Distress in patients with luminal advanced breast cancer receiving first-line endocrine therapy and CDK4/6 inhibitors: the first analysis from a university-affiliated cancer center in Poland
1,2 , 3, 4
, 3, 4

 CC BY 4.0
CC BY 4.0
Distress in patients with luminal advanced breast cancer receiving first-line endocrine therapy and CDK4/6 inhibitors: the first analysis from a university-affiliated cancer center in Poland
Introduction
Breast cancer (BC) is one of the most frequently diagnosed cancer in Poland.1 Combination treatment with endocrine therapy (ET) and a cyclin‑dependent kinase 4/6 inhibitor (CDK4/6i) significantly improves prognosis in patients with hormone receptor–positive (HR+) / human epidermal growth factor receptor 2–negative (HER2–) advanced BC (ABC), and represents the standard first‑line systemic therapy.2 ET‑CDK4/6i reimbursement began in Poland in September 2019, improving outcomes in HR+/HER2– ABC.3,4
In the course of incurable chronic cancer, beyond prolonging progression‑free and overall survival, health‑related quality of life (HRQoL) becomes an equally important parameter in treatment effectiveness. HRQoL may be significantly affected by distress.5 In oncology, distress broadly refers to emotional, psychological, social, or spiritual suffering related to the cancer diagnosis, treatment, or living with the disease. While distress is a natural reaction, it may warrant specialized support if it substantially interferes with cancer treatment and everyday life. Screening, monitoring, and managing distress have been recommended by the National Comprehensive Cancer Network (NCCN) for over 25 years in all patients diagnosed with cancer.6 If a patient distress score is moderate or high (≥4 on the Distress Thermometer, which is a visual analog scale ranging from 0 to 10), additional evaluation is performed, followed by suitable interventions, such as psychosocial support, counseling, or referral to a psychiatrist.7 Distress affects patient HRQoL, symptoms, and outcomes, and occurs in over 60% of individuals with ABC.8 Although clinical studies on CDK4/6i treatment often assess HRQoL, they usually do not measure distress specifically, leading to limited data on this aspect.9 Real‑world data on distress in CDK4/6i‑treated patients are scarce, especially in Poland, where this factor is not routinely assessed, and no prior study has explored emotional burden in HR+/HER2– ABC patients receiving first‑line therapy in standard care.
This study addresses this gap by providing the first real‑world data from Poland on distress levels and associated problem areas in HR+/HER2– ABC patients receiving first‑line treatment with ET‑CDK4/6i. It offers unique insights into distress in a defined health care setting and treatment phase, under routine conditions. Understanding these challenges can inform systemic improvements in supportive care in Poland and other countries with a similar health care system.
Patients and methods
Study design and patients
This exploratory study used a cohort survey design. It was registered at the Open Science Framework on January 29, 2023 (protocol available at https://doi.org/10.17605/OSF.IO/V6HRJ). Approval to use distress screening tools was granted by the NCCN (request ID, 44321; January 4, 2023). The distress thermometer and problem list had been validated for Poland and are reliable for assessing distress in Polish cancer patients.10
Between January 2023 and February 2024, a total of 115 women diagnosed with HR+/HER2– ABC receiving first‑line treatment with ET‑CDK4/6i participated in the survey. The patients completed the Polish version (2.2022) of the NCCN distress tool during their routine visit—either within their first month of therapy or at the next follow‑up (for those already treated)—without assistance from medical personnel. Sociodemographic data (age, level of education, employment and marital statuses) were anonymously collected. Clinical information, including menopausal status, Eastern Cooperative Oncology Group performance status (ECOG PS), germline mutation status, comorbidities, medications, date of BC diagnosis, metastatic status (de novo vs recurrence), metastatic locations, time since diagnosis, and specifics of ET‑CDK4/6i treatment, were provided by the treating physicians.
Patients were excluded if they had early‑stage BC, triple‑negative or HER2+ ABC, HR+/HER2– ABC not treated with a CDK4/6i, or had received more than 1 line of palliative systemic therapy.
The survey included patient‑reported questions assessing physician‑initiated discussions about distress at the beginning and throughout treatment.
The primary objective was to describe distress levels in patients with HR+/HER2– ABC receiving first‑line treatment with ET‑CDK4/6i. Secondary objectives were to evaluate the level of distress by therapy duration, describe its domains, assess distress management practices adopted by physicians, and analyze associations between distress levels and sociodemographic and clinical factors, including time since diagnosis and completion of radical treatment.
Ethics
The study was approved by the Ethical Committee of the Wroclaw Medical University (66/2023) and conducted in accordance with institutional standards and the 1964 Helsinki Declaration. Written informed consent was obtained from all participants.
Statistical analysis
Statistical analysis was performed using the R 4.4.1 package (R Foundation for Statistical Computing, Vienna, Austria).11 Distress domain scores were calculated by unitizing the sum of complaints per domain (min = 0). For each variable, the mean, SD, median, and range were calculated. Normality of data distribution (distress levels and domain scores) was tested using the Shapiro–Wilk test. Due to non‑normal distribution, nonparametric tests were applied. Spearman rank correlations between distress levels, age, time since diagnosis, time since radical treatment, number of comedications, and comorbidities were assessed using the “psych” library.12
Differences related to menopausal status, metastatic lesion location (bone vs other), medication use, comorbidities, recurrence, and genetic mutations were compared using the Mann–Whitney test. Effects of the ECOG PS and type of CDK4/6i were analyzed with the Kruskal–Wallis tests, followed by the Dunn post hoc analysis. Symptom intensity across domains was compared using the Friedman test, followed by pairwise Wilcoxon tests with false discovery rate corrections. Effect sizes were calculated,13 with the following thresholds: Mann–Whitney / Friedman, small below 0.3; moderate, 0.3–0.5; large above 0.5; Kruskal–Wallis, small below 0.06; moderate, 0.06–0.14; large above 0.14. This part of the analysis was performed using the “rstatix” library.14
All statistical inference was conducted at a significance level of P = 0.05.
Results
Patient characteristics
A total of 115 women diagnosed with HR+/HER2– ABC participated in this noninterventional study. All patients were of European descent, and their median age was 64 years (range, 31–86 y). Most participants were postmenopausal (80.9%). The proportion of patients with de novo and recurrent metastatic disease was balanced (53.9% vs 46.1%). Common metastatic sites included multiple locations (47.8%) and bones (39.1%). Aromatase inhibitors (AIs) were used in 82.6% of the patients, while 17.4% received fulvestrant. Ribociclib was the most frequently used CDK4/6i (64.4%), followed by abemaciclib (19.1%) and palbociclib (16.5%). Mean treatment duration was 15.7 months (median, 9). Most patients had a secondary level of education (60.9%), were married (57.9%), and retired (63.2%).
Distress and its domains
The mean (SD) distress level was 3.07 (2.58), with a median of 3 on a scale from 0 to 10, indicating moderate emotional burden. Distress levels were associated with treatment duration, although the differences were not significant (r = 0.021; P = 0.18). The highest distress levels were observed in the patients treated for up to 1 month (median [range], 3.5 [0–8] and more than 12 months (median [range], 3 [0–10]), and the lowest in those treated for 2–3 months (median [range], 1 [0–6]; Figure 1A).
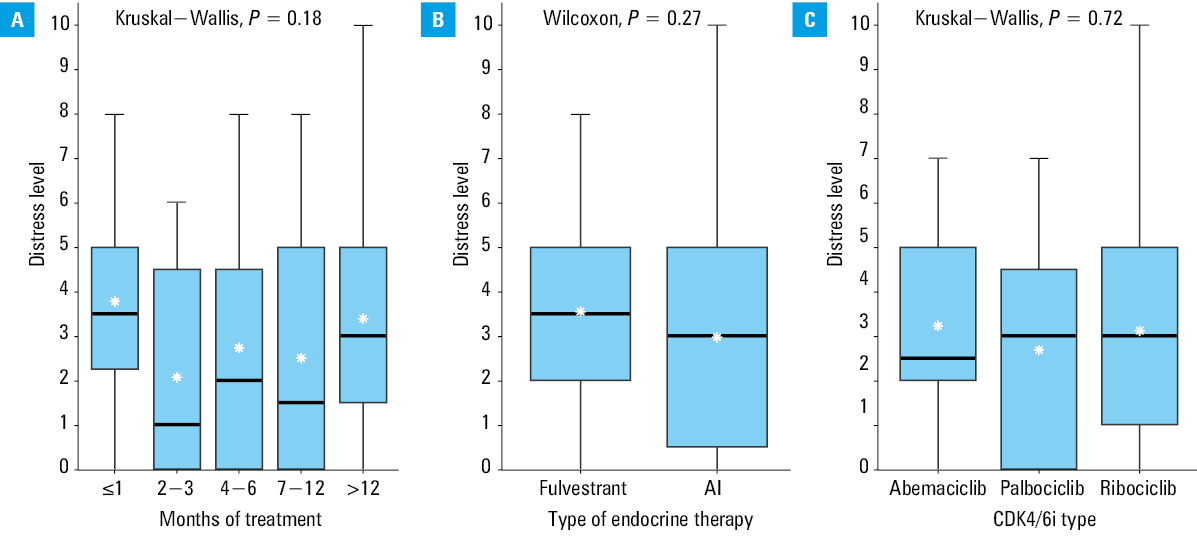
Abbreviations: AI, aromatase inhibitor; CDK4/6i, cyclin‑dependent kinase 4/6 inhibitor
The most common physical issues reported by the patients were fatigue (49.6%), pain (35.7%), and loss or changes in physical abilities (34%). Prevalence of fatigue was notably higher in the women with recurrent disease (60.4%), as compared with newly diagnosed metastatic cases (40.3%), although the difference was marginally nonsignificant (P = 0.050). The least common issues related to physical health included sexual health concerns (5.2%), tobacco use (2.6%), and substance use (0%).
Emotional problems frequently included worry / anxiety (49.6%), fear (24.4%), and anger (15.7%). Sadness / depression (13%) and feeling worthless or burdensome (7.8%) were less common. Social issues were rare, primarily concerning relationships with the family (13%) and friends / coworkers (8.7%). Problems communicating with health care providers (4.4%) and fertility concerns (2.6%) were infrequent. Practical difficulties mostly related to self‑care (25.2%) and treatment decisions (23.5%), with issues concerning housing (8.7%), work (7%), and child care (4.4%) reported less frequently. Spiritual concerns were uncommon, and predominantly involved finding meaning / purpose (14.8%) and thinking about death / dying / afterlife (13%).
Physical difficulties peaked in the first month of treatment, with a decline observed thereafter, and a slight increase after 12 months. Emotional difficulties also peaked initially, reaching their lowest point between 7 and 12 months. Social and practical issues were the most commonly reported at 4–6 months, and the least often after 12 months of treatment. Spiritual distress was the greatest initially and the lowest at 7–12 months.
Distress and patient concerns by de novo or recurrent status
In an exploratory analysis, the patients with recurrent cancer reported higher levels of distress (median [range], 3 [2–9]) than the newly diagnosed individuals (median [range], 2 [0–10]; r = 0.16; P = 0.046). Recurrent disease was associated with a greater level of physical concern than a de novo diagnosis (median [range], 33.33 [0–83.33] vs 16.67 [0–100], respectively; r = 0.18; P = 0.03) and a difference in the distribution of emotional concerns (r = 0.17; P = 0.03). Fatigue was notably higher in the recurrence group (60.4% vs 40.3%; P = 0.05). Social and practical concerns were marginally higher in the recurrence group (r = 0.05; P = 0.62 and r = 0.06; P = 0.52, respectively). Spiritual concerns were slightly more common among the newly diagnosed patients (r = 0.03; P = 0.73). These findings were not adjusted for potential confounding factors and should be interpreted with caution.
Physical issues dominated distress in both groups. The newly diagnosed patients emphasized emotional and spiritual concerns over social / practical issues, whereas the individuals with recurrent disease emphasized emotional and practical concerns rather than physical issues. Anxiety and depression were significant emotional issues in the recurrence group.
Patient distress and concerns across therapy types
An exploratory comparison of therapy types showed that the patients receiving fulvestrant had a slightly higher level of distress as compared with the AI recipients (median [range], 3.5 [0–8] vs 3 [0–10]; r = 0.1; P = 0.27; Figure 1B), whereas the AI‑treated patients had greater social concerns (r = 0.18; P = 0.03). Physical and emotional issues consistently prevailed regardless of ET type, while social / spiritual concerns were the lowest in the fulvestrant‑treated patients. These subgroup analyses were unadjusted for confounding variables and should be interpreted as exploratory findings.
Median (range) distress level was comparable across the CDK4/6i types (ribociclib, 3 [0–10]; palbociclib, 3 [0–7]; and abemaciclib, 2.5 [0–7]; r = –0.01; P = 0.72; Figure 1C). Physical and emotional problems consistently predominated, practical issues were reported less often, and social / spiritual concerns were the least impactful across CDK4/6i subgroups. Again, these results were not adjusted for confounding factors and should be viewed as exploratory.
Associations of distress, social factors, and clinical variables
Time since diagnosis significantly but weakly correlated with emotional concerns (R = 0.26) and overall distress (R = 0.24). The distress level was nonsignificantly higher in the patients treated radically for local recurrence, as compared with the nonrecurrent cases (median [range], 5 [1–8] vs 3 [0–10], respectively; r = 0.01; P = 0.22). The patients with ductal carcinoma reported greater physical concerns (R = 0.18; r = 0.18; P = 0.03). Age, menopausal status, metastasis location, ECOG PS, comorbidities, medication use, recurrence during adjuvant therapy, and genetic mutations did not significantly influence overall distress, although predisposing genetic mutations were associated with a higher level of physical concerns (R = 0.23; r = 0.23; P = 0.03). Physical and emotional distress consistently dominated across clinical factors, with minimal influence from social factors.
Internal practice of distress evaluation in patient care
Initially, 66.7% of the participants reported discussing distress with their doctors, and this rate decreased slightly during treatment (62.6%). Recommendations for mental health support were limited and comprised psychiatry referrals (27%) and psychological consultations (37.4%). Only 5.2% of the participants had prior mental health diagnoses, and 7.8% took psychiatric medications, suggesting a low prevalence of pre‑existing mental health issues.
Discussion
To our best knowledge, this is the first study to evaluate distress in HR+/HER2– ABC patients receiving ET‑CDK4/6i as their first‑line treatment, and the results may contribute to improving holistic patient care.
The International Psycho‑Oncology Society recognizes distress as the sixth vital sign, emphasizing that its assessment should be an integral part of routine clinical practice. Regular evaluation can help provide appropriate support of patient needs and improve HRQoL.15 This study aligns with psycho‑oncology frameworks by emphasizing the temporal variability of distress, which offers clinically relevant insights for supportive care planning.
Although distress assessment is not yet routine among clinical oncologists in Poland, in the analyzed cohort of women treated at the Breast Unit (BU) of the Lower Silesian Oncology Center, the median distress level across all time points was relatively low (below 4). This finding should be interpreted cautiously, as cultural factors, such as underreporting, emotional inhibition, or stigma surrounding psychological symptoms may have contributed to the observed low scores. While access to psychological care and treatment in an organized BU may support emotional wellbeing, claims about their protective effect remain speculative and require further research. Moreover, our study showed that some patients were actively informed about the consultation options, underscoring the importance of psychological support in organized BUs.16
Distress ranges from normal emotions, such as worry, anxiety, and sadness, to serious clinical conditions, including anxiety disorders or depression.15 This was confirmed in our study, as the patients frequently reported worry, anxiety, and fear. The greatest emotional and spiritual difficulties occurred in the first month of treatment, showing how challenging it is to cope initially with an ABC diagnosis. Over time, the level of distress decreased, reaching the lowest point between 7 and 12 months since the treatment initiation, suggesting patients gradually adapted psychologically. After 12 months, physical difficulties slightly increased, possibly due to disease progression or side effects of treatment. These findings reflect the expected progression of psychological adjustment over time and reinforce the need for ongoing emotional support throughout the disease course.
The observed changes in distress align with the model of coping proposed by Kübler‑Ross and Byock.17 Emotional and spiritual struggles were the greatest immediately after diagnosis, reflecting the stages of denial and anger. Over the next few months, the patients appeared to move toward acceptance, as reflected by lower distress levels at 2–3 months. Physical symptoms were also the most severe early on, probably because treatment‑related symptom management was not effective yet. This highlights the importance of integrating early supportive and palliative care interventions at the time of metastatic cancer diagnosis, regardless of patient prognosis.18 However, the clinical response to identified distress was not assessed, limiting conclusions on intervention outcomes.
HRQoL data for patients receiving ET‑CDK4/6i based on other HRQoL assessment tools indicate that patients report lower levels of pain, fatigue, and improved physical and emotional functioning, as compared with the control group.9 Our findings complement these data by showing that, despite the use of CDK4/6i, the symptoms experienced remained a significant clinical issue. As reported in the literature, fatigue continues to be the most common symptom experienced during cancer treatment.6,19
The median distress levels were comparable across the 3 CDK4/6i analyzed, with no significant differences observed. The effect size was negligible, suggesting that the type of CDK4/6i did not substantially influence the distress levels. Although slight pharmacological and survival‑related differences exist between agents, such distinctions are more likely understood by clinicians than patients.20 Thus, it is reasonable to hypothesize—but not conclude—that the specific choice of CDK4/6i does not contribute to differential psychological distress. Moreover, differences in toxicity profiles did not seem to contribute to psychological distress in this population.
A slightly higher distress level was noted in the patients treated with fulvestrant, as compared with those receiving AIs. Notably, significant differences were found with respect to social concerns, which were more pronounced in the patients on AIs. This pattern reflects the clinical rationale behind the selection of ET. Fulvestrant is typically prescribed for patients who have experienced disease progression on AIs, indicating prior treatment failure and potential hormone resistance.21,22 Therefore, the observed distress in this group may relate more to the emotional impact of the treatment history and disease progression rather than to the agent itself—an interpretation that remains exploratory.
Patients with newly‑diagnosed HR+/HER2– ABC have a better prognosis than those who experience recurrence after radical treatment.20 A notable finding of our study is that the patients with recurrent metastatic disease experienced higher distress levels than those with de novo metastatic disease, likely due to prior treatments and associated challenges. Emotional concerns were more prevalent in the recurrence group, highlighting the psychological burden of disease recurrence. These findings further support the need for individualized psychosocial interventions, particularly in patients with a history of prior cancer therapy.
Limitations
The main limitations of our study are a small sample, single‑center design, and single‑time distress assessment, which precludes evaluating changes over time. Its cross‑sectional nature limits conclusions about causality or temporal trends. While some patterns emerged based on time since treatment initiation, the lack of repeated, standardized assessments prevents us from drawing firm conclusions on distress evolution. Variation in the timing of assessment introduced heterogeneity that may have influenced the results. The study also did not evaluate clinical responses to identified distress, leaving the practical impact of screening unclear. Nonetheless, to our best knowledge, this is the first detailed report on distress in Polish women receiving first‑line treatment with ET‑CDK4/6i. It also offers valuable insights into their HRQoL, which is a research area with scarce data.
Conclusions
The highest levels of distress were noted in the patients treated for less than 1 month and more than 12 months. Physical and emotional challenges dominated across all groups, regardless of clinical characteristics or type of therapy. Social, practical, and spiritual problems were less pronounced, though their intensity varied depending on the treatment type and duration. The key determinant of the distress levels was cancer recurrence following radical treatment. The study shows that distress affects patients with ABC in many ways, highlighting the need for personalized support depending on the duration of the first‑line systemic treatment. Our findings emphasize the need for routine distress assessment in clinical oncology practice and underscore the importance of comprehensive psychological and supportive care throughout the course of treatment.
- Didkowska JA, Barańska K, Miklewska MJ, Wojciechowska U. Cancer incidence and mortality in Poland in 2023. Nowotwory. 2024; 74: 75‑93. | Crossref
- Cardoso F, Paluch‑Shimon S, Schumacher‑Wulf E, et al. 6th and 7th International Consensus Guidelines for the management of advanced breast cancer (ABC guidelines 6 and 7). Breast. 2024; 76: 103756. | Crossref
- Duchnowska R, Soter K, Smok‑Kalwat J, et al. Real‑world treatment outcomes in patients with HR+ HER2- advanced breast cancer treated with CDK4/6 inhibitors and endocrine therapy. J Clin Oncol. 2024; 42: 1067. | Crossref
- Ziobro M, Grela‑Wojewoda A. Shifting treatment paradigms: improvements in HR‑positive, HER2‑negative breast cancer care in Poland from a clinical perspective. Biomedicine. 2023; 11: 510. | Crossref
- Velickovic K, Olsson Möller U, Ryden L, et al. Model of health‑related quality of life in breast cancer patients using cross‑sectional data: the role of resilience. Cancer Manag Res. 2024; 16: 1545‑1555. | Crossref
ARTICLE INFORMATION