Proximity of traffic roads to the place of residence vs risk of acute cellular injury following heart transplantation

 CC BY 4.0
CC BY 4.0
Proximity of traffic roads to the place of residence vs risk of acute cellular injury following heart transplantation
Introduction
Heart transplantation is considered one of the most effective therapies for end‑stage heart failure due to its favorable long‑term outcomes.1 Recent immunosuppressive protocols have demonstrated efficacy, often marked by clinically silent episodes of rejection, underscoring the importance of endomyocardial biopsy in patient monitoring. Post‑transplant treatments primarily aim to suppress inflammatory responses. Identifying potential modulatory factors that may influence patient survival remains essential, as there is still room for improvement in transplant outcomes.
Environmental factors, including residential proximity to high‑traffic roads, may contribute to immune system activation in transplant recipients.2 Previous studies3 have documented traffic‑related pathophysiological mechanisms in humans, such as endothelial dysfunction, oxidative stress, and systemic inflammatory responses. Living near major traffic roads may exacerbate chronic inflammatory conditions,4 primarily due to increased exposure to air pollutants and noise.
This study aimed to investigate the relationship between endomyocardial biopsy results in heart transplant recipients and environmental factors, particularly those related to traffic road proximity.
Patients and methods
Thirty consecutive heart transplant recipients, at a median age of 49 years (range, 38–60 y), were enrolled in this prospective study to evaluate the potential association between the risk of acute cellular myocardial injury and residential proximity to traffic roads. All patients underwent orthotopic heart transplantation between 2020 and 2022 in Poland and received standard triple immunosuppressive therapy consisting of a calcineurin inhibitor (tacrolimus), mycophenolate mofetil, and prednisolone.
Protocol‑based endomyocardial biopsy (EMB) results were evaluated at 4 time points following transplantation. The patients with biopsy‑confirmed rejection episodes within the preceding 6 months or with positive cross‑match results were excluded from the analysis. In the control group, EMB was performed 1 week after an acute myocardial rejection episode was resolved, confirming the absence of ongoing cellular myocardial injury. The observation period ranged from median (interquartile range [IQR]) of 154 (138–162) to 365 (276–371) days postorthotopic heart transplantation.
The road density index was defined as the total length of a specified road type and the length of all types of roads in a buffer area within a specified radius. We defined 6 types of roads depending on their function, vehicle load, and legal speed limit. The proximity assessment was determined by the buffer radius, including 4 radius sizes.
The study utilized geomapping analysis to assess the proximity and density of traffic roads within 300-, 500-, 700-, and 1000‑meter buffers surrounding each patient’s place of residence.
Main roads were defined as high‑volume routes connecting cities or towns, excluding highways. Local roads referred to those providing access to residential areas, small businesses, or neighborhoods, excluding internal or private roads.
Personalized exposure to ambient air pollutants’ concentration was estimated based on the distance of each patient’s place of residence from air quality monitoring stations.5 Geomaps generated by the National Institute for Environmental Research illustrated the density of traffic roads surrounding each place of residence. Air pollution exposure was projected based on the mean concentration values estimated for the area of residence.
All EMB samples were analyzed at a designated reference center. Tissue fragments were fixed in 4% buffered formaldehyde, routinely dehydrated through a graded series of ethyl alcohol, and embedded in paraffin wax via xylene. The 5 µm‑thick sections were stained with hematoxylin and eosin. The grade of rejection was assessed according to the working formulation of the International Society for Heart and Lung Transplantation.6
Statistical analysis
Continuous variables were expressed as medians (IQRs) due to non‑normal data distribution. Categorical variables were presented as counts and percentages. Comparisons of continuous variables between the groups were performed using either the t test or the Mann–Whitney test, depending on the outcome of normality assessments. Myocardial injury risk was defined by ordinal variables describing the stages of immunologic response,6 including the presence and severity of lymphocyte infiltration, followed by myocyte necrosis and vascular changes. Categorical variables were compared using the Fisher exact test. The Spearman rank correlation coefficients were calculated to assess associations between EMB results (grades, 0, 1a, 1b, 2a, and 3a) in the whole analyzed population of heart recipients, and traffic road densities within the specific buffer zones. Statistical analyses were conducted using JASP statistical software 2003, version 0.18.1 (JASP Services BV, Amsterdam, the Netherlands). A P value below 0.05 was considered significant.
Ethics
Informed consent was obtained from all participants. The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Review Board of Poznan University of Medical Sciences, Poznań, Poland (5694/20) for research involving human participants.
Results
The study group consisted of 25 men (83%) and 5 women (17%) who underwent heart transplantation due to dilated cardiomyopathy (n = 17, 57%) or ischemic cardiomyopathy (n = 13, 43%). Comorbidities included arterial hypertension (n = 10, 33%), dyslipidemia (9 patients, 30%), and kidney failure (n = 6, 20%). Diabetes mellitus was diagnosed in 22 patients (73%), of whom 17 (57%) developed new‑onset diabetes after transplantation.
The observation period ranged from median (IQR) 154 (138–162) to 365 (276–371) days post‑transplant. The protocol EMBs, in the entire population, were performed within median (IQR) 154 (138–154), 182 (158–193), 273 (192–280), and 365 (276–371) days following heart transplantation as first, second, third, and fourth measurements, respectively.
During this time, 17 patients experienced episodes of acute cellular injury, confirmed by EMB. Detailed demographic and clinical characteristics, along with the EMB findings and immunosuppressive regimens, are presented in Supplementary material, Table S1.
There were no differences in echocardiographic or laboratory parameters between the groups, except for plasma troponin I levels, which were elevated in the study group (P <0.001). Intergroup differences in immunosuppressive regimens were observed in steroid dosing (P = 0.01) and mycophenolate mofetil dosing (P = 0.01) at the fourth measurement point, though no significant differences were found in drug concentration levels (Supplementary material, Table S1). Following each EMB‑confirmed episode of acute cellular rejection, a standard treatment protocol was administered, consisting of 3000 mg of intravenous methylprednisolone over 3 consecutive days, followed by an increase in oral prednisolone dosage.
Differences in traffic road density between the patients with acute myocardial injury and those without rejection were observed within the 700‑meter (median [IQR] 0.027 [0.022–0.03] vs 0.014 [0.008–0.016] m/m²; P <0.001) and 1000‑meter (median [IQR] 0.052 [0.042–0.056] vs 0.026 [0.013–0.031] m/m²; P <0.001) residential buffers. No differences were found in the 300‑meter (median [IQR] 0.015 [0.007–0.017] vs 0.012 [0.009–0.013] m/m²; P = 0.29) or 500‑meter (median [IQR] 0.006 [0.003–0.006] vs 0.004 [0.003–0.005] m/m²; P = 0.28) buffers. The corresponding geomaps illustrating traffic road density across residential areas are presented in Figure 1.
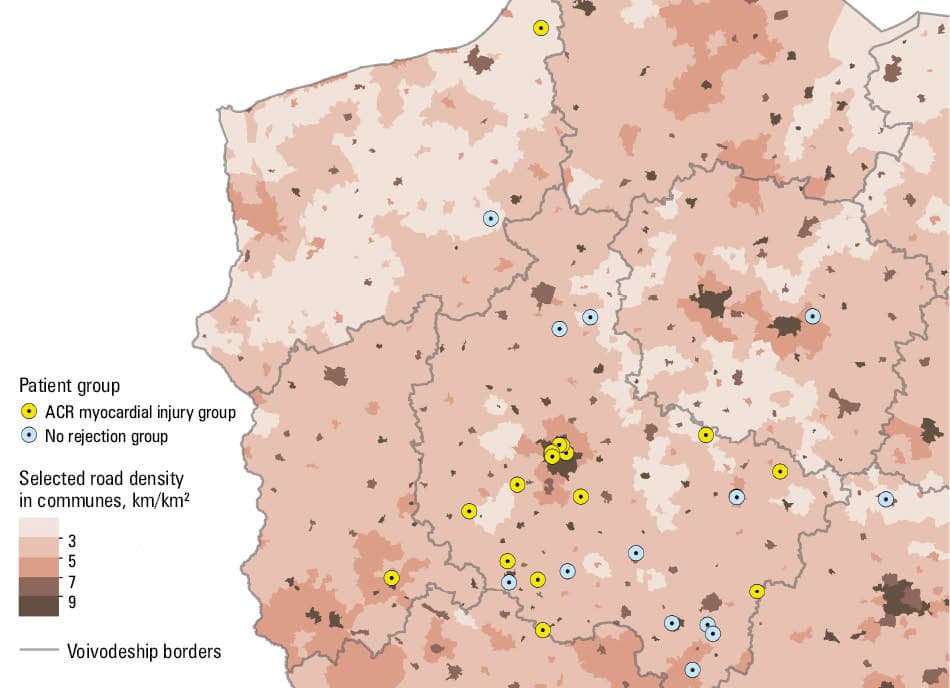
Abbreviations: ACR, acute cellular rejection
A correlation was observed between the EMB results and road density for the 300‑meter residential buffer in general (R = 0.37; P = 0.047); however, not for particular types of roads (main roads, R = 0.27; P = 0.6; local roads; R = 0.22; P = 0.3). Similarly, a correlation between the EMB results and road density was identified for the 500‑meter buffer (R = 0.39; P = 0.04), though no associations were found for either main (R = 0.27; P = 0.6) or local roads (R = 0.21; P = 0.26).
Within the 700‑meter buffer, road density was again correlated with the risk of myocardial injury (R = 0.36; P = 0.052), while the densities of main (R = 0.21; P = 0.19) and local roads (R = 0.1; P = 0.19) were not associated with this outcome.
Comparable observations were made within the 1000‑meter buffer, where overall road density correlated with myocardial injury risk (R = 0.38; P = 0.06), but no correlations were found for main (R = 0.09; P = 0.77) or local roads (R = 0.1; P = 0.62).
No correlations were identified between the EMB results and inflammatory markers, such as C‑reactive protein (R = 0.25; P = 0.19) or neutrophil‑to‑lymphocyte ratio (R = 0.13; P = 0.48), and no associations were obsereved between the EMB results and the myocardial injury marker troponin I concentration (R = 0.18; P = 0.32).
Discussion
To the best of our knowledge, this is the first study to suggest a potential correlation between acute myocardial injury following orthotopic heart transplantation and the proximity of traffic roads to the patient’s place of residence. We aimed to emphasize the role of environmental factors, including industrialization, in the risk of inflammatory activation among immunosuppressed individuals. The novelty of this study lies in its consideration of residential environmental characteristics as modulators of transplant outcomes, thereby supporting the need for a personalized approach to post‑transplant care. Individualized immunosuppressive therapy could be adjusted not only based on plasma drug concentrations but also on environmental exposures that may influence immune activation.
Chronic exposure to air pollution can activate the inflammatory system and increase oxidative stress, contributing to the development of atherosclerosis and elevating the risk of acute coronary syndromes.7 Proximity to traffic roads may disrupt physiological homeostasis through both exposure to airborne particulate matter and excessive noise. Environmental noise is increasingly recognized as a stressor that can impair auditory, neurological, endocrine, and cardiovascular function.8 Mehrizi et al8 postulated that noise‑induced production of pro‑inflammatory cytokines—such as interleukin‑1, interleukin‑6, and tumor necrosis factor—may lead to the overproduction of reactive oxygen species via nicotinamide adenine dinucleotide phosphate oxidase activation.
Traffic‑related pollutants include carbon monoxide, nitrogen oxides, particulate matter (PM; PM2.5 and PM10), volatile organic compounds, and sulfur and carbon dioxide. Inhalation of combustion‑related pollutants can elicit localized immune responses and systemic effects, including bone marrow stimulation, resulting in the release of polymorphonuclear leukocytes and mobilization of monocytes.9
Previous studies10 have identified ambient nitrogen dioxide and PM10 as potential contributors to myocardial injury, acting as chemoattractants for monocytes. The same analysis showed associations between environmental exposures (such as noise and air pollution) and upregulation of inflammatory markers, including CD40 ligand, matrix metalloproteinase 10, and vascular endothelial growth factor A.
Study limitations
The analysis was conducted on a relatively small cohort, and further research on a larger group of patients is advocated to confirm the presented hypothesis. Additionally, antibody titers, especially donor‑specific antibody monitoring, would be beneficial in future analyses.
The individualized geomaps were generated for each participant. Since none of the enrolled patients were professionally active during the study period, their place of residence was considered representative of long‑term habitation.
Conclusions
The risk of myocardial injury following heart transplantation may be associated with environmental factors, particularly the density of traffic roads within 300-, 500-, 700-, and 1000‑meter buffers. The surrounding residential environment may influence the immune system, especially in the context of immunosuppressive therapy. It seems that the overall density of traffic roads, rather than their classification type, may play a crucial role in this relationship.
- Peled Y, Ducharme A, Kittleson M, et al. International Society for Heart and Lung Transplantation Guidelines for the Evaluation and Care of Cardiac Transplant Candidates‑2024. J Heart Lung Transplant. 2024; 43: 1529‑1628.e54. | Crossref
- Refsnes M, Skuland T, Jørgensen R, et al. Role of different mechanisms in pro‑inflammatory responses triggered by traffic‑derived particulate matter in human bronchiolar epithelial cells. Part Fibre Toxicol. 2023; 20: 31‑48. | Crossref
- Zhang Q, Du X, Li H, et al. Cardiovascular effects of traffic‑related air pollution: a multi‑omics analysis from a randomized, crossover trial. J Hazard Mater. 2022; 435: 129031. | Crossref
- Talugula S, Nyenhuis SM, Eldeirawi K, et al. Proximity to traffic is associated with worse symptom severity in patients with chronic rhinosinusitis with nasal polyps. Am J Otolaryngol. 2025; 46: 104580. | Crossref
- Urbanowicz T, Skotak K, Olasińska‑Wiśniewska A, et al. Five‑year mortality disparities across urban and rural areas in patients treated with coronary artery bypass grafting. Pol Arch Intern Med. 2024; 134: 16847. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION