Clinical characteristics of patients with primary biliary cholangitis treated with ursodeoxycholic acid
Key words: cholestasis, cirrhosis, primary biliary cholangitis, pruritus, ursodeoxycholic acid

 CC BY 4.0
CC BY 4.0
Clinical characteristics of patients with primary biliary cholangitis treated with ursodeoxycholic acid
Introduction: Primary biliary cholangitis (PBC) is a chronic autoimmune cholestatic liver disease. Despite established first‑line therapy with ursodeoxycholic acid (UDCA), many patients do not achieve biochemical remission. Data on the characteristics of PBC in Poland remain limited.
Objectives: The aim of this study was to characterize demographic, clinical, and serological features of Polish patients with PBC and the effects of treatment in a multicenter retrospective cohort.
Patients and methods: A total of 364 patients from 10 hepatology centers were included. Data on demographics, laboratory tests, autoantibodies, and markers of the disease severity were collected between January 6 and March 8, 2025 and analyzed according to the duration of UDCA treatment (<2 vs ≥2 years).
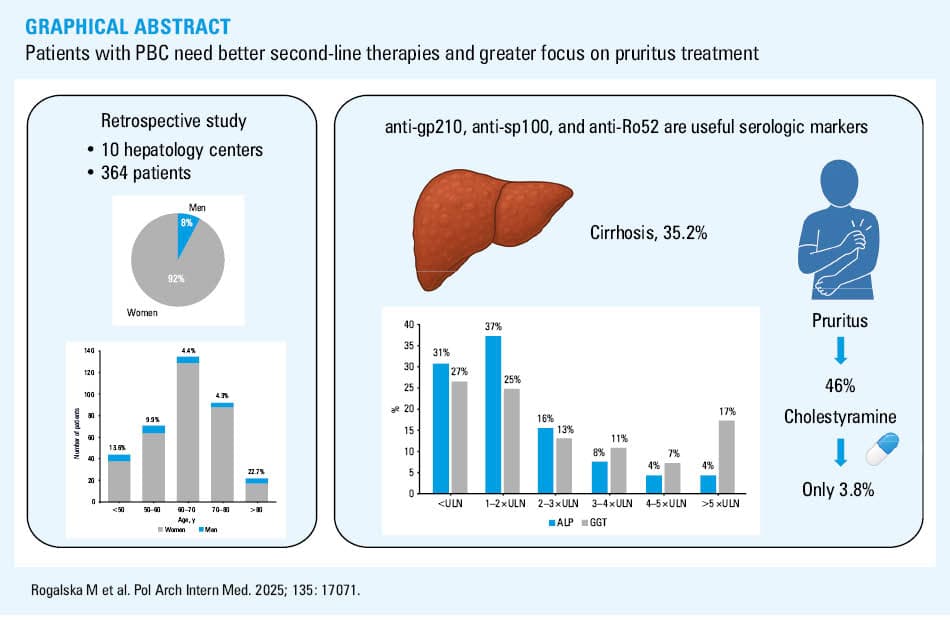
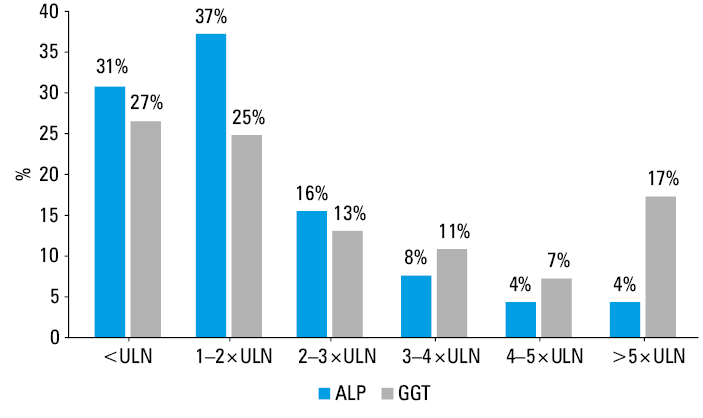
Results: Women constituted 92.3% of the cohort. Most patients were aged 60–80 years, but the proportion of men was relatively higher in the groups below 50 and over 80 years old. Cirrhosis was diagnosed in 35.2% of the patients. Antimitochondrial antibodies were present in 94.4%, and anti‑Ro52 antibodies in 34.1% of the study participants. Anti‑gp210 and anti‑sp100 antibodies were more frequent in the patients with longer disease duration. No substantial differences in liver biochemistry were found between short- and long‑term UDCA use groups, except for lower γ-glutamyl transferase activity with longer treatment. Despite pruritus found in 46% of the patients, antipruritic therapy was rarely used.
Conclusions: This is the first national study to characterize PBC in Poland. Its findings suggest limited long‑term efficacy of UDCA and unmet needs in symptom management. Anti‑gp210, anti‑sp100, and anti‑Ro52 antibodies may serve as important serologic markers. Prospective studies are needed to confirm these observations.
What's new?
This retrospective multicenter study provides the first demographic and clinical insights into the Polish population with primary biliary cholangitis (PBC), offering context for future research and clinical practice. We found that anti‑gp210 and anti‑sp100 antibodies were more frequently detected in patients with longer disease duration, which requires further analysis in a prospective study. Additionally, high prevalence of anti‑Ro52 antibodies supports a growing evidence of their specificity for PBC. Despite pruritus being a hallmark symptom of PBC, the use of antipruritic medications was low, indicating possible underrecognition or undertreatment. Finally, our findings suggest that prolonged first‑line ursodeoxycholic acid therapy does not substantially improve laboratory parameters or prevent the disease progression, underscoring the need for more effective treatment strategies.
Introduction
Primary biliary cholangitis (PBC) is an uncommon, chronic, cholestatic liver disease characterized by progressive immune‑mediated destruction of interlobular and septal bile ducts, potentially leading to cirrhosis.1 Although initial descriptions of the disease come from the 19th century, it was first reported and named primary biliary cirrhosis by Ahrens et al2 in 1950. The nomenclature was subsequently changed to the current one in 2015 to better reflect the wider nature of the disease.3 The condition shows a marked female predominance, especially among patients aged 40–60 years, and it is estimated that approximately 1 in every 1000 women aged over 40 years suffers from PBC.4 The pathogenesis of PBC remains unclear but the disease seems to be initiated by a combination of a susceptible genetic background and exposure to environmental triggers.5 The hallmark serologic feature of PBC is the presence of M2 subtype of antimitochondrial antibodies (AMA‑M2), which target the E2 subunit of the pyruvate dehydrogenase complex (PDC‑E2) in the biliary epithelial cells.6 In the AMA‑negative form of the disease, diagnosis can be supported by the presence of specific antinuclear antibodies, such as sp100 and gp210, which are associated with more aggressive disease and worse outcomes.7 Elevated activity of alkaline phosphatase (ALP) is a key biochemical marker of cholestasis and, along with bilirubin concentration, reflects the disease severity and progression.8 PBC typically presents asymptomatically in the early stages. However, as the disease progresses, pruritus and fatigue are among the most frequently reported symptoms.9 So far, the first‑line pharmacological therapy has been ursodeoxycholic acid (UDCA), which unfortunately has not prevented progression to cirrhosis or reduced the severity of disease‑related symptoms, especially pruritus, which significantly impairs patient quality of life.10,11 The results of research on drugs from the group of peroxisome proliferator‑activated receptor (PPAR) agonists offer hope for changing this situation.12
Given the lack of comprehensive data on the demographic and clinical characteristics of patients with PBC in the Polish population, we conducted a retrospective, multicenter analysis of records from 10 specialized hepatology centers to provide a characterization of this patient group and to establish a foundation for future prospective studies, which is particularly important due to the genetic determinants of PBC, which create the possibility of ethnic and geographical differences in the course of the disease.
Patients and methods
Between January 6 and March 8, 2025, a total of 367 patients diagnosed with PBC were reported to the BilTer database by 10 Polish hepatology centers. The BilTer database is a retrospective, investigator‑initiated multicenter database collecting real‑world data from hepatology centers in Poland, which was started after approval of the Bioethics Committee of the Medical University of Białystok (APK.002.30.2025). Of the patients registered in the database, 3 were not treated with UDCA, therefore, in order to ensure homogeneity of the study group, they were excluded from further analysis, and 364 patients undergoing UDCA treatment were included in the study. The diagnosis of PBC was made according to the European Association for the Study of the Liver (EASL) criteria, which require elevated ALP activity and the presence of AMAs, or—if AMAs are undetectable—the presence of anti‑sp100 or anti‑gp210 antibodies, with exclusion of other causes of liver disease.13 The diagnosis of cirrhosis was established based on a typical clinical presentation and either histological examination of liver biopsy specimens and transient elastography showing liver stiffness above 17 kPa, or noninvasive laboratory indices, such as the aspartate aminotransferase‑to‑platelet ratio index (APRI) above 1.5 and fibrosis‑4 (FIB‑4) index above 3.25. The study included demographic, clinical, laboratory, and imaging parameters available from the patient most recent clinical visit. A decision on the type of treatment was made by an attending physician based on current recommendations and availability of drugs.
Statistical analysis
Continuous variables were presented as median and interquartile range (IQR). Normality of distribution was assessed using the Shapiro–Wilk test. Since most variables did not follow a normal distribution, comparisons between the groups (UDCA treatment duration <2 years vs UDCA ≥2 years) were performed with the nonparametric Mann–Whitney test. Categorical variables were presented as counts and percentages. Associations between the categorical variables and UDCA treatment duration were tested with the χ2 test. When the expected cell counts were below 5, the Fisher exact test was used instead. Statistical significance was determined based on P values, with a threshold of P below 0.05. All statistical analyses were performed using TIBCO Statistica package, version 14 (Tibco Software Inc., Palo Alto, California, United States), which is a standard statistical software provided and supported by the Medical University of Bialystok. The package includes a dedicated medical statistics module, commonly used in clinical and hepatology research within our institution.
Results
Of the 364 patients registered in the study, over 92% were women (Table 1), and 110 patients (30%) had their last visit within the past 3 months. The predominant age group consisted of individuals aged 60–80 years (63%), and median (IQR) age of the entire cohort was 66 (57–72) years. Notably, 12% of the patients were younger than 50 years, and the percentage of men in this subgroup (13.6%)—as well as in the oldest age group (>80 years; 22.7%)—was higher (P = 0.008), as compared with the dominant 50–80‑year‑old group (5.7%; Figure 1).
Variable | All patients | UDCA <2 years | UDCA ≥2 years | P value |
Abbreviations: APRI, aspartate aminotransferase‑to‑platelet ratio index; FIB‑4, fibrosis‑4 index; IQR, interquartile range; n, number of patients in a specific category; N, total number of patients; UDCA, ursodeoxycholic acid | ||||
Women, n/N (%) | 336/364 (92.3) | 80/92 (87) | 256/272 (94.1) | 0.04 |
Age, y, median (IQR) | 66 (57–72) | 62 (53.5–69) | 67 (60–73) | 0.001 |
Pruritus, n/N (%) | 148/325 (45.5) | 40/84 (47.6) | 108/241 (44.8) | 0.7 |
Child–Pugh score in cirrhotics, n/N (%) | A, 96/128 (75); B, 21/128 (16.4); C, 11/128 (8.6) | A, 22/26 (84.6); B, 4/26 (15.4); C, 0 | A, 74/102 (72.6); B, 17/102 (16.7); C, 11/102 (10.8) | 0.07 |
Liver transplant history, n/N (%) | 7/364 (1.9) | 1/92 (1.1) | 6/272 (2.2) | 0.68 |
Dilated portal vein on ultrasound, n/N (%) | 61/364 (16.8) | 9/92 (9.8) | 52/272 (19.1) | 0.05 |
Splenomegaly on ultrasound, n/N (%) | 106/364 (29.1) | 22/92 (23.9) | 84/272 (30.9) | 0.18 |
Elastography, kPa, median (IQR) | 8.5 (6–16.4) | 7.9 (5–17.3) | 8.6 (6.2–16.1) | 0.38 |
APRI, median (IQR) | 0.55 (0.35–1.2) | 0.5 (0.34–1.09) | 0.57 (0.36–1.25) | 0.39 |
FIB‑4, median (IQR) | 2.12 (1.3–4.11) | 1.74 (1.14–3.28) | 2.22 (1.34–4.38) | 0.04 |
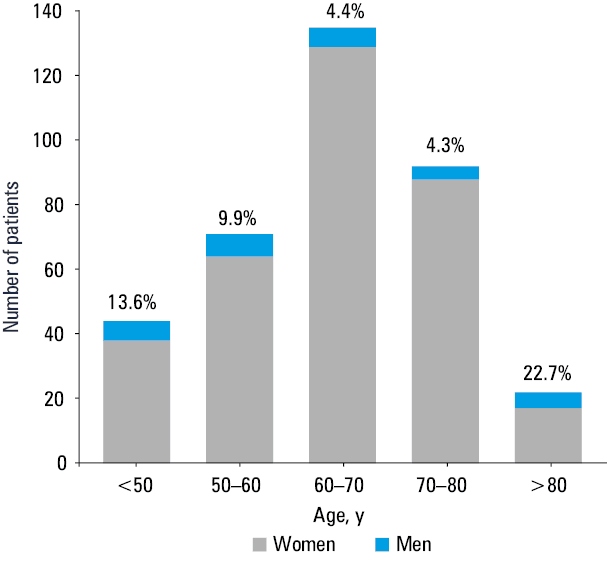
At the time of the last visit, pruritus was reported by 46% of the patients. Among the 104 individuals with prior liver biopsy, histological examination confirmed features of cirrhosis in 20 cases (19%). In the 230 patients with available elastographic examination, liver tissue stiffness exceeding 17 kPa was noted in 54 participants (23.5%). APRI values exceeding 1.5 were found in 57 of 343 patients (16.6%), while FIB‑4 values greater than 3.25 were observed in 115 of 340 patients (33.9%). Median (IQR) values for these parameters are presented in Table 1. Ultimately, cirrhosis was diagnosed in 128 patients (35.2%), of whom 32 (25%) were classified as Child–Pugh class B or C (Table 1). At the last visit, 31% and 27% of patients had ALP and g‑glutamyl transferase (GGT) activity within the normal range, respectively, while in 32% and 48% of the patients, respectively, the levels of these enzymes were at least twice above the upper limit of normal (ULN; Figure 2). Median (IQR) values for laboratory liver function parameters are presented in Table 2. The characteristic autoantibody AMA‑M2 was detected in 94.4%, and AMA‑M2‑3E in 75.3% of the patients. Much lower percentages, from 6.2% to 34.1%, were noted when testing for other autoantibodies associated with the disease (Table 3).
Variable | All patients | UDCA <2 years | UDCA ≥2 years | P value |
Data are presented as median and interquartile range.
SI conversion factors: to convert albumin to g/l, multiply by 10; ALP, ALT, AST, an GGT to μkat/l, by 0.0167; bilirubin to μmol/l, by 17.104
Abbreviations: AFP, α fetoprotein; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, γ-glutamyl transferase; PLT, platelet count; PT, prothrombin time; others, see Table 1 | ||||
ALP, IU/l | 195 (121–339) | 200 (115–343) | 194 (123–338) | 0.92 |
GGT, IU/l | 79 (39–159.5) | 132 (43–254) | 72 (38–136) | 0.001 |
ALT, IU/l | 32 (22–51) | 37 (22–69) | 31.5 (21–51) | 0.1 |
AST, IU/l | 34 (26–54.5) | 33 (25–62) | 34 (26–54) | 0.91 |
Bilirubin, mg/dl | 0.67 (0.47–1.12) | 0.61 (0.45–1.04) | 0.71 (0.49–1.15) | 0.34 |
Albumin, g/dl | 3.95 (3.61–4.2) | 4.02 (3.63–4.3) | 3.93 (3.61–4.18) | 0.16 |
AFP, µg/l | 3.1 (2–4.91) | 2.81 (1.83–4.43) | 3.2 (2.03–5.2) | 0.17 |
PLT, × 10³/µl | 202 (129–261) | 208 (136.5–267.5) | 194 (126–255) | 0.28 |
PT, s | 11.9 (11–12.9) | 11.8 (10.9–12.7) | 11.9 (11.1–12.9) | 0.31 |
Variable | All patients | UDCA <2 years | UDCA ≥2 years | P value |
Abbreviations: anti‑LC1, anti‑liver cytosol type 1 antibody; AMA‑M2, antimitochondrial antibody M2; AMA‑M2‑3E, antimitochondrial antibody M2 subtype 3E; anti‑PML, antipromyelocytic leukemia protein antibody; others, see Table 1 | ||||
AMA‑M2, n/N (%) | 337/357 (94.4) | 88/91 (96.7) | 249/266 (93.6) | 0.43 |
AMA‑M2‑3E, n/N (%) | 110/146 (75.3) | 33/46 (71.7) | 77/100 (77) | 0.54 |
Anti‑gp210, n/N (%) | 35/137 (25.6) | 6/44 (13.6) | 29/93 (31.2) | 0.04 |
Anti‑sp100, n/N (%) | 36/137 (26.3) | 5/44 (11.4) | 31/93 (33.3) | 0.01 |
Anti‑LC‑1, n/N (%) | 9/146 (6.2) | 3/46 (6.5) | 6/100 (6) | >0.99 |
Anti‑PML, n/N (%) | 20/131 (15.3) | 6/44 (13.6) | 14/87 (16.1) | 0.8 |
Anti‑Ro52, n/N (%) | 45/132 (34.1) | 12/44 (27.3) | 33 (37.5) | 0.33 |
Regarding treatment, 32 patients (8.8%) received fenofibrate in addition to UDCA, 14 (3.8%) were treated with cholestyramine, and 2 (0.6%) received obeticholic acid. UDCA therapy had been administered for less than 2 years in 92 patients (25.3%), and for at least 2 years in 272 patients (74.7%). A comparison between these groups showed a significantly higher proportion of women and older patients in the group with longer treatment duration (Table 1).
As shown in Table 1, all analyzed indicators related to the advancement of the liver disease showed features of deterioration in the group treated with UDCA for at least 2 years, however, a significant difference was found only for FIB‑4 values. Laboratory indicators of liver damage and function presented in Table 2 did not differ between the 2 groups of patients, except for GGT activity, which was significantly lower in the patients treated with UDCA for more than 2 years. Among the analyzed autoantibodies, a significant increase in the frequency with longer treatment duration was observed only for anti‑gp210 and anti‑sp100 (Table 3).
Discussion
The prevalence and incidence of PBC show a considerable geographical variation.14,15 While no epidemiologic data are currently available for Poland, pooled global estimates suggest prevalence of 14.6 per 100 000 individuals, albeit with substantial heterogeneity across studies.14 In Europe, the estimated prevalence is higher, at 22.27 per 100 000 individuals.15 Interestingly, Gazda et al15 analyzed data from selected European countries, and concluded that countries from the former Eastern Bloc had significantly lower point‑prevalence rates than those from the former Western Bloc (estimate, –0.0071; 95% CI, –0.0127 to 0.0016; P <0.05). However, it is not known whether epidemiologic data from Poland will confirm this pattern. The pooled global incidence of PBC is 1.76 per 100 000 individuals per year, with a slightly higher annual incidence in Europe of 1.87 per 100 000.14,15 Both prevalence and incidence have demonstrated an upward trend in recent years.14,16,17 This may be partially attributed to improved diagnostic tools (eg, AMA testing), greater disease awareness among health care professionals, and enhanced survival due to advances in pharmacotherapy and liver transplantation. In addition, 2 main hypotheses have been proposed to explain a potential true increase in PBC incidence: the expansion of high‑risk populations and changes in environmental triggers.
In our study, the predominant age group consisted of patients aged 60–80 years, accounting for 63% of the study population. Among those treated for a longer time, a significantly higher proportion of women and older individuals was observed. This distribution aligns well with international data, which consistently report the highest prevalence of PBC among patients aged 60–80 years.14 Interestingly, we observed a significantly higher proportion of men in both the youngest (<50 years; 13.6%) and oldest (>80 years; 22.7%) age groups, as compared with the core population aged 50–80 years (5.7%). This bimodal overrepresentation of men in the youngest and oldest age groups warrants further exploration. One possible explanation is a cohort‑specific variation in diagnostic awareness and referral practices. Younger men may be more likely to undergo early diagnostic workup due to atypical presentations or concurrent autoimmune symptoms prompting further evaluation. Another contributing factor could be demographic characteristics unique to our national cohort, such as differences in health care access or comorbidity profiles across age and sex strata.
PBC, similarly to many autoimmune diseases, predominantly affects women and has long been considered a disease of middle‑aged white women. Earlier epidemiologic estimates suggested a women‑to‑men incidence ratio as high as 10:1. However, more recent population‑based studies have challenged this view, indicating that earlier ratios may have been overestimated.18 For example, pooled analyses from several European countries report a prevalence ratio of approximately 5:1, while studies from the United States and Asia report even lower ratios, around 4:1.15,17,19
Although sex‑based differences in biochemical profiles, histology, and AMA positivity appear to be relatively minor, accumulating evidence suggests that men are more often diagnosed at more advanced disease stages.18 This may partly reflect a lower index of clinical suspicion for PBC in men, contributing to diagnostic delays. Despite a potentially similar natural history, men have been shown to experience worse outcomes. Specifically, male sex has been independently associated with higher rates of death or liver transplantation, including liver‑related mortality, even after adjustment for age, comorbidities, response to UDCA, and disease stage.18 Population‑based studies further support this disparity. For example, a United States–based health system study reported a hazard ratio of 1.47 for all‑cause mortality in men, as compared with women with PBC.19 In our cohort, men were significantly overrepresented in both the youngest (<50 years) and oldest (>80 years) age groups, suggesting possible delays in diagnosis or underrecognition of early disease. This skewed age distribution may reflect the same diagnostic delay patterns described in the literature, and underscores the need for greater awareness of PBC in men.
In our study, AMA‑M2 antibodies—the serologic hallmark of PBC—were detected in 94.4% of the patients, which is consistent with previous reports indicating their presence in 90%–95% of individuals with the disease. The remaining 5% are classified as having AMA‑negative PBC.20 These autoantibodies target the major autoantigen in PBC, that is, the E2 subunit of the pyruvate dehydrogenase complex, located in the inner mitochondrial membrane. Despite the ubiquitous distribution of mitochondria, the disease’s selectivity for cholangiocytes of the small intrahepatic bile ducts is attributed to a loss of immune tolerance to PDC‑E2, triggering a multi‑lineage immune response. Cholangiocytes not only serve as passive targets but also act as active participants in the disease progression via mechanisms such as cellular senescence, which facilitates immune cell recruitment.21 Given the high specificity of AMAs for PBC, their presence in patients with cholestatic biochemical profiles is generally sufficient to establish the diagnosis, thereby eliminating the need for liver biopsy. Nevertheless, isolated AMA positivity without biochemical or clinical evidence of liver disease can be observed in up to 0.5% of otherwise healthy individuals. Among these, only 1 in 6 patients with normal ALP levels will develop PBC within 5 years.20 AMA‑M2‑3E antibodies, which target a recombinant fusion protein composed of 3 subunits of the M2 antigen, were detected in 75.3% of our patients. This is in line with prior studies and further supports their status as one of the most specific serologic markers of PBC.22 The high prevalence of AMA‑M2 and AMA‑M2‑3E in our cohort confirms that the serologic profile of Polish patients with PBC closely mirrors international data, reinforcing the reliability of AMA‑based diagnostic criteria across populations.
We also observed the presence of PBC‑specific antinuclear antibodies—anti‑sp100 and anti‑gp210—in 26.3% and 25.6% of the patients, respectively. This is consistent with previous reports indicating a prevalence of approximately 30%.23 Although these antibodies are less common than AMAs, they are highly specific and diagnostically valuable, particularly in AMA‑negative patients. Anti‑sp100 positivity has been associated with advanced disease stages, as has anti‑gp210, which is similarly correlated with the disease progression.24,25 This aligns with our findings, as both anti‑gp210 and anti‑sp100 were significantly more frequent in the patients treated for more than 2 years than in those treated for a shorter time. Their increased presence may reflect progressive exposure to nuclear antigens during chronic cholangitis and epitope spreading. Association of those antibodies with more advanced disease stages has been noted in prior studies and supports their potential as markers of the disease severity and progression.24,26
Other autoantibodies, such as anti‑liver cytosol type 1 antibody and anti‑promyelocytic leukemia protein antibody, were detected far less frequently in our study group, and their prevalence remained stable regardless of the disease duration. In contrast, anti‑Ro52 antibodies, directed primarily against the cytoplasmic protein TRIM21, were the most commonly detected antibodies after AMAs, found in 34.1% of our patients. This observation is consistent with previous reports and underscores their potential relevance in PBC diagnosis, suggesting a high specificity for PBC.27
According to the EASL guidelines, UDCA at a dose of 13–15 mg/kg/day remains the first‑line treatment for PBC. In the cases of insufficient response or intolerance to UDCA, the use of obeticholic acid was recommended, but the European Medicines Agency authorization was recently withdrawn due to a lack of sufficient evidence of efficacy. Additionally, fibrates have emerged as a promising adjunct due to their ability to improve both biochemical and elastographic parameters, as well as their potential antipruritic effects.13
To evaluate treatment response, various scoring systems have been developed, including the Paris I/II, Barcelona, and Toronto criteria, as well as the GLOBE score.28-30 Although the specific definitions vary, most rely on serum liver biochemistry assessed after 12 months of UDCA therapy, with ALP and total bilirubin serving as key markers. These response criteria are crucial for guiding clinical management and predicting long‑term prognosis.
Persistent elevation of serum ALP remains a hallmark biochemical abnormality in PBC and is frequently the first detectable laboratory indicator. In a study by Lammers et al,31 a log‑linear relationship was observed between ALP levels and the risk of liver transplantation or death, with higher ALP level associated with reduced transplant‑free survival. Interestingly, as shown by Beretta‑Piccoli et al,32 GGT may serve as an even earlier biochemical indicator of PBC, preceding ALP elevation in some cases. Notably, bilirubin level has been identified as an independent predictor of survival.33
The aim of our study was not to evaluate treatment response using formal scoring systems but to describe patient characteristics based on laboratory data from their last follow‑up visit. Our findings showed that 31% of the patients had ALP levels within the normal range, and 27% had normal GGT activity. Conversely, 32% and 48% of the patients had ALP and GGT levels at least twice above the ULN, respectively. These results can suggest that a substantial proportion of patients in our cohort may represent potential nonresponders to UDCA therapy.
Interestingly, GGT activity was lower in the patients treated with UDCA for more than 2 years than in those with a shorter treatment duration (72 IU/l vs 132 IU/l; P = 0.001). This difference was not observed for aminotransferases, ALP, or bilirubin. However, the persistently elevated levels of other markers indicate that key parameters of liver inflammation remain largely unaffected, even with prolonged therapy. While GGT activity was significantly lower in the patients treated with UDCA for over 2 years, this isolated finding should be interpreted with caution. GGT is a sensitive but nonspecific marker of cholestasis and hepatocellular damage, and although it may decrease with effective UDCA therapy, its isolated reduction does not necessarily reflect meaningful clinical improvement or histological stabilization. In our study, other key markers of cholestasis and liver function, such as ALP, bilirubin, and aminotransferases, did not significantly differ between the groups, and the markers of fibrosis, such as FIB‑4, tended to worsen over time. This suggests that the observed GGT decrease may partly reflect treatment‑related modulation of hepatobiliary enzyme activity rather than robust disease control.
According to previous studies, although UDCA has a marked impact on clinical outcomes in patients with PBC, up to 40% of patients exhibit an insufficient response to treatment.31 Importantly, responders experience fewer hepatic events and have a more favorable prognosis than nonresponders.34 Moreover, a Cochrane meta‑analysis suggests that prolonged treatment with UDCA, when initiated in early stages of the disease, is likely required to achieve maximal benefit.35 These issues will be further explored in future analyses of the Polish PBC population.
In addition to achieving biochemical remission, a fundamental goal of PBC treatment is to halt histopathological progression and prevent development of liver cirrhosis. The link between biochemical response and histological outcomes is well recognized; patients who respond to UDCA are significantly less likely to experience disease progression.36 In our cohort, a trend toward worsening was observed across all evaluated markers of liver disease severity in the patients treated with UDCA for more than 2 years. However, a significant difference was observed only for FIB‑4 values. The significantly higher FIB‑4 scores in the patients treated with UDCA for more than 2 years appear unexpected, given the known antifibrotic effects of UDCA in PBC. However, this finding likely reflects underlying differences in the disease stage at treatment initiation rather than a paradoxical effect of therapy. As our study was retrospective and based on cross‑sectional data from the most recent clinical visit, we lacked access to baseline fibrosis assessments. It is therefore possible that patients with longer treatment duration had more advanced disease at the outset, which is a form of indication bias. Importantly, FIB‑4 may also be influenced by age and platelet count, both of which differed slightly between the 2 groups, potentially affecting the score independently of fibrosis progression.
This considerable prevalence of cirrhosis is clinically significant, given the well‑documented association between PBC and hepatocellular carcinoma (HCC). Previous studies have reported an incidence rate of 3.9 cases per 1000 patients per year, with a notably higher risk observed in individuals with suboptimal responses to therapy.37 These findings underscore the need for close monitoring and early identification of inadequate responders. Prompt initiation of second‑line therapies in this population may be critical to reducing the risk of long‑term complications, including cirrhosis and HCC.
Pruritus is one of the hallmark symptoms of PBC, with significant implications for patient quality of life. In our cohort, 46% of the patients reported pruritus—somewhat fewer than the prevalence typically cited in the literature, which ranges from 50% to 80%. Scales defining the severity of PBC symptoms, especially those characterizing itching and fatigue, are very useful in monitoring the clinical course of the disease. However, as they are not routinely used in all centers participating in our study and their possible analysis would be incomplete, we decided not to evaluate them.38-40 Cholestatic pruritus is often described as a disabling symptom that fluctuates independently of the disease severity. It may be present in the early stages of PBC, persist despite normalization of liver biochemistry, and, paradoxically, may disappear in the end‑stage of liver disease. Nonetheless, it typically improves following liver transplantation.41
The EASL guidelines recommend cholestyramine, an anion exchange resin, as the first‑line treatment for cholestatic pruritus in PBC.13 Despite this, only 3.8% of patients in our cohort received cholestyramine. This low usage may reflect factors such as mild pruritus not requiring pharmacologic intervention, patient intolerance, which may be relatively common, or limitations related to the drug cost and availability.39 PPAR agonists are becoming increasingly important in the treatment of PBC, including the reduction of cholestatic pruritus.42 Although only 8.8% of our patients received fenofibrate, a representative of this group of drugs, it might be expected that the percentage of patients treated with PPAR agonists will increase in the near future. Notably, other antipruritic agents, including second‑line therapies, such as rifampicin, were reported only sporadically. Moreover, the prevalence of pruritus in our cohort did not differ according to the duration of UDCA therapy, consistent with previous findings that UDCA offers limited efficacy in the management of this symptom.35,43
Although only 0.6% of our patients received obeticholic acid, it is important to note that this agent has been associated with dose‑dependent exacerbation of pruritus, reported in up to 40% of the treated patients, which may necessitate treatment discontinuation.44
Limitations
The most important limitations of our study, resulting from its retrospective nature, are the lack of baseline data at the time of diagnosis and treatment initiation, limited freshness of laboratory data, and the absence of detailed information on UDCA dosing, which could influence therapeutic response. Additionally, we were unable to systematically assess comorbidities such as diabetes, obesity, cardiovascular disease, or potential overlap syndromes, which could significantly influence both the disease course and interpretation of biochemical parameters. Similarly, data on alcohol consumption and concomitant medications (including statins, immunosuppressants, or hepatotoxic drugs) were incomplete or unavailable for many patients. These limitations stemmed from inconsistencies and gaps in outpatient and hospital records and may have led to underreporting of relevant clinical factors. We emphasize the need for prospective, structured data collection in future analyses. For this reason, at this stage of the study, we decided to limit ourselves to basic information, which with 100% certainty was available for all patients. Another limitation of the study was the omission of asymptomatic patients who did not yet require treatment. This resulted from the lack of a national screening program for PBC, which would allow for the detection of the risk of the disease at an early stage and its monitoring.
Conclusions
This first, national, retrospective characterization of PBC in Poland provides preliminary demographic and clinical insights but is limited by its design and potential selection bias. Our data suggest that long‑term efficacy of UDCA is limited for a meaningful subset of patients, and that symptom burden remains undertreated. Anti‑gp210, anti‑sp100, and anti‑Ro52 antibodies may be useful serologic markers. These observations should be validated, and their prognostic and therapeutic implications defined, in multicenter, prospective studies.
- Lleo A, Marzorati S, Anaya JM, Gershwin ME. Primary biliary cholangitis: a comprehensive overview. Hepatol Int. 2017; 11: 485‑499. | Crossref
- Ahrens EH Jr, Kunkel HG. The relationship between serum lipids and skin xanthomata in 18 patients with primary biliary cirrhosis. J Clin Invest. 1949; 28: 1565‑1574. | Crossref
- Beuers U, Gershwin ME, Gish RG, et al. Changing nomenclature for PBC: from ‘cirrhosis’ to ‘cholangitis’. J Hepatol. 2015; 63: 1285‑1287. | Crossref
- Boonstra K, Beuers U, Ponsioen CY. Epidemiology of primary sclerosing cholangitis and primary biliary cirrhosis: a systematic review. J Hepatol. 2012; 56: 1181‑1188. | Crossref
- Lleo A, Leung PSC, Hirschfield GM, Gershwin ME. The pathogenesis of primary biliary cholangitis: a comprehensive review. Semin Liver Dis. 2020; 40: 34‑48. | Crossref
ARTICLE INFORMATION