A rare cause of gastrointestinal bleeding and intussusception in a patient with undifferentiated pleomorphic sarcoma

 CC BY 4.0
CC BY 4.0
A rare cause of gastrointestinal bleeding and intussusception in a patient with undifferentiated pleomorphic sarcoma
Undifferentiated pleomorphic sarcoma (UPS), formerly known as malignant fibrous histiocytoma, is soft tissue sarcoma derived from mesenchymal cells. It is a rare tumor with incidence of 1–2 per 100 000 individuals per year, developing usually in the sixth to eighth decade of life. UPS is typically localized in deep muscles of the limbs (70% of the cases) and retroperitoneal space (15%).1,2
However, in rare cases, it can be localized in the intestines. The symptoms of primary intestinal UPS are uncharacteristic, typical of various common gastrointestinal diseases, and they include bleeding, pain, and weight loss.3
To our knowledge, we present the first case of small bowel intussusception caused by UPS reported in Poland.
A 70‑year‑old man was admitted for diagnostic evaluation of severe anemia. His medical history included renal replacement therapy for 6 months, hypertension, and chronic heart failure. He denied any symptoms of gastrointestinal (GI) bleeding. Previous esophago‑gastro‑duodenoscopy (EGD) performed for GI bleeding 8 months earlier found Mallory–Weiss tear as the cause of bleeding, and no other important findings were reported.
Results of the laboratory tests performed on admission showed a low hemoglobin concentration (6 g/dl; reference range [RR], 12–14.7 g/dl) and iron deficiency (transferrin saturation, 19%; RR, 20%–45%). EGD identified a reddened swollen polyp measuring 9 mm in diameter in the descending duodenum, covered with clot, but with no active bleeding. A single hemoclip was applied.
The patient was treated with proton pump inhibitors (8 mg of pantoprazole per hour in continuous infusion) and blood transfusions, but the course was complicated by acute ST segment elevation myocardial infarction and paroxysmal atrial fibrillation, followed by initiation of antiplatelet therapy alongside heparinization during hemodialysis.
Further 3 EGDs were performed within 3 weeks due to suspected GI bleeding: several polyps were found in the antrum and duodenum with oozing bleeding (Figure 1A), treated with hemoclips (Figure 1B), endoloops, and application of hemostatic powder. However, all these attempts did not stop blood loss, and the patient received a total of 27 units of packed red blood cells within 30 days.
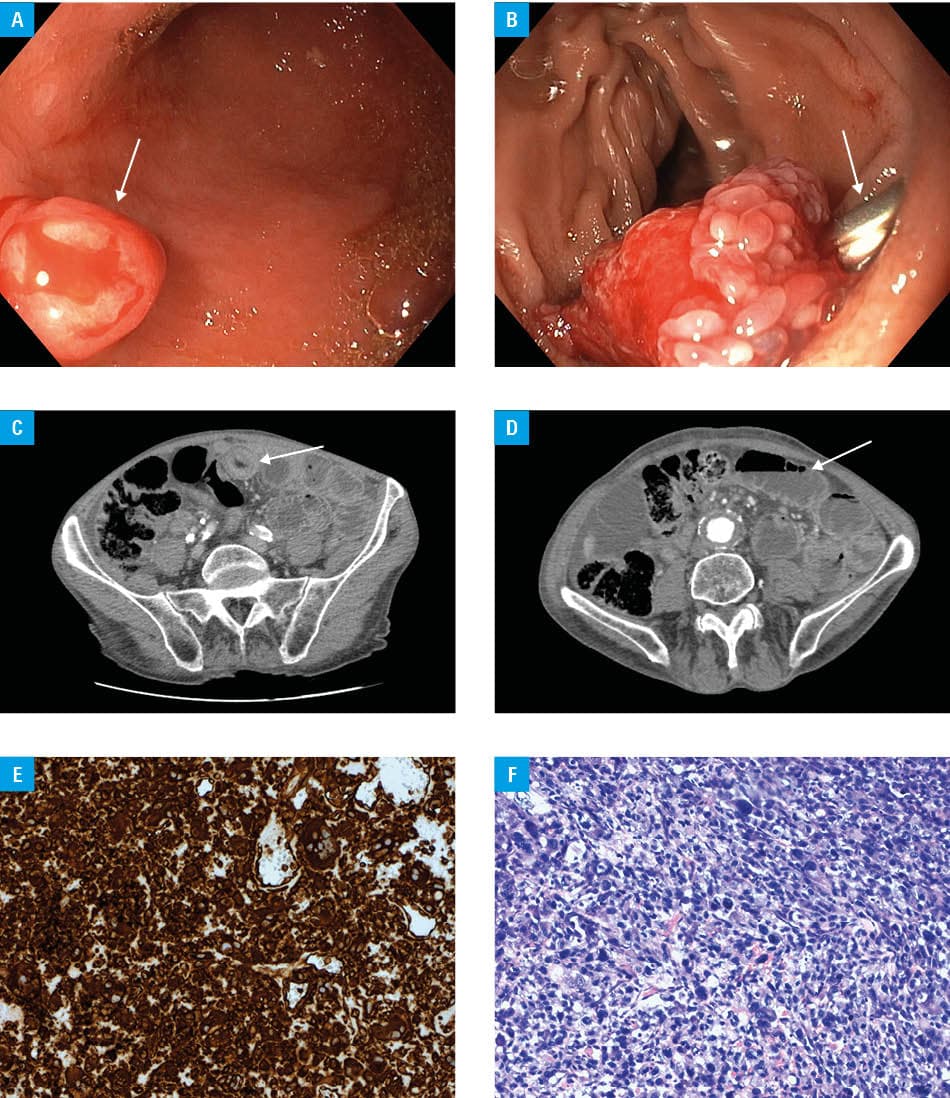
On day 25 after admission, symptoms of small bowel obstruction developed (vomiting, abdominal distention, and recurrent colicky pain). Emergency computed tomography showed small bowel intussusception with microperforation (Figure 1C and 1D), as well as metastatic tumors in the right lung and the brain. Emergency surgery with partial jejunal resection was performed. Small bowel intussusception was found over a tumor, as well as dozens of similar tumors located mainly in the proximal part of the jejunum. Pathology report indicated an ulcerated tumor of 5 cm in diameter infiltrating the full thickness of the bowel wall and multiple smaller tumors infiltrating the muscular membrane.
The patients’ general condition further deteriorated, complicated by hemorrhage within brain metastasis, and he died 6 days after laparotomy.
Histopathologic examination suggested undifferentiated pleomorphic sarcoma (immunohistochemical stains were positive for vimentin and partially for CD68 (LCA–, CK–, VIM+, HMB45–, S100–, SMA–, CD34–, Ki67 >70%, CD68+/–; Figure 1E and 1F).
Intestinal intussusception is most often caused by malignant or benign tumors (33% and 38%, respectively), but sarcomas are a very uncommon cause of the disease.4
Undifferentiated pleomorphic sarcoma of the intestines is an extremely rare condition with nonspecific symptoms and rapid progression, including metastases to distant organs. It is, therefore, almost impossible to diagnose preoperatively and carries an unfavorable prognosis. In this case, the main difficulties were cardiac complications and renal replacement therapy, requiring antiplatelet therapy and anticoagulants, respectively. Moreover, the intestinal source of bleeding was not accessible with standard endoscopic procedures.
- Eto R, Hoshino I, Takiguchi N, et al. Surgical resection of undifferentiated pleomorphic sarcoma (UPS) with jejunal perforation, a suspected case of metastasis of lung cancer. Clin J Gastroenterol. 2021; 14:1386‑1391. | Crossref
- Fu D‑L, Yang F, Maskay A, et al. Primary intestinal malignant fibrous histiocytoma: two case reports. World J Gastroenterol WJG. 2007; 13: 1299‑1302. | Crossref
- Kodera K, Hoshino M, Takahashi S, et al. Surgical management of primary undifferentiated pleomorphic sarcoma of the rectum: a case report and review of the literature. World J Surg Oncol. 2022; 20: 199. | Crossref
- Lambrinow J, Świątkowski F, Jurga M, et al. Intussusception caused by an extremely rare tumor: undifferentiated spindle cell sarcoma. Pol Arch Intern Med. 2023; 133: 16491. | Crossref
ARTICLE INFORMATION