Creeping fat is not exclusive to Crohn disease: a case of small bowel xanthomatosis causing its complete obstruction



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Creeping fat is not exclusive to Crohn disease: a case of small bowel xanthomatosis causing its complete obstruction
A 70‑year‑old woman was admitted due to epigastric pain, vomiting, and abdominal distension. Her medical history included arterial hypertension and hypercholesterolemia, and she was taking candesartan 16 mg, lercanidipine 20 mg, and rosuvastatin 20 mg daily. Computed tomography showed multiple gas‑fluid levels consistent with bowel obstruction (Figure 1A), caused by the last loop of the ileum with a thickened wall and narrowed lumen (Figure 1B). She underwent emergency exploratory laparotomy, which identified numerous small pale nodules covering the surface of the small bowel and mesentery (Figure 1C), suggesting miliary tuberculosis or peritoneal carcinomatosis, as well as a shortened and constricted ileum with creeping fat (Figure 1D) that may have indicated Crohn disease. The procedure included biopsy of peritoneal nodules and resection of the last loop of ileum with manual end‑to‑end anastomosis, since the lumen was too narrow to introduce a stapler (Figure 1E). The patient was discharged home in a satisfactory condition.
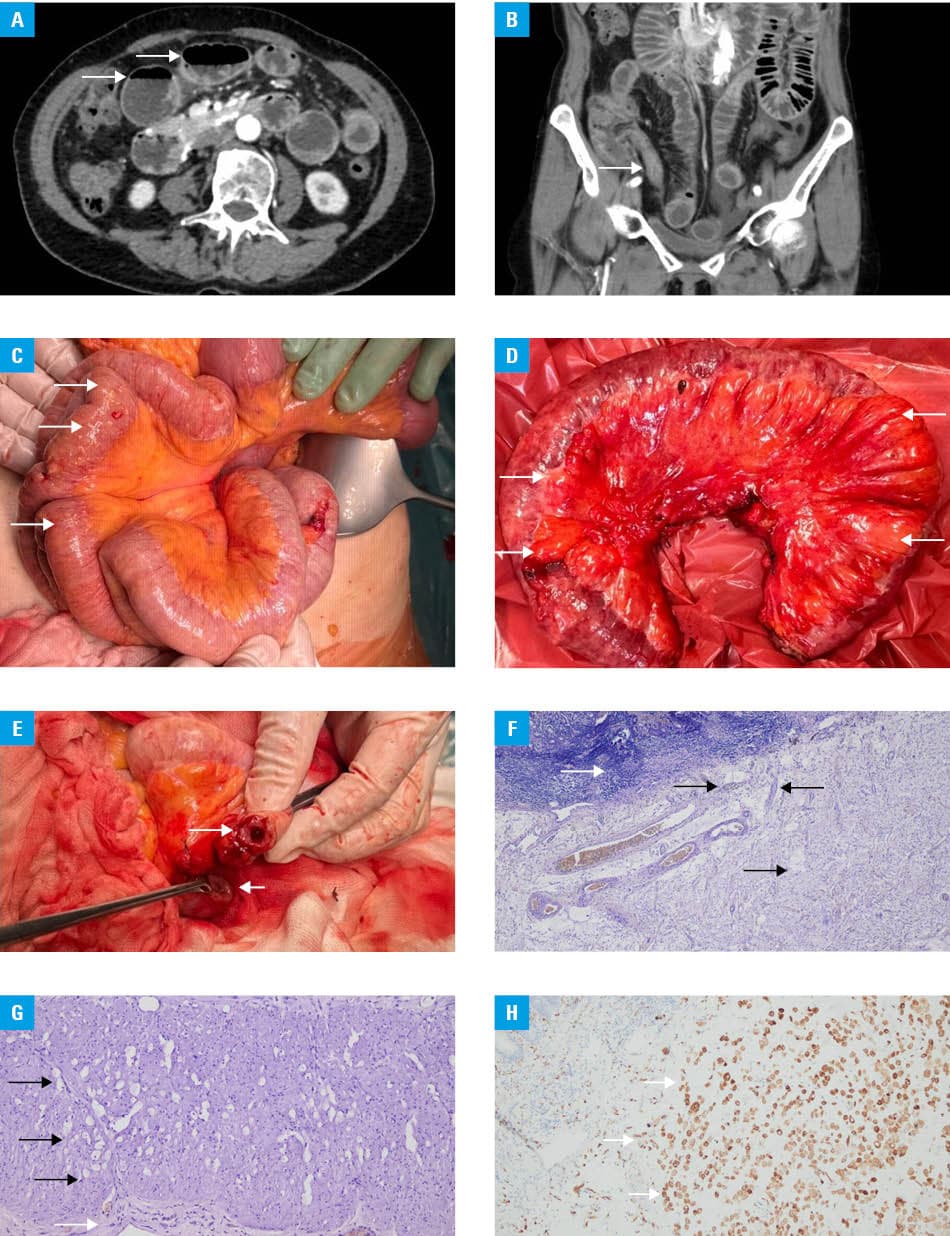
Pathologic examination showed extensive thickening of the submucosa (Figure 1F) and muscularis propria (Figure 1G) due to infiltration with foamy macrophages confirmed on immunohistochemical staining with anti‑CD68 antibody (Figure 1H). Specimens were negative for pan‑cytokeratin, S100, SOX10, PAX8, CAIX, GATA3, periodic acid Schiff (PAS), and mucicarmine. There was no confirmation of either tuberculosis, carcinomatosis, or Crohn disease.
Xanthomas are small nodules consisting of cholesterol‑rich foamy macrophages that typically involve skin, especially eyelids, tendons, and joints. Multiple or diffuse xanthomas—xanthomatosis—may also appear in any part of the digestive tract, most commonly the stomach, but they are usually small and asymptomatic, accompanying chronic gastritis, intestinal metaplasia, Helicobacter pylori infection, duodenogastric reflux, and postgastrectomy status. Small bowel xanthomatosis is a possible but extremely rare cause of bowel obstruction, described in very few articles to date. It may be associated with hyperlipidemia, lymphoproliferative disorders, chronic mesenteric ischemia, previous radiotherapy, chemotherapy, immunosuppression, or infections (disseminated Mycobacterium avium‑intracellulare and cytomegalovirus colitis), but the relationship is debatable. Our patient showed no signs of the aforementioned diseases, and her lipid profile was normal (total cholesterol, 107 mg/dl; reference range [RR], 120–200 mg/dl; triglycerides, 75 mg/dl; RR, 45–150 mg/dl). Differential diagnosis should include poorly differentiated carcinoma (typically positive for pan‑cytokeratin), storage diseases, muciphages (positive for PAS stain), infections, such as Whipple disease (PAS‑positive macrophages containing Gram‑positive bacilli), Mycobacterium (positive for Ziehl–Neelsen stain), or AIDS, macroglobulinemia, and Erdheim–Chester disease.1-4
Based on macroscopic similarity, we postulated to include Crohn disease in this list. Creeping fat, also known as the fat wrapping sign, is a result of pathologic fibrofatty proliferation of mesenteric tissues that gradually encase the adjacent bowel. This feature was noted by Burrill B. Crohn himself in his original article describing regional ileitis. Creeping fat is regarded as a hallmark of Crohn disease that correlates with disease activity and presents prognostic qualities, but as we showed, it may as well accompany small intestine xanthomatosis, although its incidence is far less common.5 To sum up, xanthomatosis should be included in differential diagnosis in the cases of inflammatory tumor / stricture causing small bowel obstruction.
- Barrera‑Herrera LE, Arias F, Rodríguez‑Urrego PA, et al. Small bowel obstruction due to intestinal xanthomatosis. Case Rep Pathol. 2015; 2 015: 231830. | Crossref
- Moran AM, Fogt F. 70‑year‑old female presenting with rectosigmoid (colonic) xanthoma and multiple benign polyps ‑ case report. Pol J Pathol. 2010; 1: 42‑45. | Crossref
- Nielsen SL, Ingeholm P, Holck S, et al. Xanthomatosis of the gastrointestinal tract with focus on small bowel involvement. J Clin Pathol. 2007; 60: 1164‑1166. | Crossref
- Yamamoto S, Matsumura K, Seno H. Segmental xanthomatosis of the ileum. Clin Gastroenterol Hepatol. 2019; 17: e18. | Crossref
- Yin Y, Xie Y, Ge W, et al. Creeping fat formation and interaction with intestinal disease in Crohn’s disease. United Eur Gastroenterol J. 2022; 10: 1077‑1084. | Crossref
ARTICLE INFORMATION