Epicardial cryoablation with a novel liquid nitrogen-based device and concomitant, bilateral cardiac sympathetic denervation on rescue venoarterial extracorporeal membrane oxygenation for electrical storm and cardiogenic shock



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Epicardial cryoablation with a novel liquid nitrogen-based device and concomitant, bilateral cardiac sympathetic denervation on rescue venoarterial extracorporeal membrane oxygenation for electrical storm and cardiogenic shock
Electrical storm (ES) may require advanced interventions beyond pharmacotherapy, including surgical ablation, bilateral cardiac sympathetic denervation (BCSD), and, in selected cases, venoarterial extracorporeal membrane oxygenation (VA ECMO) support.1-4 The first report of such a hybrid approach incorporating BSCD, VA ECMO support, and ventricular tachycardia (VT) ablation has become available only recently.5
A 66‑year‑old man with recurrent VT interrupted by multiple implantable cardioverter defibrillator shocks, chronic heart failure (ejection fraction <30%), and coronary artery disease was urgently transferred to a cardiac surgery department for BCSD. Earlier, he required electrical cardioversion and modification of antiarrhythmic treatment due to ES. Propafenone was used temporarily, and despite the diagnosis of postamiodarone hyperthyroidism, amiodarone was reintroduced in consultation with an endocrinologist. The patient’s medical history also included anterior wall myocardial infarction, percutaneous coronary intervention, postinfarction pseudoaneurysm of the heart apex, stereotactic radiotherapy targeting the arrhythmia substrate in the left ventricle, and multiple VT ablations (right ventricular apex, left and right ventricular outflow tract regions).
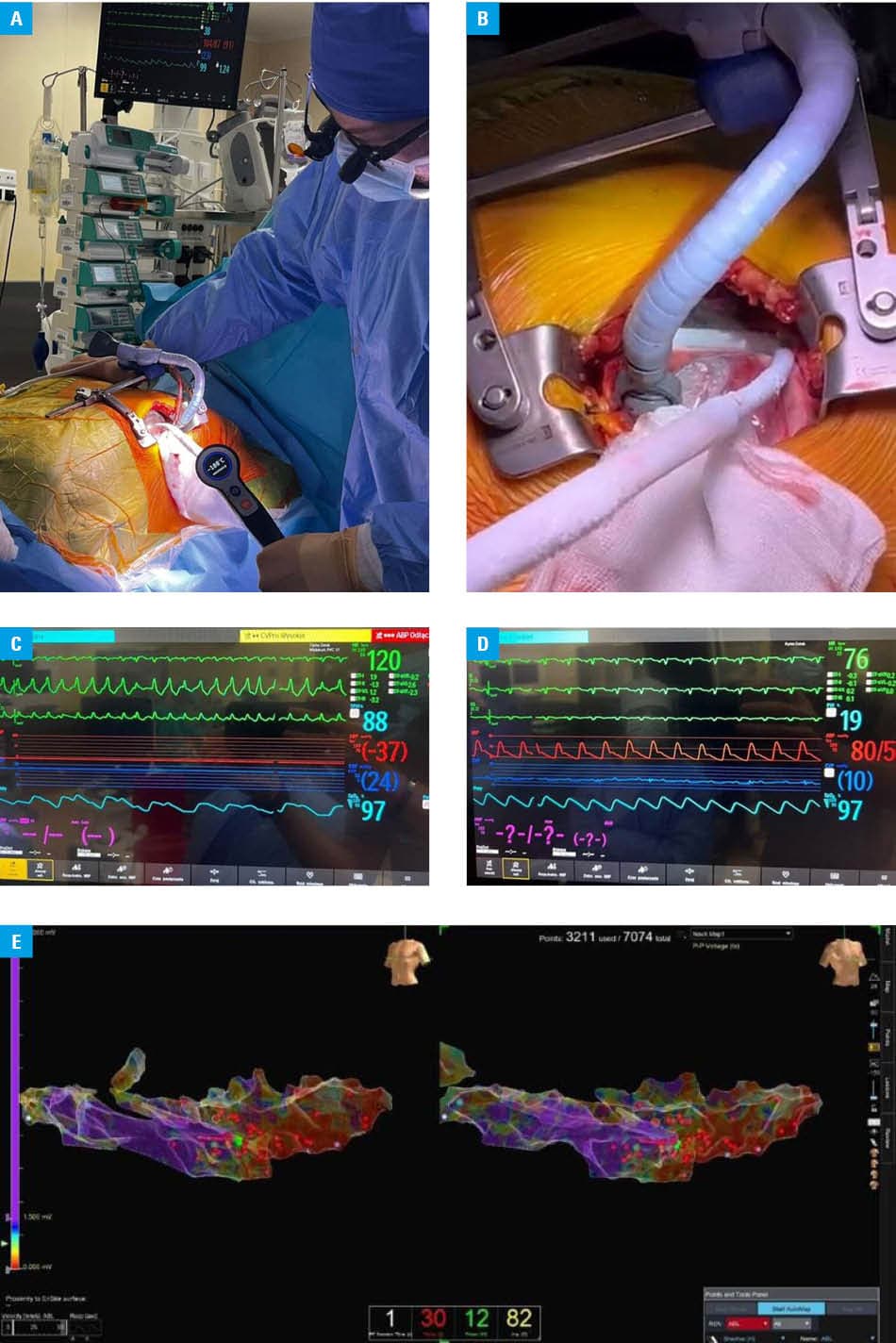
Upon admission to the operating room, the patient presented features of impending cardiogenic shock (blood pressure, 80/50 mm Hg), prompting urgent peripheral VA ECMO implantation. Then, BCSD was performed, followed by left anterior minithoracotomy and electrophysiology study (EPS)-guided cryoablation. The procedure utilized the CoolCryo device (CoolCryo, Medinice, Warsaw, Poland), which is approved by the Food and Drug Administration and pending CE mark within the European Union. The patient has signed informed consent for off‑label use, and a respective agreement for life‑saving use from the competent authority was acquired. Cryoablation was applied around the heart apex in the postinfarction scar region with 8 applications, 120 seconds each (Figure 1A and 1B). During incessant VT, sinus rhythm was restored within the second application (Figure 1C and 1D). Subsequently, the patient was weaned off V‑A ECMO. Following an uneventful postoperative period, the patient was transferred to a department of cardiology for further treatment and rehabilitation. Three months later, follow‑up EPS was performed with touch‑up VT ablation at the right ventricular apex and intraventricular septum (Figure 1E). At 6‑month follow‑up, the patient remained in a good condition with no recurrence of ES.
The case describes the first in Poland use of a novel surgical cryoablation system for the treatment of ES. It highlights promising results in the epicardial management of ventricular arrhythmias, as well as the importance of recognizing ES as a medical emergency that warrants prompt escalation and referral to specialized centers—a key consideration for internists and intensivists involved in early patient management.
The cryoablation CoolCryo device consists of a control console and single‑use cryoapplicators with moldable aluminum tips cooled with liquid nitrogen, enabling significantly faster procedures. Its advanced design allows for effective ablation of thick myocardial tissue, and it is suitable for use on a beating heart. Unlike with previous devices, surgeons can adjust cryoablation depth by setting the application time and freezing temperature.
- Zeppenfeld K, Tfelt‑Hansen J, De Riva M, et. al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022; 43: 3997‑4126. | Crossref
- Suwalski P, Stec S, Zienciuk‑Krajka A. Robotic bilateral cardiac sympathetic denervation in a patient with severe long QT syndrome: first experience in Poland. Kardiol Pol. 2023; 81: 644‑645. | Crossref
- Murtaza G, Sharma SP, Akella K, et al. Role of cardiac sympathetic denervation in ventricular tachycardia: a meta‐analysis. Pacing Clinical Electrophis. 2020; 43: 828‑837. | Crossref
- Vallabhajosyula S, Vallabhajosyula S, Vaidya VR, et al. Venoarterial extracorporeal membrane oxygenation support for ventricular tachycardia ablation: a systematic review. ASAIO. 2020; 66: 980‑985. | Crossref
- Kowalewski M, Stec S, Ogorzelec N, Suwalski P. Hybrid cardiac neuromodulation on veno‑arterial extracorporeal membrane oxygenation support in patients with recurrent electrical storm and end‑stage heart failure. Kardiol Pol. 2025; 83: 934‑936. | Crossref
ARTICLE INFORMATION