Unique case of atypical hemolytic syndrome associated with Purtscher retinopathy and cerebral aneurysm

 CC BY 4.0
CC BY 4.0
Unique case of atypical hemolytic syndrome associated with Purtscher retinopathy and cerebral aneurysm
A 29‑year‑old woman with a history of hypothyroidism and occasional smoking presented to an ophthalmic emergency department with progressive visual impairment which occurred during the previous 48 hours, accompanied by edema of the distal parts of the upper and lower limbs and basal crackles over the lungs. Intraocular pressure was normal (14 mm Hg). Pupils were wide and reactive. Optical coherence tomography of the macula and the optic disc was performed, showing the presence of subretinal fluid and papilledema. On fundus examination, whitish, sharply demarcated irregular foci were observed within the disc and the nasal part of the macula, surrounded by numerous flame‑shaped hemorrhages indicating Purtscher‑like retinopathy (PLR; Figure 1A and 1B). Noncontrast brain computed tomography (CT) was performed, not showing any significant lesions. The patient was urgently transferred to an internal medicine department for further investigation. On admission, her blood pressure was 119/70 mm Hg. Laboratory test results showed an elevated level of lactate dehydrogenase (>1400 U/l, reference range [RR], 135–214 U/l) and the presence of schistocytes on a manual peripheral blood smear (Figure 1C). Additionally, a reduction in platelet count (128 G/l [RR, 150–400 G/l]) and hemoglobin level (5.9 mmol/l [RR, 7.7–10 mmol/l]) was observed. Initially, the creatinine level was normal at 0.86 mg/dl (RR, 0.5–0.9 mg/dl). The following day, a rapid increase of the creatinine level, up to 1.5 mg/dl, and a drop in the platelet count to 72 G/l were observed. At this point, a diagnosis of acute kidney injury and thrombotic microangiopathy was established. Additionally, albuminuria with an albumin‑to‑creatinine ratio of 2225 mg/g (RR <30 mg/g) and the haptoglobin level below 0.1 g/l (RR, 0.3–2 g/l) were observed. A blood sample was sent for a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS13) assay, and a direct antiglobulin test was ordered with the suspicion of thrombotic thrombocytopenic purpura (TTP). The patient’s plasmic score was 6 at that time. Therapeutic plasma exchange was initiated on the third day of hospital stay, along with high‑dose intravenous methylprednisolone pulses. As ADAMTS‑13 activity was estimated at 24.5% (RR, 40%–130%), TTP was ruled out. Typical hemolytic uremic syndrome was also excluded, as testing for Shiga toxin–producing Escherichia coli via stool polymerase chain reaction turned out negative. The overall clinical presentation was indicative of atypical hemolytic uremic syndrome, and anti‑C5 therapy was initiated on day 8, with eculizumab at a single dose of 900 mg. The same day, however, the patient experienced recurrent seizure episodes accompanied by progressive respiratory failure and hypertensive crisis (blood pressure of 200/130 mm Hg). Urgent contrast‑enhanced brain CT was performed, showing subarachnoid hemorrhage and a ruptured aneurysmal protrusion up to 2.5 mm in diameter in the inferior wall of the anterior communicating artery (Figure 1D–1F). Given her critical condition, the patient was transferred to an intensive care unit. Due to severe coagulation disorders, neurosurgical treatment was abandoned. Brain angiography performed 2 days later showed no intracranial circulation, and the patient died shortly after.
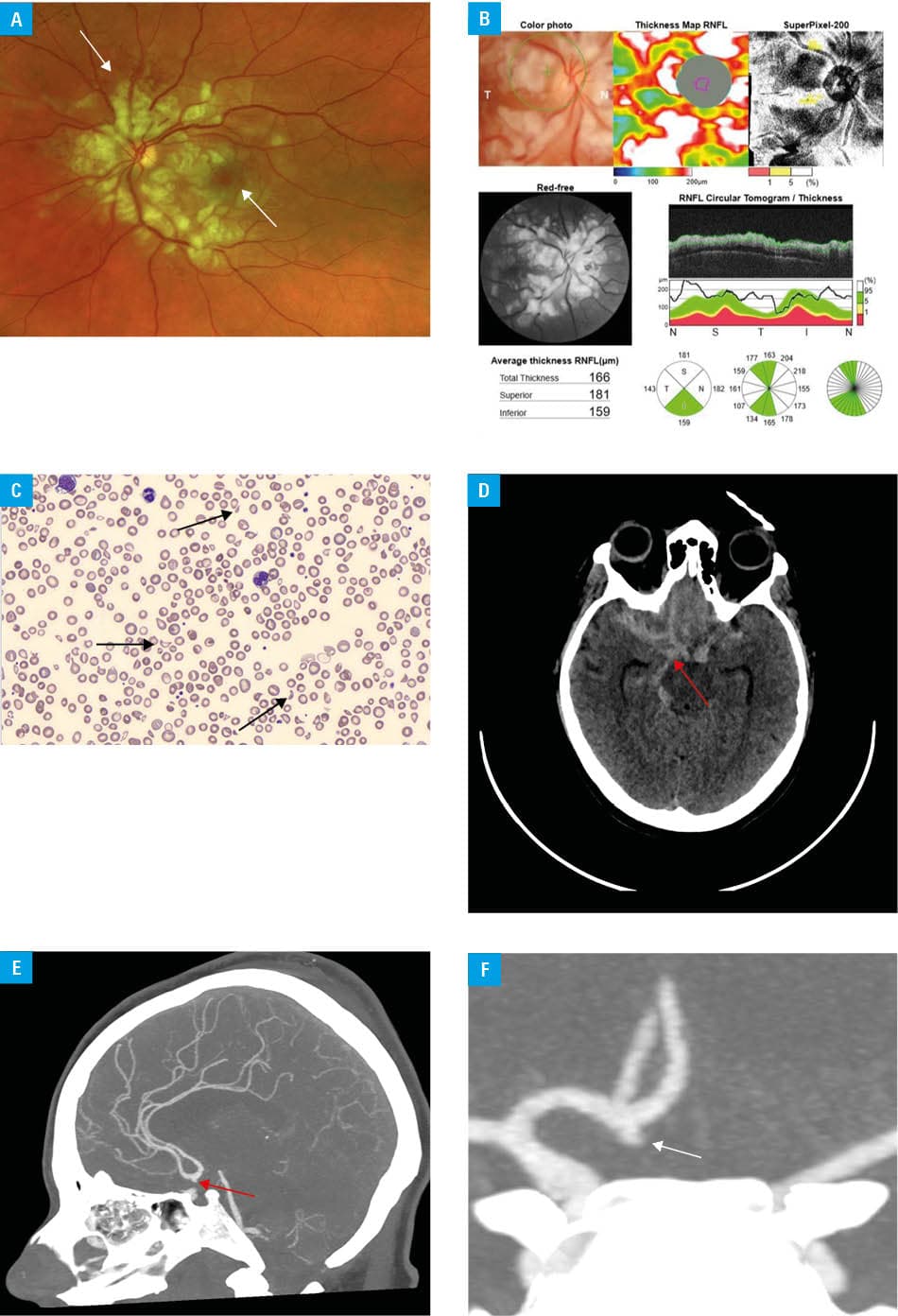
Abbreviations: RNFL, retinal nerve fiber layer
Both atypical hemolytic uremic syndrome and PLR are rare disorders.1 A prompt and accurate diagnosis is crucial in the management of patients with PLR, and central nervous system imaging should be performed urgently due to the potentially life‑threatening nature of a possible underlying condition.2 Symptoms, such as sudden visual loss, elevated renal function parameters, peripheral edema, hemolytic anemia, and thrombocytopenia—particularly in young individuals—should prompt an in‑depth diagnostic workup for thrombotic microangiopathies, such as atypical hemolytic uremic syndrome or TTP.3 The differential diagnosis should also include branch or central retinal artery occlusion, hypertensive retinopathy, diabetic retinopathy, and HIV retinopathy with cotton‑wool spots.4
- Gange WS, Haghighi A, Toy BC. Purtscher‑like retinopathy associated with atypical hemolytic uremic syndrome: case report and review of outcomes. Retin Cases Brief Rep. 2023; 17: 154‑159. | Crossref
- Ustaoğlu M, Önder F, Solmaz N, et al. Purtscher‑like retinopathy associated with atypical hemolytic uremic syndrome. Turk J Ophthalmol. 2017; 47: 348‑350. | Crossref
- Holak H, Holak N, Huzarska M, et al. Pathogenesis of Purtscher’s retinopathy and Purtscher‑like retinopathy. Klin Oczna. 2007; 109: 38‑45. | Crossref
- Agrawal A, McKibbin MA. Purtscher’s and Purtscher‑like retinopathies: a review. Surv Ophthalmol. 2006; 51: 129‑136. | Crossref
ARTICLE INFORMATION