Real-life application of the European Society for Medical Oncology guidelines for the prevention and treatment of cancer-associated thrombosis: challenges and perspectives
Key words: cancer-associated thrombosis, oral direct anticoagulants, guidelines, low-molecular-weight heparin, risk assessment model

 CC BY 4.0
CC BY 4.0
Real-life application of the European Society for Medical Oncology guidelines for the prevention and treatment of cancer-associated thrombosis: challenges and perspectives
Cancer‑associated thrombosis (CAT) is the second leading cause of death in cancer patients, significantly affecting their quality of life, survival, and health care costs. This review summarizes key recommendations from the 2023 European Society for Medical Oncology guidelines on CAT prevention and treatment, illustrated by a real‑world case, and examines barriers to their implementation. CAT risk is multifactorial, shaped by tumor‑related factors (type, stage, time since diagnosis), treatment exposures (anticancer agents, surgery, central venous catheters), and comorbidities, captured by the “4TS” rule. Emerging biomarkers (eg, D‑dimer, thrombin generation, coagulome genes) and oncogenic mutations may refine risk stratification. The guidelines recommend routine assessment using models such as the Khorana score, COMPASS‑CAT, or Vienna‑CATS, with COMPASS‑CAT demonstrating superior predictive accuracy for patients with breast, lung, ovarian, or colon cancer. For high‑risk ambulatory patients, thromboprophylaxis is recommended for up to 6 months, with regular reassessment of risk thereafter. Treatment of CAT favors low‑molecular‑weight heparin or oral direct FXa inhibitors (apixaban, edoxaban, rivaroxaban), with incidental venous thromboembolism managed similarly to symptomatic events. The API‑CAT study supports low‑dose apixaban (2.5 mg twice a day) as a safer long‑term treatment. Screening for antiphospholipid antibodies guides therapeutic strategies. Major challenges for optimization of the antithrombotic treatment include renal impairment, thrombocytopenia, and treatment adherence. Oral direct FXa inhibitors may improve quality of life. Effective CAT management requires individualized care, strong clinician–patient communication, and education. The guideline implementation remains suboptimal. Closing the gap demands national strategies promoting health‑provider training, patient empowerment, e‑health applications, equitable access, and dedicated CAT outpatient clinics for sustained, personalized care.
Introduction
Therapeutic advances in oncology have transformed many types of cancers into chronic diseases; however, cancer–associated thrombosis (CAT) remains a significant health care burden. Although it is a preventable disease, with an annual incidence of up to 20% among patients with active cancer, CAT is the second leading cause of mortality in cancer patients after cancer itself. It affects both the quality of life (QoL) and the life expectancy of patients and is a significant financial burden for health care systems.1-4
Epidemiologic data underscore the magnitude of the problem, emphasizing the urgent need for effective risk stratification and prophylactic measures5,6: 1) patients with active cancer face a 3- to 9‑fold higher risk of venous thromboembolism (VTE), as compared with the general population; 2) occult cancer is identified in 4% to 9% of patients with unprovoked VTE. In the 6 months preceding a cancer diagnosis, the overall VTE incidence raises up to 18.6 per 1000 person‑years, being significantly higher in comparison with 3.2 per 1000 person‑years in controls. This 6‑fold increase in the thrombotic risk further escalates up to 10‑fold in the 6 months following diagnosis and remains 8‑fold higher at 1 year after diagnosis; 3) cancer patients who develop CAT have a 4- to 6‑fold higher mortality rate than those without thrombosis; d) 70% to 80% of CAT events occur in the outpatient setting.
The rising incidence of CAT varies according to the type of cancer, and it is estimated to further increase in the coming years. The rise in CAT incidence is driven in part by an aging patient population, the increase in life expectancy, and the advent of targeted anticancer therapies, such as protein kinase inhibitors, antiangiogenics, and immunotherapies, which confer an about 2.5‑fold increased risk of VTE relative to conventional chemotherapy.7-10
CAT disrupts anticancer treatment by causing delays or modifications during high‑risk periods, and necessitates long‑term anticoagulation, thereby increasing bleeding risk and complicating overall cancer care.11-13 During the first 3 months following symptomatic VTE, the high risk of recurrence often forces delays or changes in cancer treatment or surgery. These adjustments may worsen disease outcomes, raising the risk of treatment resistance, disease progression, or recurrence.14
The economic burden of CAT is substantial. Each hospitalization episode incurs costs ranging from 5000 to 15 000 EUR. As the risk of VTE increases, total health care expenditures rise accordingly, driven by the need for long‑term anticoagulation, bleeding management, and extended follow‑up care. About 16%–28% of patients with CAT require hospitalization for recurrence, occurring 2 to 3 times more frequently than in patients with VTE alone. Overall, anticancer treatment costs are approximately 50% higher in patients with CAT than those without.15-22
The 2023 European Society for Medical Oncology (ESMO) guidelines offer updated, evidence‑based recommendations specifically adapted to the evolving landscape of cancer therapies.23 Despite availability of expert guidance, significant gaps persist in their clinical awareness and implementation, particularly in routine oncology practice.24-27
This review aims to contextualize the implementation of the most recent ESMO guidelines for the prevention and treatment of CAT, while identifying key barriers that hinder awareness and adherence. To support this objective, the rationale will be illustrated through a representative real‑life clinical case reflecting common challenges in everyday oncology practice.
A typical clinical case of metastatic breast cancer
A 52‑year‑old premenopausal woman with obesity (body mass index [BMI], 31 kg/m2), hypertension, and hypertriglyceridemia, residing in a rural zone, 80 km from a university hospital, presented with persistent back pain. Imaging showed bone lesions, and further diagnostic workup confirmed a diagnosis of de novo stage IV hormone receptor‑positive (HR+), HER2‑negative breast cancer with bone metastases. The hematological workup yielded hemoglobin of 12.8 g/dl (reference range [RR], 12–15.5 g/dl), platelet count of 450 G/l (RR, 150–400 G/l), and white blood count of 6.8 G/l (RR, 4–10 G/l).
Primary diagnosis and first‑line anticancer treatment
Histopathological analysis identified invasive ductal carcinoma (grade 2, estrogen receptor [ER] 90%, progesterone receptor [PR] 10%, HER2 2+/ISH–) in the breast and a concordant profile in a bone lesion (ER+, PR–, HER2–). The patient underwent bilateral salpingo‑oophorectomy and mastectomy for removal of the primary tumor. Since she underwent abdominal cancer surgery, in accordance with the recommendations (Table 1), she received postoperative thromboprophylaxis with enoxaparin 4000 IU once daily for 30 days. First‑line systemic therapy was initiated with aromatase inhibitor letrozole and zoledronic acid (bisphosphonate).
Options | Hospitalized patients | Surgical patients | Ambulatory patients |
a Lack of a specific indication for cancer outpatients in the package inserts
b The use of DOACs in this setting, including extended thromboprophylaxis for 4 weeks after discharge, is currently not recommended since the reduction of VTE compared with standard heparin prophylaxis was offset by an increase in major bleeding.
c Some patients may have a contraindication for mechanical prophylaxis (eg, patients with peripheral limb ischemia).
Abbreviations: bid, twice daily; CrCl, creatinine clearance; DOAC, direct oral anticoagulant; GCS, graduated compression stockings; LMWH, low‑molecular‑weight heparin; IPC, intermittent pneumatic compression; od, once daily; UFH, unfractionated heparin; VTE, venous thromboembolism; Xa, activated factor X | |||
Heparins (UFH/LMWH) | |||
UFH, IU | 5000 every 8 h | 5000, 2–4 h preoperatively and every 8 h thereafter | – |
Bemiparin, anti‑Xa IU | 3500 od | 3500, starting 2 h preoperatively or 6 h postoperatively and 3500 od thereafter | 3500 od |
Dalteparin, anti‑Xa IU | 5000 od | 5000, 12 h preoperatively and 5000 thereafter | 5000 od |
Enoxaparin, anti‑Xa IU | 4000 od | 4000, 12 h preoperatively and 4000 od thereafter | 4000 odb |
Nadroparin, anti‑Xa IU | 3800 od (if weight >70 kg, 5700 od) | 2850, 2–4 h preoperatively and 2850 od thereafter | 3800 od (if weight >70 kg, 5700 oda |
Tinzaparin, anti‑Xa IU | 4500 od | 4500 od, beginning 12 h postoperatively | 4500 oda |
Selective parenteral indirect factor Xa inhibitor | |||
Fondaparinux | 2.5 mg od 1.5 mg od in patients with CrCl 20–50 mg/dl | 2.5 mg od beginning 6–8 h postoperatively | Not studied in the outpatient prophylaxis setting |
DOAC | |||
Apixaban | Not recommendedb | Not recommended | 2.5 mg orally bida |
Rivaroxaban | Not recommendedb | Not recommended | 10 mg orally oda |
Mechanical prophylaxis | |||
IPC device | If pharmacological VTE prophylaxis is contraindicatedc | If pharmacological VTE prophylaxis is contraindicatedc | Not recommended |
Venous foot pump | If pharmacological VTE prophylaxis is contraindicatedc | If pharmacological VTE prophylaxis is contraindicatedc | Not recommended |
GCSs | If pharmacological VTE prophylaxis is contraindicatedc | If pharmacological VTE prophylaxis is contraindicatedc | Not recommended |
Diagnosis of cancer progression and second- and third‑line treatment
Approximately 2 years later, the patient developed bone disease progression and was treated with second‑line fulvestrant (ER antagonist) in combination with palbociclib (cyclin‑dependent kinase 4/6 inhibitor). After about 5 years since the initial diagnosis, she experienced further disease progression involving bone and liver metastases, and third‑line therapy with everolimus‑exemestane (mammalian target of rapamycin inhibitor and steroidal aromatase inhibitor, respectively) was commenced.
Cancer progression and asymptomatic venous thromboembolism
Six months into this treatment, progression of liver metastases was documented. Core‑needle biopsy revealed decreased ER expression (50%), complete loss of PR expression (0%), and a HER2 1+ status. A computed tomography (CT) scan performed at that time showed asymptomatic partial thrombosis of the right common and internal iliac veins, with no evidence of pulmonary embolism (PE). Therapeutic‑dose tinzaparin was initiated, and fourth‑line therapy with capecitabine was introduced.
Residual cancer disease
Six months later, follow‑up imaging showed a partial tumor response and no clinical or radiological signs of recurrent VTE. Tinzaparin was discontinued and replaced by oral apixaban at 5 mg twice daily.
Venous thromboembolism in breast cancer: epidemiologic insights and risk stratification challenges
Breast cancer is generally considered a low‑risk malignancy for VTE, both in surgical settings and among outpatients receiving standard anticancer therapies. However, the association between breast cancer and VTE is significant and often underestimated.28
This perception stems from the low incidence observed in unselected cohorts. In a population‑based study using data from the California Cancer Registry and Patient Discharge Data Set (1993–1999), the 2‑year cumulative VTE incidence among 108 255 patients with breast cancer was 1.2%, with rates of 1.2 and 0.6 events per 100 patient‑years during the first and second half‑year, respectively.29 However, this incidence was still significantly higher than in the general population (standardized incidence ratio, 4.2; 95% CI, 3.9–4.4).
In‑hospital data further underscore the clinical burden of CAT, showing mortality rates of about 7.4% for acute deep vein thrombosis (DVT) and 8% for PE in breast cancer patients with VTE.30 Independent predictors of VTE included older age (hazard ratio [HR], 2 for >75 vs <45 years), at least 3 comorbidities (HR, 2.9 vs none), and metastatic disease (HR, 6.3 vs localized). Without administration of thromboprophylaxis, VTE incidence generally increases with advanced cancer stage; a review by Wun et al31 estimated breast cancer VTE incidence over 1 year as approximately 0.6% at a local stage, rising to 2.8% in metastatic disease.
The histological type of breast cancer is a significant determinant of VTE risk. In a prospective cohort of 1762 patients with invasive breast cancer or ductal carcinoma in situ undergoing breast surgery (mastectomy or lumpectomy, with or without axillary surgery and / or immediate reconstruction), the incidence of symptomatic, objectively confirmed VTE—including DVT and / or PE—was 0.9%.31 The presence of intrinsic risk factors, particularly cardiovascular risk factors, further amplified VTE risk. In the non‑VTE group, invasive ductal carcinoma was the predominant histological subtype. Notably, the patients who received neoadjuvant chemotherapy had lower VTE incidence than those who did not (0.2% vs 1.2%; P = 0.048).32
A recent prospective study in breast cancer patients undergoing surgery without pharmacologic thromboprophylaxis reported a 6‑month cumulative incidence of symptomatic, confirmed VTE, including superficial vein thrombosis (SVT), lower‑extremity DVT, central venous catheter–related thrombosis (CRT), upper‑extremity DVT, and PE, approaching 20%. Approximately 9% of VTE events (mainly lower‑extremity SVT and DVT) occurred during hospitalization. One‑month postsurgery, CRT emerged as the most frequent VTE type.33 In another retrospective cohort of 52 457 women surgically treated for breast cancer, 395 (0.8%) were diagnosed with VTE during their index hospitalization or within 90 days of discharge. Most of the VTE cases (67.1%) were diagnosed after discharge from the hospital. The mean and median number of days between hospital discharge and VTE diagnosis was 26.2 and 13, respectively.34
Anticancer agents and venous thromboembolism risk in breast cancer
Breast cancer patients have an approximately 6% annual risk of VTE while undergoing chemotherapy, which is about 10.8 times higher than women without cancer during the same period. For breast cancer patients receiving systemic therapies, such as cyclin‑dependent kinase inhibitors, reported VTE rates are up to 5%–9% during median follow‑up of 18.5 months.35 Targeted anticancer agents show cumulative VTE incidences of 11% at 6 months and 13% at 12 months.36
Endocrine therapy with tamoxifen is associated with a substantially increased risk of VTE, approximately doubling the risk in comparison with pretreatment levels. Several large clinical trials have consistently demonstrated that aromatase inhibitors (AIs) are associated with a significantly lower risk of VTE, as compared with tamoxifen in breast cancer patients. The ATAC trial (Arimidex, Tamoxifen Alone or in Combination; n = 9366) showed a VTE rate of 2.8% with anastrozole vs 4.5% with tamoxifen (P = 0.0004), while the BIG 1–98 trial (Letrozole or Tamoxifen in Treating Postmenopausal Women with Breast Cancer; n = 8010) reported a 1.5% VTE rate with letrozole vs 3.5% with tamoxifen (P <0.001). The TEAM trial (Exemestane as Treatment in Adjuvant for Post‑Menopausal Patients with Non‑Metastatic Breast Cancer; n = 9779) found only a 1% VTE rate in patients receiving exemestane vs 2% in those receiving tamoxifen followed by exemestane (P <0.0001). These findings suggest that AIs may be preferable to tamoxifen in patients at an increased risk for thromboembolic events.37-39
Table 2 summarizes the mechanisms of action and the associated VTE risk of the anticancer agents administered to the patient described in the clinical case.
Drug | Mechanism of action | VTE risk | VTE risk classification |
Abbreviations: CDK4/6, cyclin‑dependent kinases 4 and 6; mTOR, mammalian target of rapamycin; mTORC1, mammalian target of rapamycin comple × 1; others, see Table 1 | |||
Letrozole | Aromatase inhibitor, blocks conversion of androgens to estrogens lowering estrogen levels | Lower risk of VTE (1.5%) vs tamoxifen (4.5%) | Low to moderate |
Fulvestrant | Estrogen receptor antagonist, degrades and blocks estrogen receptor signaling | Approximately 2.8% incidence in trials | Low to moderate |
Zoledronic acid | Bisphosphonate, inhibits osteoclast‑mediated bone resorption | No significant direct VTE risk reported | Low |
Palbociclib | CDK4/6 inhibitor, blocks cyclin‑dependent kinases 4 and 6 inhibiting cell cycle progression | Reported VTE risk varies but up to around 10%, notably higher than endocrine therapies alone | Moderate to high |
Everolimus | mTOR inhibitor, reduces cell growth and proliferation by inhibiting mTORC1 | VTE not commonly reported as major side effect | Low |
Exemestane | Steroidal irreversible aromatase inhibitor, causes irreversible inhibition of aromatase | Similar to other aromatase inhibitors; lower VTE risk than with tamoxifen | Low |
The consistent reduction in VTE risk observed across multiple trials and with various AIs should not be interpreted as an absence of risk associated with these treatments, as VTE remains a clinically relevant concern.
These data highlight that although the overall VTE risk in breast cancer is generally low, there is significant interpatient variability. Effective prevention and management require individualized risk stratification, considering factors such as tumor histology, cancer stage, time since diagnosis (primary diagnosis, recurrent disease, or disease progression), type of anticancer treatment, and the presence of comorbidities or cardiovascular risk factors, all of which influence thrombotic risk.
Contextualized application of guidelines for the prevention of cancer‑associated thrombosis
At initial diagnosis, the patient presented with de novo metastatic HR+/HER2− breast cancer and cardiovascular risk factors, both recognized as risk factors for VTE. In addition, she received treatment with letrozole, which is associated with a low‑to‑moderate risk of VTE. Despite multiple risk factors, the patient was not assessed for VTE risk and did not receive pharmacologic thromboprophylaxis at cancer diagnosis, during first‑line therapy, or at subsequent progression and initiation of second- and third‑line treatments.
Assessment of cancer‑associated thrombosis risk at cancer diagnosis and recommendations for thromboprophylaxis
Routine pharmacologic thromboprophylaxis is not recommended for all cancer outpatients scheduled to or receiving anticancer therapy. The overall rate of symptomatic VTE does not justify universal prophylaxis, and the risk of bleeding—especially in patients with cancer‑related complications, such as thrombocytopenia, renal impairment, or liver toxicity—may outweigh potential benefits.
The risk of CAT is multifactorial, shaped by cancer‑specific factors, such as its type and stage, time since diagnosis or recurrence, and the anticancer / supportive therapies (ie, chemotherapy, targeted anticancer therapy, radiotherapy, surgery, erythropoietin, etc, and the use of central venous catheters),40 summarized as the “4TS” rule, as well as patient‑specific characteristics and comorbidities, such as cardiovascular disease or risk factors (ie, diabetes, hypertension, obesity, and dyslipidemia), personal history of VTE, previous recent hospitalization, etc.
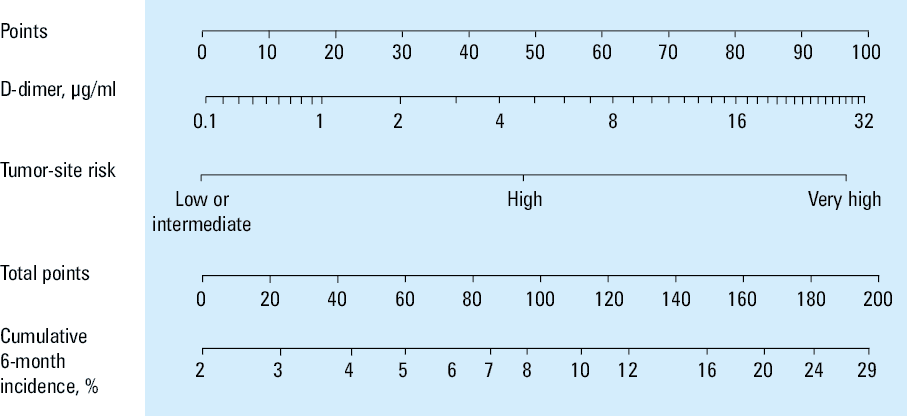
Personalized risk assessment using validated risk scores, such as the COMPASS‑CAT41 (Table 3), the Vienna‑CATS42 (Figure 1), or the Khorana risk score (KRS; Table 4),43 are recommended by the 2023 ESMO guidelines.23
Predictors for VTE | Score |
a Risk scores corresponding to the patient profile outlined in the clinical case
Abbreviations: CVC, central venous catheter; others, see Table 1 | |
Cancer‑related risk factors | |
Antihormonal therapy for women with hormone receptor–positive breast cancer or on anthracycline treatment | 6a |
Time since cancer diagnosis ≤6 months | 4a |
CVC | 3 |
Advanced stage of cancer | 2a |
Predisposing risk factors | |
Cardiovascular risk factors
(composed of at least 2 of the following predictors: personal history of peripheral artery disease, ischemic stroke, coronary artery disease, hypertension, hyperlipidemia, diabetes, obesity) | 5a |
Recent hospitalization for acute medical illness | 5 |
Personal history of VTE | 1 |
Biomarkers | |
Platelet count ≥350 G/l | 2a |
Score ≥7: high risk (rate of VTE >10%) | 19a |
Khorana risk score | Points |
a Risk scores corresponding to the patient profile outlined in the clinical case
b Total score is calculated by adding points for each criterion in the model.
Abbreviations: see Table 1 | |
Patient characteristic | |
Prechemotherapy platelet count ≥350 G/l | 1 |
Hemoglobin level <10 g/dl or use of red cell growth factors | 1 |
Prechemotherapy leukocyte count >11 G/l | 1 |
Body mass index ≥35 kg/m2 | 1 |
Site of cancer | |
Very high risk (stomach, pancreas) | 2 |
High risk (lung, lymphoma, gynecologic, bladder, testicular, renal) | 1 |
Interpretationb | |
High risk (VTE rate, 6.7%–12.9%) | ≥3 |
Intermediate risk (VTE rate, 1.8%–4.8%) | 1–2 |
Low risk (VTE rate, 0.3%–1.5%) | 0a |
Emerging biomarkers, such as elevated D‑dimer level, abnormal thrombin generation, shortened procoagulant phospholipid‑dependent clotting time (Procoag‑PPL), and an increase in podoplanin level, along with certain genetic variations in coagulation pathway genes (coagulome genes), and oncogenic mutations and rearrangements have been linked to increased CAT risk, and may help refine risk stratification beyond clinical factors alone.44-48 Prospective observational studies are essential to pinpoint the most clinically relevant biomarkers for identifying cancer patients at a high risk of thrombosis who may benefit from pharmacologic thromboprophylaxis.
Among the biomarkers discussed, D‑dimers are the most easily accessible and routinely assessed. They are incorporated into the Vienna‑CATS score as a predictive factor.42 However, current evidence does not support the routine use of D‑dimers or any other biomarker for tailoring thromboprophylaxis or assessing its efficacy.49 In this context, artificial intelligence and machine learning approaches are expected to play a key role in generating more accurate clinical‑biological risk prediction models.
Recent experimental evidence shows that in tumor microenvironment, the procoagulant fingerprint of cancer cells affects the activation of endothelial cells and the formation of fibrin clot network, which acts as a protective shield against anticancer agents and also as a scaffold that facilitates cancer cell migration within the clot.50,51 Biomarkers or global coagulation assays informative for fibrin clot structure, function, permeability, and lysability, might be meaningful in the evaluation of cancer‑associated hypercoagulability and related thrombotic risk.52
Accuracy of the risk assessment models for cancer‑associated thrombosis
At the time of cancer diagnosis and prior to initiating the first‑line treatment, the COMPASS‑CAT score41 yielded a total of 19 points, classifying the patient as high‑risk for VTE. In contrast, the KRS43 yielded only 1 point, placing the patient in the low‑risk category. Assessment using the Vienna‑CATS score42 was not feasible in this case due to unavailability of baseline D‑dimer measurements, which are required for its calculation.
The COMPASS‑CAT score was specifically developed using data from a large prospective cohort of 1355 ambulatory patients with breast, lung, colorectal, or ovarian cancer, and was subsequently externally validated in more than 3800 patients with the same cancers. The KRS emphasizes the tumor type, making it less sensitive to individual risk factors, such as comorbidities, treatment modalities, and cancer progression dynamics that are integral to the COMPASS‑CAT model. In addition, the derivation cohort of the COMPASS‑CAT study prospectively enrolled outpatients either before treatment initiation or during different phases of anticancer therapies, whereas the KRS was derived from a retrospective analysis of a cohort formed before any anticancer treatment administration. These characteristics explain the higher sensitivity of the COMPASS‑CAT score in identifying high‑risk patients with breast, lung, colorectal, or ovarian cancer in real‑world outpatient oncology settings, and support its use throughout the entire oncological care pathway, both before and during anticancer therapy.53 Recent meta‑analyses of 13 studies comprising 8665 patients confirm the robust predictive performance of COMPASS‑CAT (sensitivity, 0.76; area under the curve, 0.77), with superior accuracy in comparison with KRS, particularly in identifying high‑risk patients with diverse cancers. The addition of hypercoagulability (eg, Procoag‑PPL, thrombin generation) and inflammatory biomarkers (eg, interleukin 10) further enhances its prognostic utility.54-56
The COMPASS‑CAT is particularly valuable for assessing patients with common cancers in real‑world clinical practice.57
Primary prevention of cancer‑associated thrombosis in high‑risk outpatients with active cancer undergoing anticancer therapy
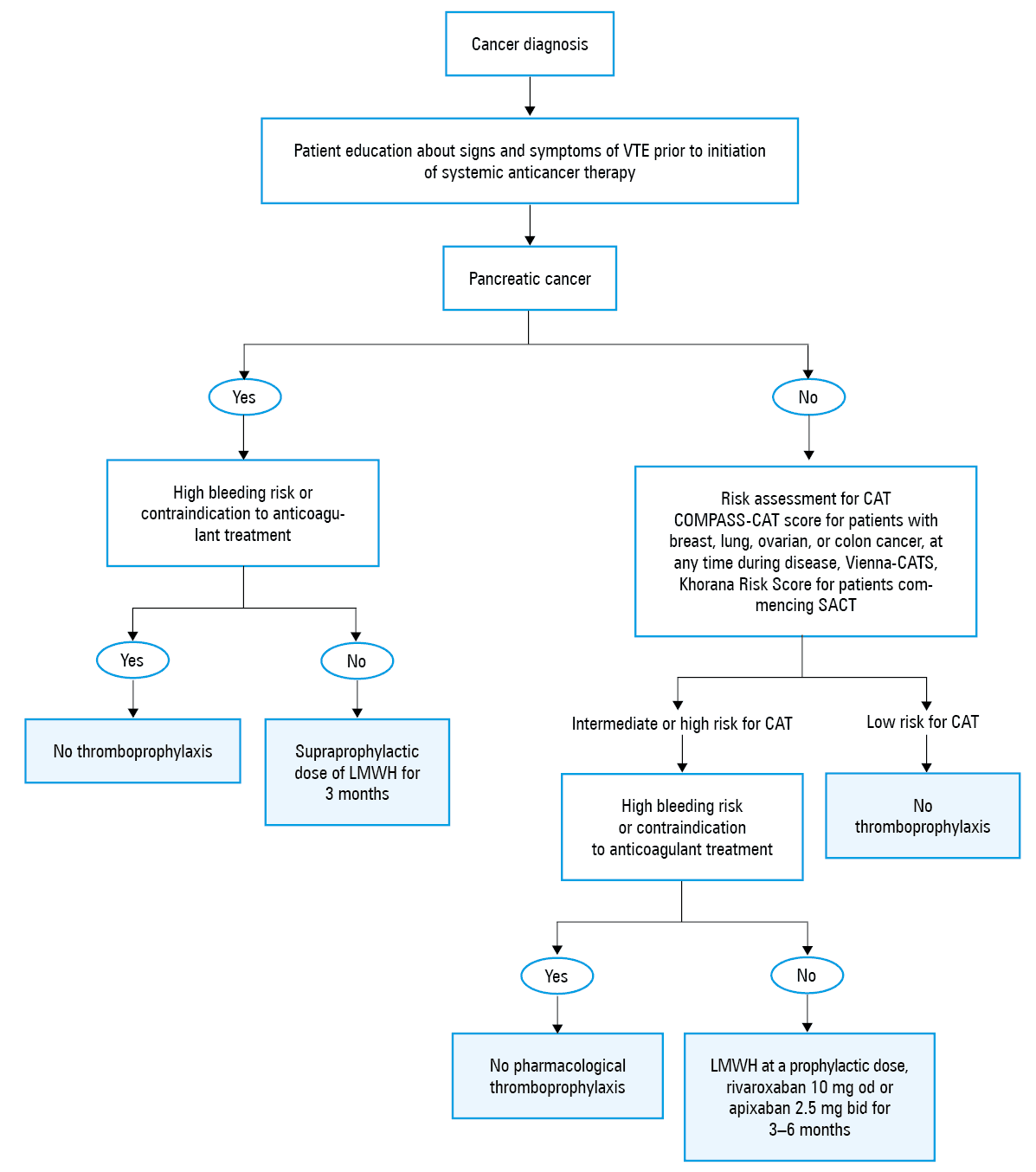
According to the COMPASS‑CAT risk assessment model, the patient was consistently classified as high‑risk for CAT throughout the entire disease course—from the initial diagnosis and first‑line therapy to each documented progression and subsequent treatment line. In alignment with the 2023 ESMO guidelines (Figure 2), pharmacologic thromboprophylaxis with either low‑molecular‑weight heparin (LMWH), or specific oral direct FXa inhibitors, such as apixaban or rivaroxaban (Table 1), would be recommended at cancer diagnosis and for up to 6 months following initiation of the first‑line therapy. Reassessment after each progression, specifically at the start of the second- and third‑line treatments, would justify renewed thromboprophylaxis for an additional 6‑month period, given the sustained high‑risk profile.23
Treatment of cancer‑associated thrombosis
While on the third‑line treatment and cancer progression, being at a high risk for CAT without thromboprophylaxis, incidental DVT (partial thrombosis of the right common and internal iliac veins, with no evidence of PE) was diagnosed on a routine CT scan in the discussed patient.
Incidental venous thromboembolism in cancer: clinical impact and management
The 12‑month incidence of incidental VTE in active cancer patients ranges from 4.5% to 9.7%, depending on cancer type and stage. Importantly, incidental diagnoses account for 20% to 50% of all VTE events in this population, typically identified during routine imaging for disease staging or treatment monitoring. Incidental VTE is clinically significant, being associated with unfavorable outcomes, including a 6% risk of recurrence within 1 year and a 30‑day mortality rate approaching 10%.58-60
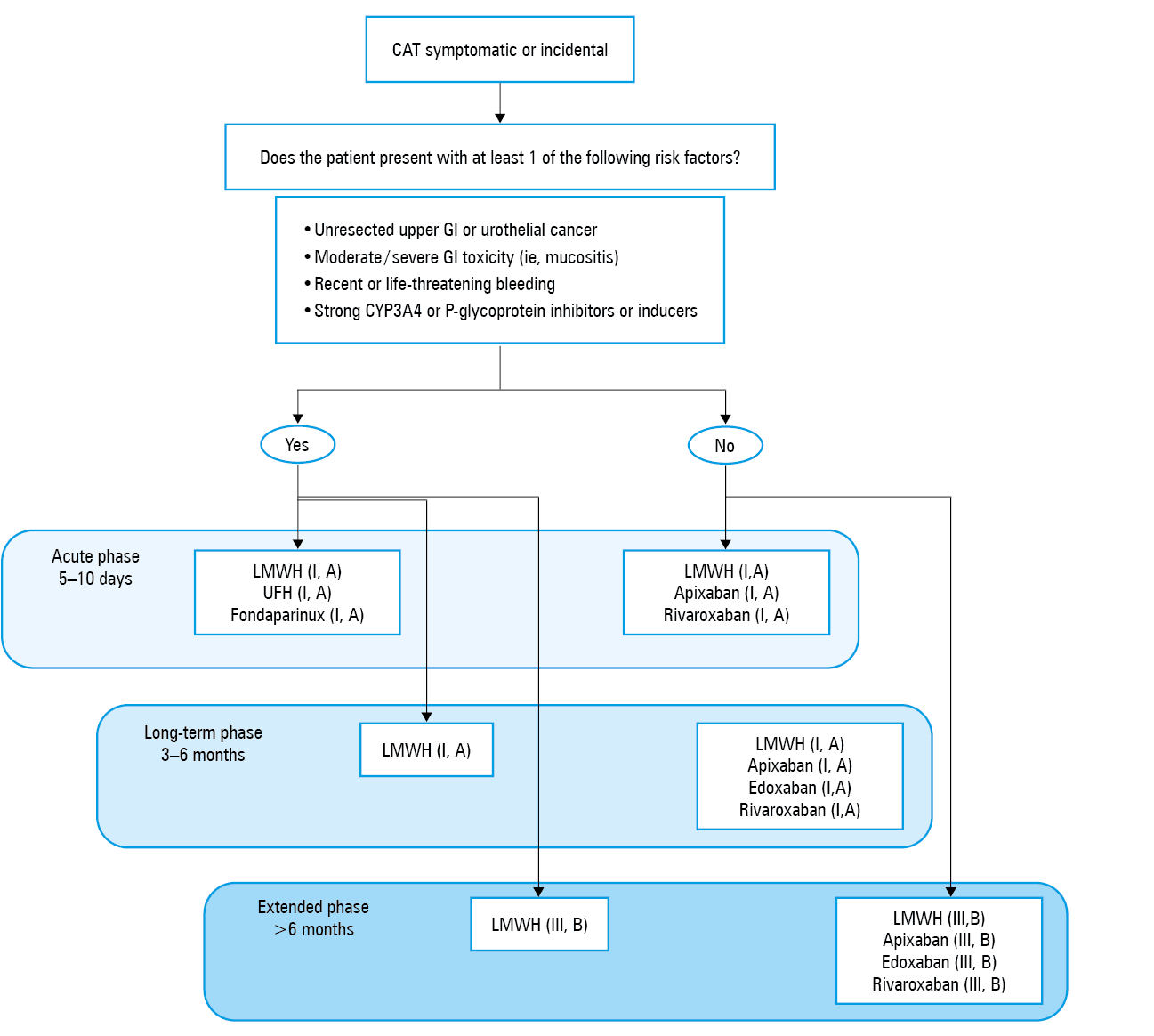
According to 2023 ESMO guidelines, the same treatment with therapeutic doses of LMWH or FXa inhibitors is recommended for incidentally detected VTE as for symptomatic VTE (Figure 3; Table 5).
Drug | Initial treatment of established VTE (5–10 days) | Long‑term phase (first 3–6 months) and extended phase (beyond 6 months) |
a According to the results of the APICAT trial61
Abbreviations: aPTT, activated partial thromboplastin time; INR, international normalized ratio; iv, intravenous; others, see Table 1 | ||
Heparins (LMWH/UFH) | ||
Dalteparin, anti‑Xa IU/kg | 100 every 12 h, or 200 od for the first 30 days | 150 od after day 30 |
Enoxaparin, anti‑Xa IU/kg | 100 every 12 h, or 150 od | 100 every 12 h, or 150 od |
Tinzaparin, anti‑Xa IU/kg | 175 od | 175 od |
Nadroparin, anti‑Xa IU/kg | 86 every 12 h, or 171 od | 86 every 12 h, or 171 od |
Bemiparin, anti‑Xa IU/kg | 115 od | 115 od |
UFH, IU/kg | 80 iv bolus, then 18 h iv; adjust dose based on aPTT | – |
DOACs | ||
Edoxaban | Therapeutic doses of parenteral anticoagulant (tLMWH or UFH or fondaparinux) for at least 5 days | 60 mg, od 30 mg, od if: 1) CrCl <50 ml/min, 2) weight ≤60 kg, or 3) patients receiving P‑glycoprotein inhibitors |
Rivaroxaban, mg | 15 every 12 h for 3 weeks | 20 od |
Apixaban, mg | 10 every 12 h for 7 days | 5 every 12 h
2.5 every 12 h after the first 6 months from the diagnosis of VTE and the initiation of the acute phase treatmenta |
Vitamin K antagonists | ||
Acenocoumarol | – | Adjust dose to maintain INR 2–3 |
Phenprocoumon | – | Adjust dose to maintain INR 2–3 |
Warfarin | – | Adjust dose to maintain INR 2–3 |
The patient received the recommended treatment with LMWH, tinzaparin, for 6 months, and subsequently switched to apixaban 5 mg twice daily. The duration of the antithrombotic treatment is determined by the presence of active cancer and the administration of anticancer therapy.
A dose of apixaban can be optimized. A multicenter randomized, double‑blind, noninferiority APICAT trial (API‑CAT STUDY for Apixaban Cancer Associated Thrombosis) compared the efficacy and safety of apixaban at a reduced (2.5 mg) or full (5 mg) dose twice daily for 12 months in 1766 patients with active cancer and proximal DVT or PE who had completed at least 6 months of anticoagulant treatment.61 Median treatment duration was 11.8 months. Recurrent VTE occurred in 2.1% of the patients on reduced‑dose apixaban and 2.8% of those on full‑dose (adjusted subhazard ratio, 0.76; P = 0.001 for noninferiority). Clinically relevant bleeding was lower with reduced‑dose (12.1%) vs full‑dose (15.6%) treatment (adjusted subhazard ratio, 0.75; P = 0.03). Mortality was similar (17.7% vs 19.6%). Reduced‑dose apixaban (2.5 mg twice daily) proved noninferior for VTE prevention and safer in terms of bleeding, supporting its use as a long‑term treatment option. The favorable benefit‑risk profile of the reduced apixaban dose (2.5 mg twice daily) has been also observed in a single‑center study by Weronska et al.62
Key factors in optimizing antithrombotic therapy
Patients on antithrombotic treatment for CAT face both increased risk of VTE recurrence and bleeding. The 1‑year VTE recurrence rates after discontinuation of anticoagulant therapy range from 13% to over 20% for patients with cancer vs 6%–7% in noncancer patients. In addition, the risk of CAT recurrence during antithrombotic treatment is high. The SELECT‑D study (Anticoagulation Therapy in Selected Cancer Patients at Risk of Recurrence of Venous Thromboembolism) showed a HR of about 3.2 (95% CI, 1.9–5.4) for recurrence in cancer patients, as compared with noncancer ones, despite antithrombotic therapy.63 The risk of major bleeding in cancer patients receiving antithrombotic therapy is about 2- to 3‑fold higher than in noncancer patients.64,65 The risks of VTE recurrence and bleeding in CAT patients are influenced by multiple dynamic factors, such as cancer localization and progression, hypercoagulability, drug absorption, and drug‑to‑drug interactions as well as by side effects of anticancer therapy (ie, thrombocytopenia, anemia, thrombocytopathy induced by drug myelotoxicity, etc.). Patient traits (age, frailty, obesity) and hematologic parameters also affect the risk.
The tumor location plays a crucial role in selecting an antithrombotic agent. Patients with gastrointestinal cancer have a 2- to 4‑fold higher risk of clinically relevant bleeding when treated with oral direct FXa inhibitors, as compared with LMWH.23 Frequent, thorough reassessment, even at primary health care units, is essential for optimal management of patients receiving antithrombotic treatment for CAT.
Antiphospholipid syndrome
In patients with CAT, it is important to screen for antiphospholipid syndrome (APS), as its presence is associated with a high risk of recurrence after discontinuation of antithrombotic therapy.51 Identifying APS in patients with CAT is therefore essential for optimizing treatment strategies and determining the appropriate type, dose, and duration of the antithrombotic therapy. APS, a key prothrombotic condition in cancer patients, is defined by the occurrence of thrombosis in the presence of at least 1 antiphospholipid antibody (aPL)—lupus anticoagulant (LA), anticardiolipin (aCL), anti-β2‑glycoprotein I (anti-β2GPI)—or, less commonly, nonconventional antibodies, such as antiprothrombin antibodies. The aPL positivity is higher in cancer patients, up to 18% vs 9% in noncancer patients, and is associated with an increased thrombotic risk. The presence of aPL antibodies raises by 3- to 4‑fold the risk of VTE or arterial thrombosis. In triple‑positive patients (LA, aCL, anti-β2GPI), direct oral anticoagulants (DOACs) are not advised due to their lower efficacy. Long‑term LMWH remains the preferred treatment for cancer patients with APS. Screening for aPL is thus essential before switching to oral direct FXa inhibitors.51
Renal impairment
Cancer patients with renal dysfunction face an elevated risk of major bleeding and VTE recurrence during antithrombotic therapy. In moderate renal impairment (creatinine clearance [CrCl], 30–60 ml/min), available data indicate that LMWH and FXa inhibitors offer similar efficacy and safety as in patients with normal renal function. However, patients with severe renal impairment (CrCl <30 ml/min) were excluded from pivotal trials. For these patients, treatment options include unfractionated heparin followed by vitamin K antagonists (VKAs) or LMWH at adjusted doses and monitoring of plasma levels of FXa activity at 4 hours after a subcutaneous injection. However, as for other indications, oral direct FXa inhibitors may be used with caution in patients with severe renal impairment and CrCl equal to or below 15 ml/min.66,67
Obesity
In patients with extreme obesity (>120 kg or BMI >40 kg/m²), LMWH dosing should be based on actual body weight; though the upper threshold recommended by the manufacturer has to be respected. While no major efficacy or safety issues have been observed with FXa inhibitors in this group of patients, their use should remain cautious in individuals weighing over 120 kg due to limited data.23
Thrombocytopenia
For cancer patients with platelet count below 50 G/l, management of the antithrombotic agents depends on thrombosis risk. In high‑risk cases (within 30 d of acute VTE or with proximal DVT/PE), full‑dose LMWH may be combined with platelet transfusions to maintain counts above 40–50 G/l.68 For lower‑risk scenarios, reduced‑dose LMWH is an option, with temporary cessation if platelets fall below 25 G/l. Full‑dose LMWH can be resumed if platelet counts are above 50 G/l. Data on the use of oral direct FXa inhibitors in this setting remain insufficient.
ESMO recommendations for specific groups of patients are summarized in Figure 2.
Management of cancer‑associated thrombosis and quality of life
The patient was diagnosed with advanced‑stage breast cancer and experienced progressive disease. From the time of initial diagnosis, she was classified at a high risk for CAT, making her eligible for long‑term pharmacologic thromboprophylaxis with LMWH or oral direct FXa inhibitors. Following the occurrence of VTE, long‑term therapeutic anticoagulation was indicated. Treatment adherence is a critical factor for the success of antithrombotic therapy.
QoL is of major importance in CAT management and adherence to treatment. Patients face physical and psychological distress from cancer, therapies, thrombosis, and hospitalizations. Long‑term treatment with LMWH or oral direct FXa inhibitors is a standard of care and is generally well tolerated. LMWH may even improve QoL when bleeding is controlled, and many patients find daily injections acceptable.69
A recent systematic literature review of 21 studies (from 2009 to 2024) evaluating patient satisfaction with VKAs, DOACs, and LMWHs showed that DOACs consistently improved treatment adherence and QoL, largely due to their oral route and ease of administration.70
The QoL is also shaped by factors such as disease progression, residual thrombosis, cardiovascular comorbidities, and bleeding risk, which remains a major concern during prolonged therapy. Commonly used QoL assessment tools, such as the 36‑Item Short Form Health Survey and European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 lack specificity for CAT, underlining the need for more targeted, patient‑centered evaluation.
A strong physician–patient relationship is essential to successfully applying thromboprophylaxis recommendations and ensuring adherence to the antithrombotic treatment for CAT. Patient attitude toward medical information and treatment can vary widely depending on cultural background, ranging from passive acceptance to active engagement or even denial. While distress related to CAT may be limited, lack of knowledge often affects acceptability of LMWH therapy. This has important implications for anticoagulant choice, particularly as FXa inhibitors are now a validated therapeutic option.71,72
Ultimately, individualized therapeutic strategies led by skilled, communicative clinicians are critical. Integrating patient satisfaction into decision‑making can improve adherence, optimize QoL, and enhance overall treatment outcomes.
Awareness, guideline implementation, and barriers to management of cancer‑associated thrombosis
The patient resides in a rural zone, 80 km from the university hospital; she is on antithrombotic treatment and needs regular specialized follow‑up.
The recommended frequency of follow‑up consultation in patients with CAT on antithrombotic treatment is not rigidly defined in all guidelines,73,74 but several key principles apply.
Follow‑up during anticoagulant therapy requires structured planning. In the initial phase (first weeks), frequent monitoring is needed to evaluate tolerability, detect clinical signs of bleeding, reinforce adherence, and review injection technique in the case of treatment with LMWH. During the first 3–6 months, monthly reviews are recommended to assess treatment efficacy, side effects, renal function, platelet count, and cancer progression. After 6 months, if antithrombotic therapy continues, follow‑up may occur every 3–6 months, but regular reassessment of the thrombotic and bleeding risk remains essential.
Follow‑up is often conducted in specialized centers, posing logistic and financial challenges, especially for patients living in remote areas, such as islands and mountainous regions. These difficulties include long travel times, limited access to specialized care, and substantial out‑of‑pocket expenses. The impact of health care system organization becomes evident when comparing countries. For example, in France, where public health coverage is robust, annual CAT‑related follow‑up costs are approximately 400 EUR per patient and are largely reimbursed by the national health insurance. In contrast, in Greece, where the public health care system has been severely weakened and health care is largely privatized and fragmented, costs range from approximately 600 EUR on the mainland to over 1500 EUR in remote areas, with expenses predominantly paid out‑of‑pocket by patients.75-81
These disparities highlight the importance of strong public health care system in ensuring equitable access to care and reducing the financial burden of chronic disease management for cancer patients with CAT. The organization and strength of the public health care system play a critical role in mitigating these burdens.
Raising awareness and enhancing implementation of cancer‑associated thrombosis guidelines—an unmet need
Effective implementation of guidelines for the prevention and treatment of CAT is crucial not only for improving patient outcomes but also for reducing health care costs, both at the macroeconomic level and in terms of individual and family financial burden.
Yet, in Europe and North America adherence remains suboptimal. Only 40%–60% of hospitalized cancer patients receive thromboprophylaxis, and in outpatient settings, this rate is just 10%–25%. Similarly, while 60%–70% of inpatients with CAT are treated as per guidelines, only 30%–60% of outpatients receive appropriate care.82-87
ESMO reports that most oncologists underestimate CAT risk—often due to limited awareness or training. Martin et al86 conducted a retrospective study in pancreatic and gastric cancer patients and found that none of the high‑risk individuals received thromboprophylaxis. Over 90% of oncologists rarely assessed CAT risk, and 67% were unfamiliar with the risk models or guideline‑based prophylaxis.
Patients also show low awareness. The ROADMAP‑CAT‑Awareness study (Prospective Risk Assessment and Management of Patient with CAT) found that only 30% of the public and only 40% of cancer patients were aware of CAT risk, with just 25% recognizing VTE symptoms. Only 35% of informed patients learned about CAT from a physician, underscoring a gap in clinician–patient education.88
Integrated care pathways and national strategies for cancer‑associated thrombosis management
Equitable, free access to medical services for all citizens remains a cornerstone of patient care. Longitudinal, dispensary‑based surveillance, reinforced by dynamic follow‑up and supported by digital tools, is essential for managing CAT over the course of cancer care. To effectively bridge the gap between scientific evidence and clinical practice, a comprehensive national strategy for CAT management is essential. It should be flexible enough to adapt to diverse social, economic, and cultural contexts. This strategy must operate across all levels of health care. At the primary health care level, priorities include education of medical professionals, education of patients and the members of their social environment, development of multidisciplinary care networks, systematic identification of high‑risk patients at cancer diagnosis, and development of e‑health and telemedicine to ensure continuity of care and decrease the impact of geographic and financial barriers. Within hospital settings, staff training, risk‑based routine prevention, and personalized treatment protocols are essential. Structured long‑term anticoagulation management must be ensured, through dedicated thrombosis consultations and specialized outpatient clinics to support shared decision‑making and organize networks of expert centers with the primary health care structures in rural and defavorized areas and populations. Additionally, a strong partnership between health care providers, citizens, and stakeholders is important in a comprehensive campaign for prevention and optimal treatment of CAT according to the guidelines.
Concluding remarks
CAT remains underrecognized despite its significant impact on survival and patient QoL, as well as on the health care costs. ESMO recommends: 1) thromboprophylaxis with LMWH for patients undergoing oncological surgery; 2) routine risk assessment using the COMPASS‑CAT or the Vienna‑CATS scores, or the KRS. High‑risk ambulatory patients should receive thromboprophylaxis with LMWH or oral direct FXa inhibitors (apixaban, rivaroxaban) for up to 6 months; 3) treatment with therapeutic dose of LWMH or oral direct FXa inhibitors (apixaban, edoxaban, rivaroxaban) for patients with symptomatic or incidental VTE. The optimal duration of the treatment is principally determined by the state of cancer and the bleeding risk. Oral direct FXa inhibitors improve QoL. For long‑term treatment of CAT, a low‑dose regimen of apixaban (2.5 mg twice daily) is safe and as effective as the standard dose (5 mg twice daily).
Careful evaluation of the localization of cancer, regular monitoring of the platelet count and renal function, as well as screening for APS are essential steps for optimization of antithrombotic therapy.
Awareness among oncologists and patients is limited, and structured CAT education is lacking. Fragmented care, unequal service access, and socioeconomic disparities worsen the problem. A coordinated, patient‑centered approach and updated decision support tools are needed. In this respect, the World Thrombosis Day markedly increases CAT awareness among physicians, patients, health care stakeholders, and the general population.89,90 The VAS European Independent Foundation is dedicated to play a central role in advancing this mission.
- Khorana AA, Francis CW, Culakova E, et al. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007; 5: 632‑634. | Crossref
- Dewilde S, Janssen MF, Lloyd AJ, et al. Exploration of the reasons why health state valuation differs for children compared with adults: a mixed methods approach. Value Health. 2022; 25: 1185‑1195. | Crossref
- Khorana AA. Venous thromboembolism and prognosis in cancer. Thromb Res. 2010; 125: 490‑493. | Crossref
- Weitz JI, Haas S, Ageno W, et al. GARFIELD‑VTE investigators. Cancer associated thrombosis in everyday practice: perspectives from GARFIELD‑VTE. J Thromb Thrombolysis. 2020; 50: 267‑277. | Crossref
- van Es N, Le Gal G, Otten HM, et al. Screening for cancer in patients with unprovoked venous thromboembolism: protocol for a systematic review and individual patient data meta‑analysis. BMJ Open. 2017; 7: e015562. | Crossref
ARTICLE INFORMATION