential variability in procedural or clinical data.
Procedural workflow
Prior to ablation, almost all patients underwent TEE to rule out intracardiac thrombus in the left atrial appendage and to assess the interatrial septum. The CHA2DS2-VASc score below 2, sinus rhythm on admission, and regular adherence to anticoagulant therapy allowed for the omission of preprocedural TEE according to our internal standards. The catheters were inserted via the femoral veins under local anesthesia. In each procedure, a 10‑pole diagnostic catheter was introduced into the coronary sinus. Unfractionated heparin was infused to maintain the activated clotting time above 355 seconds during the procedure, with the first bolus dose (100 IU/kg) administered before transseptal puncture. Left atrial access was obtained via fluoroscopy‑guided and pressure‑guided transseptal puncture. A 3‑dimensional reconstruction of the left atrium and pulmonary veins was created using rotational angiography in patients with an estimated glomerular filtration rate above 30 ml/min/1.73 m2. Durability of PVI was checked by pacing (exit block) for all PFA patients or pacing maneuvers (exit block) and left atrium remapping in the patients who underwent RF ablation.
Study group procedure workflow
Typically, the patients were sedated with propofol boluses and received infusions of remifentanil for pain management during the procedure. The Farawave catheter was used to isolate the pulmonary veins under fluoroscopy. Each pulmonary vein received 4 applications using the basket catheter and 4 applications using the flower configuration catheter to complete the standard 32‑application lesion set. Additional applications between the veins were delivered at the operator’s discretion. One patient in the PFA group had the posterior wall application performed. Electrical isolation was assessed by exit block testing with pacing.
Control group procedure workflow
In the RF group, a 20‑pole LassoNav or PentaRay catheter (Biosense Webster, Inc.) and the CARTO electroanatomic navigation system (Biosense Webster, Inc.) were used to construct the map. The catheters were chosen at the discretion of the operator.
For vHPSD ablation, the QMode+ algorithms were applied, delivering 4 seconds of 90‑W applications via the Qdot Micro catheter (Biosense Webster, Inc.). Each RF application in this mode was preceded by a 2‑second precooling phase and a 4‑second irrigation flow (8 ml/min).
During AI‑guided ablation, PVI was performed in accordance with the CLOSE protocol via the Thermocool Smarttouch Surround Flow catheter (Biosense Webster, Inc.).6 The power output was set to 35 W, aiming for a target AI above 400 on the superior, posterior, and inferior walls of the left atrium, and above 550 on the anterior wall. The target contact force range was 10–30 g, with an irrigation flow rate of 15 ml/min.
The maximum temperature cutoff point was 55 °C for the Qdot Micro catheter and 40 °C for the Thermocool Smarttouch SF catheter. Once this temperature threshold was reached, the catheters were automatically switched off.
Primary and secondary outcomes
The primary end point was freedom from arrhythmia recurrence. In our study, the blanking period was defined as the first 3 months postablation. During this period, the episodes of atrial tachyarrhythmias (AF or atrial tachycardia [AT]) were not considered as the recurrence of arrhythmia. However, if the arrhythmia was triggered during the blanking period and recurred beyond 3 months postprocedure, it was included in the recurrence rate. The diagnosis of AF or AT recurrence was based on the results of Holter ECG performed after the 3‑month blanking period, as well as at 6 and 12 months after the procedure or any ECG recorded after 3 months postdischarge. Smartwatches worn by some patients, as well as mobile medical devices designed for self‑monitoring of ECG proved to be helpful, as they could easily identify AF based on ECG, which assisted in detecting the episodes of arrhythmia.
The secondary outcome was the assessment of procedural safety, which was defined as the occurrence of SAEs and minor complications from the time of procedure to hospital discharge. SAEs were defined as death, myocardial infarction, cardiac tamponade, phrenic nerve injury, cerebrovascular accident, transient ischemic attack, significant bleeding, thromboembolic events, or other vascular complications. Minor complications related to vascular access included groin hematoma, pseudoaneurysm, or arteriovenous fistula. Transthoracic echocardiography was carried out after ablation and on the following day before discharge. If the patients experienced such symptoms as pain, edema, bleeding, or vascular murmur indicating potential vascular complications, ultrasonography of the puncture site was performed.
Additionally, several data points were compared in this study, such as the procedure and fluoroscopy times, administration of remifentanil and heparin during ablation, and medication dosages for home administration depending on the employed method. All the aforementioned data were extracted from medical records.
Data collection
All PVI ablations were carried out by 5 electrophysiologists, each performing over 50 PVI procedures annually. A database containing procedural and clinical data was created by a single independent researcher. Additionally, an investigator conducted interviews with all patients for at least 3 months following ablation. Follow‑up visits at the outpatient clinic typically involved the physicians who performed the procedures at our center.
Statistical analysis
The distribution of continuous variables in the analyzed subgroups was assessed using the Shapiro–Wilk test. Results are presented as median and interquartile range (IQR) for variables with non‑normal distribution in at least 1 group and as mean (SD) for normally distributed variables in both groups. Categorical variables are reported as number and percentage of participants. The Fisher exact test was used to compare categorical variables. The t test and the Mann–Whitney test were used for normally and non‑normally distributed continuous variables, respectively. The log‑rank test was used to compare arrhythmia‑free time distributions between the groups. The Kaplan–Meier survival curve was plotted to analyze AF recurrence in both groups. A P value below 0.05 was considered significant. The statistical analysis was performed with Statistical Analysis Software, version 9.4 (SAS, Cary, North Carolina, United States).
Ethics
The study was approved by the Institutional Review Board of the Medical University of Warsaw (AKBE/127/2022), and was conducted in accordance with the ethical principles of the Declaration of Helsinki. Written informed consent for AF ablation was obtained from all patients.
Results
Baseline characteristics
Over the study period, 210 PVI ablation procedures were performed, with no significant differences in patient characteristics between the PFA and the RF groups, including median (IQR) age (67 [59–74] vs 67 [61–72] y; P = 0.89) and sex (41.7% vs 43.1% women; P = 0.89). The population undergoing PVI had more often paroxysmal than persistent AF, but there was no disproportion between the methods (PFA, 86 [79.6%]; RF, 74 [72.5%]; P = 0.26). Antiarrhythmic medications were prescribed at the discretion of the attending cardiologist, with a nonsignificantly more frequent administration in the RF group. Our study demonstrated higher prevalence of β-blocker use in the patients undergoing RF ablation (PFA, 83 [76.9%]; RF, 90 [88.2%]; P = 0.045). General characteristics of the population and medications prescribed after ablation are summarized in Table 1.
Variable | Total (n = 210) | PFA group (n = 108) | RF group (n = 102) | P value |
Data are provided as number and percentage or median (interquartile range) unless indicated otherwise.
SI conversion factors: to convert hemoglobin to mmol/l, multiply by 0.0626; creatinine to μmol/l, by 8.842.
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitors; AF, atrial fibrillation; ARB, angiotensin receptor blockers; ASA, acetylsalicylic acid; BMI, body mass index; CAD, coronary artery disease; CRP, C‑reactive protein; eGFR, estimated glomerular filtration rate; Hb, hemoglobin; PAD, peripheral artery disease; PFA, pulsed‑field ablation; RF, radiofrequency; TIA, transient ischemic attack; WBC, white blood cell count | ||||
Age, y | 67 (60–73) | 67 (59–74) | 67 (61–72) | 0.89 |
BMI, kg/m2, mean (SD) | 29.2 (4.3) | 29.5 (4.6) | 29 (3.9) | 0.46 |
Women | 89 (42.4) | 45 (41.7) | 44 (43.1) | 0.89 |
Paroxysmal AF | 160 (76.2) | 86 (79.6) | 74 (72.5) | 0.26 |
Hypertension | 150 (71.4) | 74 (68.5) | 76 (74.5) | 0.36 |
Heart failure | 32 (15.2) | 18 (16.7) | 14 (13.7) | 0.57 |
Stroke / TIA | 10 (4.8) | 6 (5.6) | 4 (3.9) | 0.75 |
CAD/PAD | 44 (21) | 23 (21.3) | 21 (20.6) | >0.99 |
Diabetes | 30 (14.3) | 16 (14.8) | 14 (13.7) | 0.85 |
CHA2DS2VASc score | 2 (1–3) | 2 (1–4) | 2.5 (1–3) | 0.62 |
Hb, g/dl, mean (SD) | 14.2 (1.4) | 14.1 (1.4) | 14.3 (1.4) | 0.39 |
WBC, × 109/l, mean (SD) | 7.4 (1.8) | 7.6 (1.8) | 7.2 (1.7) | 0.15 |
Creatinine, mg/dl | 1 (0.9–1) | 1.1 (0.9–1.2) | 1 (0.9–1) | 0.56 |
eGFR, ml/min/1.73 m2, mean (SD) | 68.6 (18) | 68.3 (18.4) | 68.8 (17.7) | 0.84 |
CRP, mg/l | 1.0 (0.6–2) | 1 (0.6–2) | 1.2 (0.6–2.1) | 0.66 |
Antiarrhythmics class I | 13 (6.2) | 5 (4.6) | 8 (7.8) | 0.4 |
Amiodarone | 2 (0.9) | 1 (0.9) | 1 (1) | >0.99 |
β-Blockers | 173 (82.4) | 83 (76.9) | 90 (88.2) | 0.04 |
ACEI/ARB | 138 (65.7) | 66 (61.1) | 72 (70.6) | 0.19 |
Statins | 116 (55.2) | 58 (53.7) | 58 (56.9) | 0.68 |
Calcium blockers | 66 (31.4) | 31 (28.7) | 35 (34.3) | 0.46 |
Rivaroxaban | 29 (13.8) | 14 (13) | 15 (14.7) | 0.84 |
Apixaban | 134 (63.8) | 67 (62) | 67 (65.7) | 0.67 |
Dabigatran | 42 (20) | 26 (24.1) | 16 (15.7) | 0.17 |
Vitamin K antagonist | 4 (1.9) | 1 (0.9) | 3 (2.9) | 0.36 |
ASA | 3 (1.4) | 3 (2.8) | 0 | 0.25 |
P2Y12 inhibitors | 2 (1) | 0 | 2 (2) | 0.23 |
Primary end points
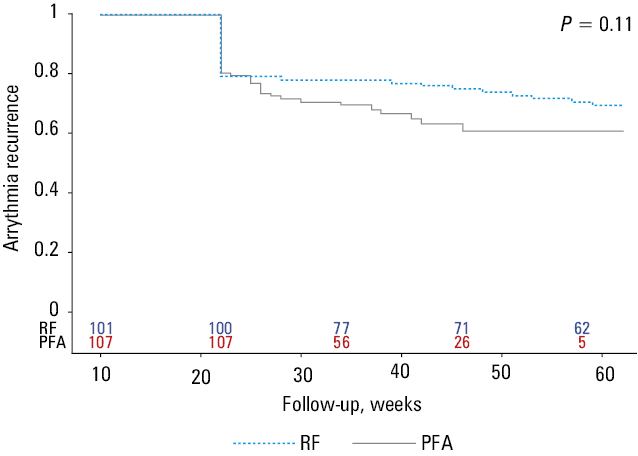
Acute PVI was successful in all patients. The efficacy of the 2 methods did not differ in terms of atrial arrhythmia recurrence rates during the blanking period (PFA, 32.4%; RF, 28.4%; P = 0.55) or afterward (PFA, 34.3%; RF, 33.3%; P >0.99). Two patients in the PFA group (1.9%) and 4 in the RF group (3.9%) experienced AF recurrence before discharge (P = 0.43). All values are presented in Table 2. The timeline of arrhythmia recurrence is shown on the Kaplan–Meier survival curves in Figure 1. The rates of arrhythmia recurrence without the blanking period considering both methods are presented in Figure 2.
Variable | Total (n = 210) | PFA group (n = 108) | RF group (n = 102) | P value |
Data are presented as number and percentage or median (interquartile range).
Abbreviations: TEE, transesophageal echocardiography; others, see Table 1 | ||||
TEE before the procedure | 168 (80) | 89 (82.4) | 79 (77.5) | 0.39 |
Procedure time, min | 85 (55–115) | 55 (45–70) | 115 (100–135) | <0.001 |
Fluoroscopy time, s | 603.5 (165–1087) | 1100 (800–1400) | 159 (88–335) | <0.001 |
Heparin administered during the procedure, thousands of units | 19 (15–23) | 18 (15–20) | 21 (17–24) | <0.001 |
Remifentanil administered during the procedure, mg | 0.3 (0.2–0.5) | 0.2 (0.15–0.3) | 0.5 (0.3–0.6) | <0.001 |
Pericardial effusion | 7 (3.3) | 4 (3.7) | 3 (2.9) | >0.99 |
Vascular complications | 1 (0.5) | 1 (0.9) | 0 | >0.99 |
Pseudoaneurysm | 1 (0.5) | 0 | 1 (1) | 0.49 |
Arteriovenous fistula | 1 (0.5) | 1 (0.9) | 0 | >0.99 |
Stroke | 0 | 0 | 0 | – |
AF before discharge | 6 (2.9) | 2 (1.9) | 4 (3.9) | 0.43 |
Cardioversion | 35 (16.7) | 17 (16.7) | 18 (17.6) | 0.72 |
Postprocedural hospitalization, d | 1 (1–1) | 1 (1–1) | 1 (1–1) | 0.15 |
Abbreviations: see Table 1
Abbreviations: see Table 1
Secondary end points
The overall rate of major and minor complications was low, irrespective of the ablation technique (PFA, 5.6%; RF, 3.9%). Pericardial effusion occurred in 4 patients in the PFA group and 3 patients in the RF group. In the former group, delayed tamponade occurred 1 day after PVI, requiring a surgical intervention. A vascular complication occurred in 1 patient who underwent PFA ablation and 1 individual in the RF group developed a pseudoaneurysm. Importantly, there were no cases of atrioesophageal fistula, stroke, or phrenic nerve injury. A list of adverse events is provided in Table 2.
Other study end points
Median (IQR) procedural times were reduced with PFA (55 [45–70] min) as compared with RF (115 [100–135] min; P <0.001), while fluoroscopy exposure duration was notably longer for PFA (1100 [800–1400] s) than for RF (159 [88–335] s; P <0.001). In the patients who underwent PVI with PFA, the remifentanil dose (PFA, 0.2 [0.15–0.3] mg; RF, 0.5 [0.3–0.6] mg) and heparin dose (PFA, 18 000 [15 000–20 000] IU; RF: 21 000 [17 000–24 000] IU) were lower than those required for RF ablation (P <0.001). The PFA procedures were performed under deep sedation, while RF procedures were performed under conscious sedation. The procedural data are presented in Table 2.
Discussion
This study comparatively analyzed efficacy, procedural data, and safety of PFA and RF ablations. The major findings were as follows: 1) arrhythmia recurrence rates were comparable for both methods; 2) both techniques were associated with a low risk of SAEs; 3) the patients undergoing PFA required administration of lower doses of remifentanil and heparin; 4) the PFA procedures were significantly shorter, although overall fluoroscopy exposure time was longer. Discussions are ongoing regarding the potential benefits of the new method, including catheter stability, shorter procedure time, and similar efficacy to thermal techniques.3 Our results contribute to the ongoing debate regarding optimal energy sources in patients undergoing PVI.
Safety
The implementation of PFA in the management of arrhythmias is expected to be a breakthrough in terms of safety. According to the MANIFEST‑PF survey (Multi‑National Survey on the Methods, Efficacy, and Safety on the Post‑Approval Clinical Use of Pulsed Field Ablation), the method based on electroporation and selectivity of cardiomyocyte destruction can reduce the risk of collateral damage.7 The researchers found no PFA‑specific adverse events, such as esophageal complications, PV stenosis, or persistent phrenic nerve injury, providing evidence for the specificity of tissue sensitivity.7 Histopathological examination of cardiac, esophageal, and phrenic nerve tissue also showed differences in the depth of the damage. High‑intensity PFA applications had no influence on the esophagus or phrenic nerve tissue, whereas RF ablation destroyed the muscularis propria and adventitia layers.8 Studies focusing on the biophysics of thermal ablations have shown that RF lesions can reach a depth of up to 4 mm, which is sufficient in thinner areas of the heart wall for myocardial necrosis.9 In contrast, PFA can penetrate 5 to 6 mm into the tissue, safely creating lesions.10 This generally allows the operator to apply energy to the posterior wall of the left atrium without concern for potential damage. Simultaneously, creating deeper lesions enables targeting fibrotic or thicker areas of the heart wall, potentially increasing the effectiveness of PVI.
Our study confirmed the absence of the complications mentioned above, and we also observed that, regardless of the method used, the overall AE rates were comparable (PFA, 5.56%; RF, 3.92%). The SAEs for PFA were estimated to occur in 0.93% cases, while the rate of minor complications was 4.6%. In the RF group, no SAEs were reported, and the minor complication rate was 3.9%. Our results align with recent data published by Reddy et al,4 where the device- or procedure‑related SAEs were estimated at 2.1% for PFA and 1.5% for RF ablations. Moreover, a multicenter MANIFEST‑17K study (Multi‑National Survey on the Safety of the Post‑Approval Clinical Use of Pulsed Field Ablation in 17 000+ Patients), which involved 17 642 patients, estimated the overall AE rate after PFA at 4.19%, with SAEs at 0.98% and minor AEs at 3.21%.11
Follow‑up
Our research suggests that PFA is noninferior to thermal ablation with respect to arrhythmia recurrence rates. Regarding the selected method, freedom from AF was comparable during the blanking period (PFA, 32.4%; RF, 28.4%), and later follow‑up (PFA, 34.3%; RF, 33.3%). In multicenter studies and trials, the efficacy of ablation procedures using the PFA method has been reported to be 66.2% in patients with paroxysmal AF and 55.1% in those with persistent AF,12 and 74% in patients affected with both paroxysmal and persistent AF.13 Mean (SD) freedom from AF rate at 1 year in the IMPULSE (A Safety and Feasibility Study of the IOWA Approach Endocardial Ablation System to Treat Atrial Fibrillation), PEFCAT (A Safety and Feasibility Study of the FARAPULSE Endocardial Ablation System to Treat Paroxysmal Atrial Fibrillation), and PEFCAT II (Expanded Safety and Feasibility Study of the FARAPULSE Endocardial Multi Ablation System to Treat Paroxysmal Atrial Fibrillation) trials was estimated to be 81.1% (3.8%) in patients with paroxysmal AF.14,15 It is noteworthy that our center did not participate in the aforementioned multicenter studies, but the results of our analysis closely resembled those reported. The issue of follow‑up duration also warrants consideration. According to the European Society of Cardiology guidelines compulsory at the time of the study, the blanking period was defined as the first 3 months postablation, during which any recurrence of AF, atrial flutter, or AT was not considered a failure of the procedure nor was it indicative of long‑term AF recurrence. Based on current evidence, the authors of the guidelines recommended a 2‑month blanking period.1,16 In the majority of the studies included in our discussion, a blanking period lasted 3 months, so the comparison seems valid.
It is worth pointing out that the timing and pattern of AF or AT recurrence both prior to discharge and during the blanking period differ between the ablation techniques. The available data suggest that distinct short‑term (ischemia, myocardial necrosis, oxidative stress, myocardial edema) and long‑term (inflammation, proliferative tissue repair) processes play a role in tissue regeneration following thermal or PFA methods.
Importantly, the early postablation effects on electrograms cannot be assessed after PFA because myocardium remains stunned longer than in the case of RF.17 Moreover, transient inflammation is increased in the RF method, making early recurrences in this group more likely. The DECAAF II study (Efficacy of Delayed Enhancement MRI‑Guided Ablation vs Conventional Catheter Ablation of Atrial Fibrillation) explained that arrhythmia recurrences in the third month after PFA were highly associated with later arrhythmic episodes, whereas early recurrences in the RF group were more frequently transient.18 These findings contributed to an expert consensus recommending a shorter postablation blanking period.1 This allows for earlier detection of clinically relevant AF recurrences.
Differences in follow‑up data collection, ablation technique, and patient characteristics can affect study outcomes, making comparisons difficult. Consequently, it is still crucial to gather and share a comprehensive range of real‑world data. Not enough articles comparing the efficacy of PFA and other PVI methods have been published. According to Reddy et al,4 the reported probability of procedural success was 73.3% for PFA and 71.3% for thermal ablation. The consistency of these findings with those of Badertscher et al19 supports the conclusion of relative effectiveness of the 2 treatment methods, which aligns with our findings.
Procedural data
Several previous studies have indicated that PFA is associated with reduced procedure time but prolonged fluoroscopy exposure. The overall procedure time in our study (55 min; range, 45–70 min) was similar to the one in the MANIFEST‑PF survey (65 min; range, 38–215 min) and to the mean (SD) procedure time in the first‑in‑human PFA trials of 96.2 (30.3) minutes.7,14 When comparing theses values with the duration of RF ablation, which is 115 minutes (range, 110–135 min), the advantage of performing PFA is clear. The duration of the procedure is directly related to the time the catheters are placed in the left atrium, which can lead to more frequent occurrences of cerebral ischemia. The issue of longer fluoroscopy times should be considered in light of potential reduction in workplace safety. The higher radiation exposure associated with PFA is likely related to a lack of electroanatomical mapping systems.
Anesthesia during PFA remains a subject of ongoing debate. Initial reports, which served as recommendations, indicated that general anesthesia (GA) was required.1 However, relieving pain from a contracted diaphragm and reducing anxiety are not the only factors influencing the effectiveness of the procedures. An important purpose of GA is to maximize catheter stability and the accuracy of electroanatomical mapping. Recent studies; however, have shown that deep sedation protocols may offer more advantages than previous techniques. In an analysis by Grimaldi et al,20 patients received dexmedetomidine, midazolam, and remifentanil, which demonstrates that a deep sedation protocol is a valid alternative to GA.
At our center, PVI is conducted under continuous analgesia, primarily with remifentanil in patients undergoing RF ablation. A previous study from our department demonstrated a reduction in remifentanil administration with the vHPSD method, as compared with the AI‑guided procedure.21 In this study, the median (IQR) dose of remifentanil administered during PFA (0.2 [0.15–0.3] mg) was significantly lower than that required for RF ablation (0.5 [0.3–0.6] mg). These observations are unambiguous enough to suggest that PFA represents a next step in pain and anesthesia management for patients undergoing PVI. Moreover, propofol was introduced during PFA, whereas it was not used in RF procedures. Therefore, comparing the doses of propofol administered in the study and control group was impossible. The German Society of Cardiology statement on cardioanalgosedation suggests that AEs occur less frequently with RFA, and sedation does not require the involvement of an anesthesiologist. However, the staff must be trained in cardiac sedation and advanced cardiac life support.22
An important observation from our study is the decreased rate of prescribed β-blockers following PFA procedures, as compared with RF. The increased resting heart rate in patients after thermal ablation is a common consequence of modifications to the cardiac autonomic nervous system. β-Blockers are among the most frequently prescribed medications for reducing heart rate.23 This correlation suggests that PFA may not directly influence the collateral nerves. Musikantow et al24 reported minimal influence of PFA on cardiac ganglionated plexi, resulting in the absence of significant heart rate changes following the procedure. Their study demonstrated that within the blanking period, thermal ablation was associated with an approximate 10‑bpm increase in resting heart rate, whereas no significant change was observed after PFA. The outcomes were supported by electroanatomical mapping of the ablated regions and assessment of vagal responses at the location of ganglionated plexi.
The implementation of PFA indicates many of the advantages mentioned above, positioning it as the next step in the ongoing revolution in electrophysiology.
Study limitations
Our study has several limitations. First, this was a retrospective cohort study, in which the groups were not randomized, and the characteristics of the included patients were not controlled. Second, since the follow‑up data were collected remotely, there is a possibility that information regarding AF recurrence and its documentation may have been inaccurate. Third, the study included PFA procedures that were performed in accordance with the electrophysiologist learning curve at our center. Another inherent limitation typical of retrospective studies is the fact that some patients were lost to follow‑up, but their number was comparable in both groups. Finally, the echocardiographic images could not be presented due to a lack of software saving the data for longer than 3 months.
Conclusions
Regardless of the selected method, the efficacy of PVI, and, consequently, the absence of arrhythmia recurrence, remain comparable. There was no significant difference in the occurrence of postoperative AEs between PFA and RF. Considering the reduced procedure time and safety equivalent to that of RF, more PFA procedures can be performed in the same timeframe. This enables health care providers to respond to the needs of the growing population of patients with AF more effectively.
- Tzeis S, Gerstenfeld EP, Kalman J, et al. 2024 European Heart Rhythm Association / Heart Rhythm Society / Asia Pacific Heart Rhythm Society / Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace. 2024; 26: euae043. | Crossref
- Mitrega K, Sredniawa B, Sokal A, et al. Does atrial fibrillation still increase the risk of death? One‑year follow‑up results of the NOMED‑AF study. Pol Arch Intern Med. 2024; 134: 16619. | Crossref
- Bisignani A, Schiavone M, Solimene F, et al. National workflow experience with pulsed field ablation for atrial fibrillation: learning curve, efficiency, and safety. J Interv Card Electrophysiol. 2024; 67: 2127‑2136. | Crossref
- Reddy VY, Gerstenfeld EP, Natale A, et al. Pulsed field or conventional thermal ablation for paroxysmal atrial fibrillation. N Engl J Med. 2023; 389: 1660‑1671. | Crossref
- Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio‑Thoracic Surgery (EACTS): developed by the task force for the management of atrial fibrillation of the European Society of Cardiology (ESC), with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Endorsed by the European Stroke Organisation (ESO). Eur Heart J. 2024; 45: 3314‑3414.
ARTICLE INFORMATION