Internal hernias are an uncommon and often challenging cause of small bowel obstruction. In surgical patients, they particularly affect Roux‑en‑Y (RY) reconstructions (bariatric and oncologic). Petersen hernia involves the herniation of small bowel loops through the mesenteric defect arising between the Roux limb and the transverse mesocolon, referred to as the Petersen space. Although the overall prevalence after gastrectomy is low (0.2%–5.6%), Petersen hernia is particularly prone to bowel ischemia and necrosis due to delayed diagnosis. Risk factors include laparoscopic access, rapid postoperative weight loss, low body mass index, and the failure to close mesenteric defects during primary operation.1-4
A 59‑year‑old man was admitted to an emergency department with acute epigastric pain, nausea, and postprandial discomfort persisting for several days. The patient had a medical history of poorly differentiated, intestinal‑type gastric adenocarcinoma involving the gastroesophageal junction (ypT2N0M0), treated with perioperative fluorouracil, leucovorin, oxaliplatin, and docetaxel chemotherapy, total gastrectomy with D2 lymphadenectomy, and RY reconstruction 6 months prior.
Physical examination showed epigastric tenderness and abdominal distension without peritoneal signs. Laboratory investigations, including inflammatory marker assessment, were within normal limits. Contrast‑enhanced abdominal computed tomography (CT) identified swirling of the mesenteric vessels (“whirl sign”), suggestive of an internal hernia with small bowel volvulus, without evidence of peritoneal metastases or local cancer recurrence (Figure 1A–1C).
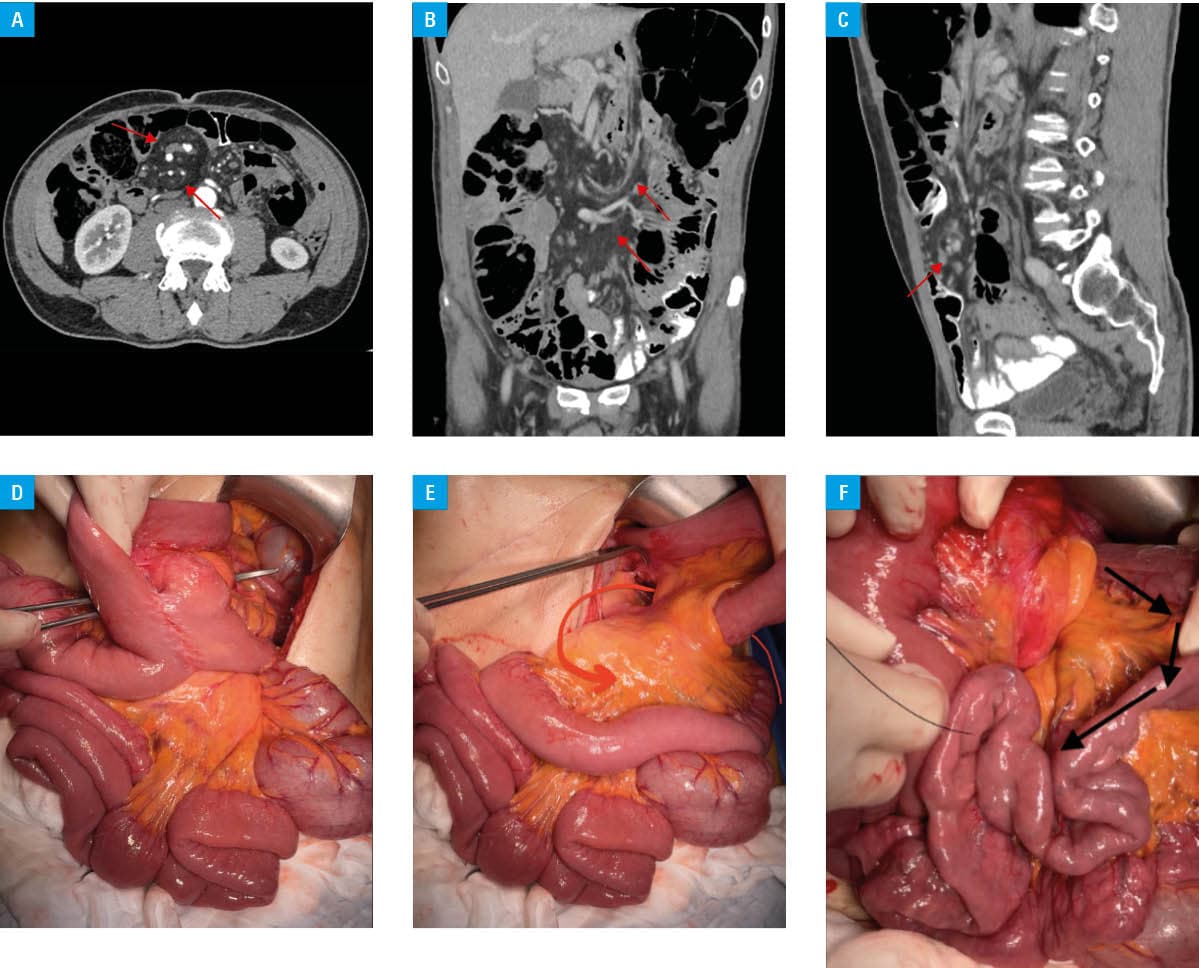
The patient underwent emergency laparotomy. Intraoperatively, Petersen hernia was diagnosed, with small bowel herniating through the mesenteric defect between the Roux limb and the posterior abdominal wall, resulting in volvulus but without signs of ischemia. The herniated loops were reduced, adhesiolysis was performed, and the mesenteric defect was closed. No tumor recurrence was noted (Figure 1D–1F).
Postoperative recovery was uneventful. Oral feeding was resumed on the first postoperative day. The patient was discharged in a good condition and complication‑free.
Petersen hernia often presents with nonspecific symptoms, including recurring abdominal pain, nausea, early postprandial fullness, and signs of intermittent small bowel obstruction. Normal laboratory results and nonacute abdomen do not exclude a life‑threatening condition after surgery. These nonspecific features frequently delay diagnosis, contributing to increased morbidity. It demands vigilance from internists and emergency physicians. CT remains the diagnostic modality of choice, with the whirl sign being a characteristic and sensitive finding.3 Petersen hernia should be included in the differential diagnosis of small‑bowel obstruction after RY reconstruction, alongside more common causes, such as adhesions, peritoneal carcinomatosis, and local tumor recurrence.
Surgical management involves prompt reduction of the herniated bowel and closure of the mesenteric defect. In the cases with ischemia, bowel resection may be necessary. Preventive closure of mesenteric defects during initial surgery is highly recommended. Studies have shown that this procedure significantly reduces the risk of internal herniation.2,4,5
Petersen hernia is an uncommon but potentially fatal complication that can present late after gastrectomy with vague gastrointestinal symptoms. A high index of suspicion is warranted in postgastrectomy patients, even when laboratory results are normal and peritoneal signs are absent. Early CT, with recognition of the characteristic mesenteric whirl sign, followed by prompt surgical consultation, are crucial to prevent intestinal ischemia.
This case highlights the need for vigilance among internists and primary care physicians, and the importance of routine inclusion of Petersen hernia in the differential diagnosis of small‑bowel obstruction after RY reconstruction.
- Sun K, Wu Y. Current status of internal hernia after gastrectomy for gastric cancer. Langenbecks Arch Surg. 2022; 407: 99‑104. | Crossref
- Kang K, Cho Y, Min S, et al. Internal hernia after gastrectomy for gastric cancer in minimally invasive surgery era. Gastric Cancer. 2019; 22: 1009‑1015. | Crossref
- Doishita S, Takeshita T, Uchima Y, et al. Internal hernias in the era of multidetector CT: correlation of imaging and surgical findings. Radiographics. 2016; 36: 88‑106. | Crossref
- Han W, Eom B, Yoon H, et al. Clinical characteristics and surgical outcomes of internal hernia after gastrectomy in gastric cancer patients: retrospective case control study. Surg Endosc. 2019; 33: 2873‑2879. | Crossref
- Murakami K, Obama K, Kanaya S, et al. Mesenteric closure after laparoscopic total gastrectomy with Roux‑en‑Y reconstruction is effective for prevention of internal hernia: a multicenter retrospective study. Surg Endosc. 2022; 36: 4181‑4188. | Crossref
ARTICLE INFORMATION