Alveolar echinococcosis of the adrenal gland: a rare diagnostic challenge among adrenal incidentalomas

 CC BY 4.0
CC BY 4.0
Alveolar echinococcosis of the adrenal gland: a rare diagnostic challenge among adrenal incidentalomas
Adrenal tumors affect around 3%–5% of middle‑aged individuals, and even up to 10% of the elderly. Adrenal incidentalomas are usually benign, nonsecreting adenomas that rarely require therapeutic interventions. However, sometimes they pose difficult diagnostic challenges, as the list of differential diagnoses for an adrenal tumor is very complex.1 Parasitic infections of the adrenal gland are exceptionally rare and constitute some of the most challenging diagnoses.
Our patient was a 66‑year‑old woman who was admitted to an endocrine department for evaluation due to adrenal tumor regrowth after adrenalectomy. The tumor was first visualized 3 years earlier on abdominal ultrasound performed because of hematuria. Computed tomography (CT) of the abdomen, followed by magnetic resonance imaging (MRI), showed a 64 mm × 74 mm × 70 mm tumor with a density of 25 Hounsfield units, likely arising from the right adrenal gland, infiltrating the hilum of the liver and the right crux of the diaphragm. Hormonal assessment showed elevated 3‑methoxytyramine excretion in a 24‑hour urine collection. The patient was diagnosed with dopamine‑secreting pheochromocytoma and referred for surgery. The initial histopathologic examination demonstrated chronic inflammatory infiltration with no signs of neoplastic process.
On subsequent follow‑up MRIs, a gradual progression of the residual tumor was observed, which prompted a referral to our department for further diagnostics.
On admission, the patient complained of fatigue, tiredness, and decreased exercise tolerance, which could not have been unequivocally attributed to any of her comorbidities (type 2 diabetes, angina pectoris, chronic gastritis, hypertension, Parkinson disease, and hypothyroidism [status post‑thyroidectomy]). On physical examination, minor leg edema and varicose veins of the legs were observed. Laboratory testing indicated mild normocytic anemia (hemoglobin, 11.2 g/dl; reference range [RR], 11.8–15.8 g/dl), increased eosinophil count (0.7 × 103/μl; RR, 0.02–0.5 × 103/μl), and an elevated chromogranin A level (145.92 ng/dl; RR, 19–100 ng/dl). Abdominal CT visualized a 79 mm × 61 mm × 90 mm lesion in the adrenalectomy bed, which was infiltrating neighboring organs (Figure 1A–1D). No abnormalities in hormonal test results were observed. We assumed that the previously elevated 3‑methoxytyramine urinary excretion was attributable to chronic intake of levodopa, used for treatment of Parkinson disease, as 3‑methoxytyramine is a metabolite of levodopa.
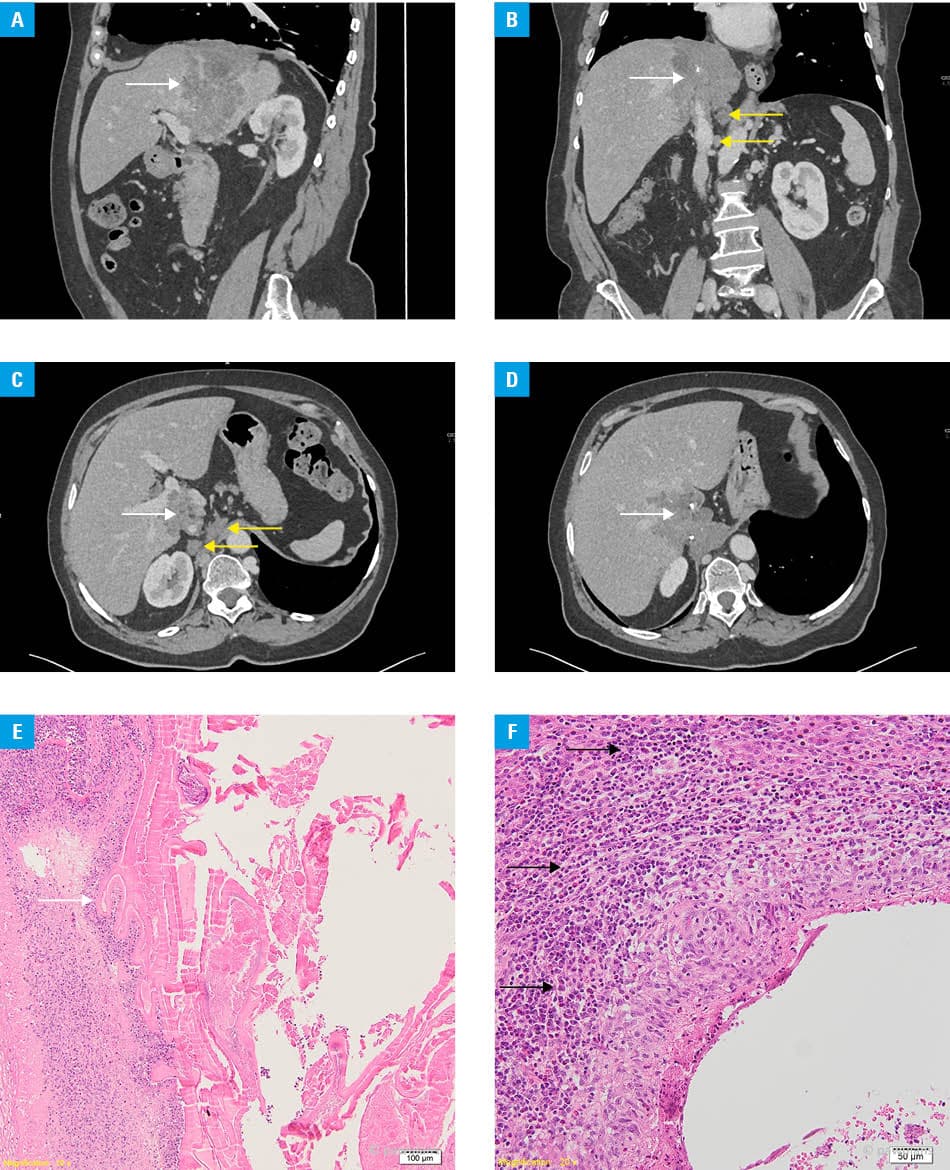
We retrieved a surgical pathology specimen for secondary analysis, which was indicative of a parasitic infection (Figure 1E and 1F). Consequently, we tested the patient for the presence of Echinococcus immunoglobulin G antibodies (enzyme‑linked immunosorbent assay), and the result was positive (25 NovaTec units, where <9 means negative, 9–11 is indeterminate, and >11 corresponds to positive). To differentiate between E. multilocularis and E. granulosus infections, we checked for antibodies against endomorphin 2 (Em2), which are highly sensitive and specific for E. multilocularis. The Em2 index value was above 3 (results ≥1 are considered reactive). Finally, Western blotting further confirmed the diagnosis, as the band profile was unequivocally positive for E. multilocularis infection. Regarding potential epidemiologic risk factors, the patient was previously employed in the agricultural sector and confessed to eating wild forest berries without washing them. Eventually, she was diagnosed with alveolar echinococcosis (AE) in an advanced, unresectable stage P4N1M1, and pharmacological treatment with albendazole was implemented.
AE is a lethal and devastating disease that mimics a malignant, metastasizing tumor. Timely diagnosis is of utmost importance, as an early introduction of antiparasitic treatment reduces the rate of relapse after surgery or disease dissemination after biopsy.2 Unfortunately, none of the international endocrine guidelines mention testing for parasitic infections in the case of an adrenal tumor. Previously described cases of adrenal gland AE presented with imaging features similar to our patient’s tumor.3-5 To date, only cases of right adrenal gland AE have been described, which suggests that despite imaging features indicative of an adrenal tumor, the primary site of the infection—at least in some cases—might still be a peripheral part of the liver from which the disease extends into the adrenal gland through contiguous spread.
We recommend that screening for AE should be considered in patients with hormonally inactive tumors of the right adrenal gland with suspicious imaging features and infiltration of the liver or the vena cava.
- Cyranska‑Chyrek E, Szczepanek‑Parulska E, Olejarz M, Ruchala M. Malignancy risk and hormonal activity of adrenal incidentalomas in a large cohort of patients from a single tertiary reference center. Int J Environ Res Public Health. 2019; 16: 1872. | Crossref
- Brunetti E, Kern P, Vuitton DA. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Tropica. 2010; 114: 1‑16. | Crossref
- Witowska A, Sykutera M, Szczepanek‑Parulska E, Ruchała M. Parasitic infestation presenting as advanced infiltrating tumor mimicking adrenal cancer. Am J Med. 2025; 9: 1227‑1230. | Crossref
- Spahn S, Helmchen B, Zingg U. Alveolar echinococcosis of the right adrenal gland: a case report and review of the literature. J Med Case Rep. 2016; 10: 325. | Crossref
- Wilk-Śledziewska K, Śledziewski R, Piotrowska W, et al. Unraveling the enigma: Echinococcus multilocularis in the adrenal gland as a very rare cause of hypertension in a young patient. Pol Arch Intern Med. 2024; 134: 16839. | Crossref
ARTICLE INFORMATION