A 37‑year‑old woman with a history of uterine myomectomy several years before, currently qualified for a hysterectomy due to recurrence, was transferred to a tertiary center with an abnormal structure in the inferior vena cava (IVC) penetrating to the right atrium (RA), accidentally found on preoperative computed tomography (CT). She presented with nonspecific abdominal discomfort and exertional dyspnea. Due to an initial suspicion of thrombosis, antithrombotic therapy was initiated, but turned out to be ineffective.
Echocardiography showed a tumor in the RA, resulting in functional tricuspid valve stenosis (mean pressure gradient, 5 mm Hg; Figure 1A and 1B). Chest CT was performed to rule out pulmonary embolism, simultaneously confirming the presence of pathological masses, including in the IVC and RA, suspected of proliferative nature. Abdominopelvic magnetic resonance imaging (MRI) revealed a contiguous, enhancing, soft‑tissue mass arising from the uterine venous plexus, and extending cephalad through the IVC into the RA (Figure 1C). However, positron emission tomography / CT showed no lesions with increased glucose metabolism.
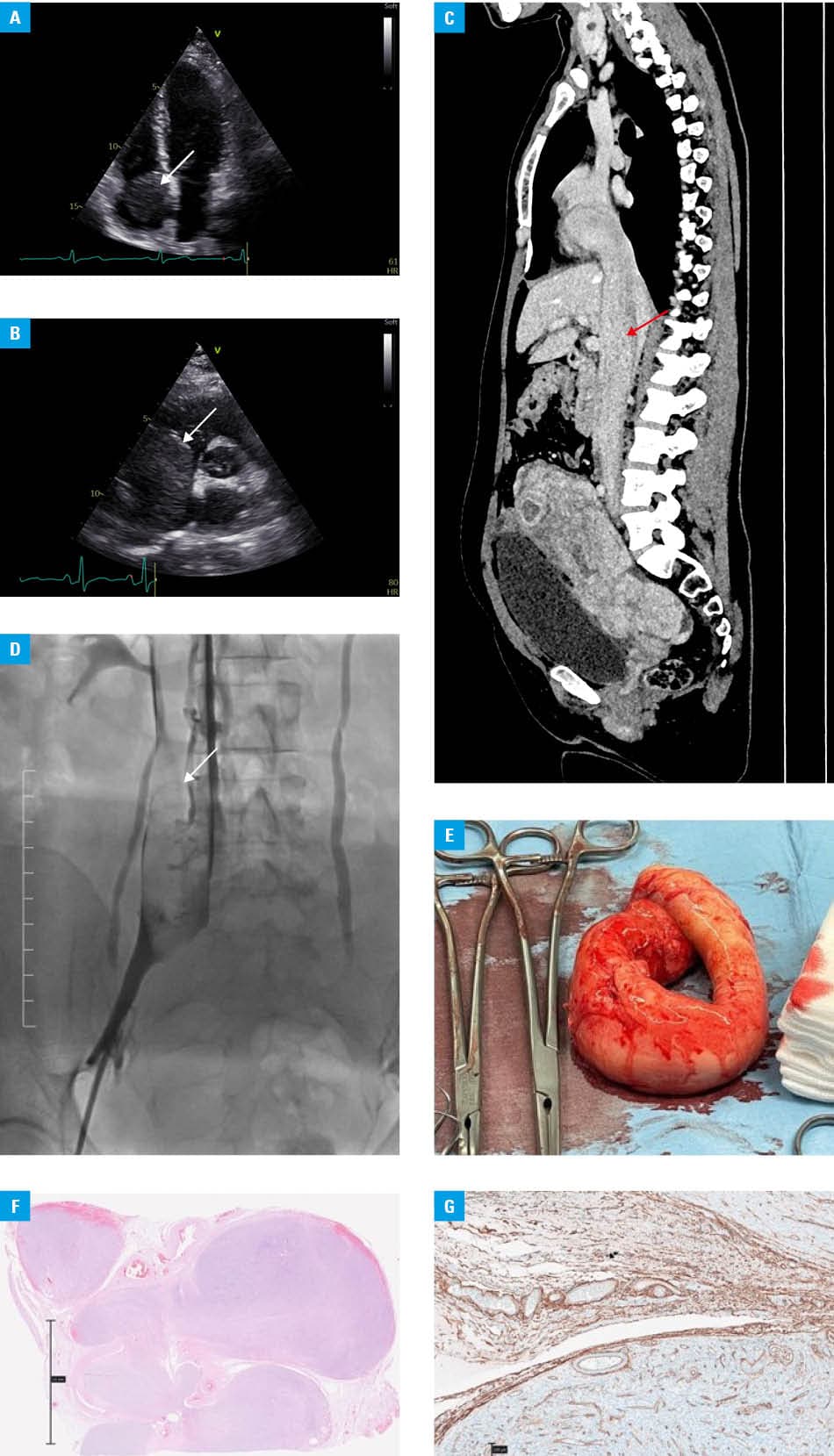
Subsequently, an attempt was made to obtain material for histopathologic examination. Venous angiography followed by biopsy of the tumor was performed (Figure 1D). Unfortunately, the obtained specimen turned out to be nondiagnostic.
A multidisciplinary team discussed treatment options, and finally, the patient underwent 1‑step complete surgical resection. In deep hypothermia, the uterus, oviducts, IVC, and RA tumor were removed. The tumor extraction from the heart required partial resection of the RA wall followed by its reconstruction. Perioperative period was uncomplicated. Intraoperative photography confirmed gross appearance of the tumor spanning from the pelvic cavity to the RA (Figure 1E). Histopathologic examination allowed for the diagnosis of intravenous leiomyomatosis (IVL; Figure 1F and 1G).
IVL is an extremely rare tumor, with benign histopathologic features, originating in the uterus or the uterine vessels, and penetrating to the iliac veins, IVC, or even right heart chambers and pulmonary arteries. Its intracardiac extension accounts for about 10% of cases.1 To date, about 300 cases of IVL have been reported. In recent years, with newer iterations of imaging techniques and diagnostic improvement, the detection rate has gradually increased.
Clinical presentation is primarily determined by the size and location of the tumor. Progressive intraluminal extension may propagate through the IVC into the right heart, resulting in life‑threatening complications.
Various imaging modalities, such as echocardiography, abdominal ultrasound, CT, and MRI, are available for detection and diagnosis of IVL.
On histopathologic examination, the presentation is similar to that of typical benign uterine leiomyomas, but is distinguished from that of smooth muscle tumors by the tumor cells growing in the vasculature lined with endothelial cells and covered by flattened endothelial cells on the surface.2
Currently, there are no specific guidelines for IVL treatment, but available literature suggests radical resection as the preferred method. IVL usually adheres to but does not invade the vessel wall and, therefore, can usually be removed by traction. A combined multidisciplinary thoracoabdominal operation with cardiopulmonary bypass is indicated if IVL is extending to the right heart chamber. The main concern in postoperative period is IVL recurrence, estimated at 22.2%.3
This case illustrates a rare presentation of a benign uterine tumor with potentially life‑threatening intracardiac extension, emphasizing the critical role of multimodal imaging in diagnosis and surgical planning.
- Gwacham NI, Manyam M, Fitzsimmons CK, et al. Multidisciplinary approach to pelvic leiomyomatosis with intracaval and intracardiac extension: a case report and review of the literature. Gynecol Oncol Rep. 2022; 40: 100946. | Crossref
- Clay TD, Dimitriou J, McNally OM, et al. Intravenous leiomyomatosis with intracardiac extension ‑ a review of diagnosis and management with an illustrative case. Surg Oncol 2013; 22: e44‑e52. | Crossref
- Low HY, Zhao Y, Huang KS, et al. Intravenous leiomyomatosis of the uterus: a clinicopathological analysis of nine cases and literature review. Taiwan J Obstet Gynecol. 2017; 56: 362‑365. | Crossref
ARTICLE INFORMATION