We present a case of a 60‑year‑old man with type 2 diabetes (T2D) and obesity who presented with rapidly deteriorating renal function and hypercalcemia, without albuminuria. Renal biopsy demonstrated oxalate nephropathy: intratubular crystals confirmed by birefringence under polarized light as calcium oxalate. It was subsequently discovered that he had been self‑medicating with orlistat and supratherapeutic doses of vitamins C and D3. Via interactions between different mechanisms of electrolyte metabolism, these nonprescription agents very nearly led to this patient requiring renal replacement therapy.
This case demonstrates the importance of establishing over‑the‑counter medication use as part of a medical assessment. In a world where these medications are being increasingly accessed over the internet, it also highlights the risks and potential interactions which may occur with lack of professional oversight.
A 60‑year‑old man with T2D and obesity was referred to a nephrology department by his diabetes physician due to declining renal function in the absence of albuminuria. His estimated glomerular filtration rate (eGFR) had fallen from above 60 ml/min/1.73 m2 to 33 ml/min/1.73 m2 (reference range [RR] >60 ml/min/1.73 m2) in 1 year. He reported intentional weight loss of 27 kg over the same period and his glycemic control had significantly improved.
On initial nephrology clinic assessment, his eGFR had fallen further to 22 ml/min/1.73 m2 despite being asymptomatic and appearing systemically well. Urinalysis was normal. He was also noted to have hypercalcemia (serum calcium 2.85 mmol/l; RR, 2.2–2.65 mmol/l).
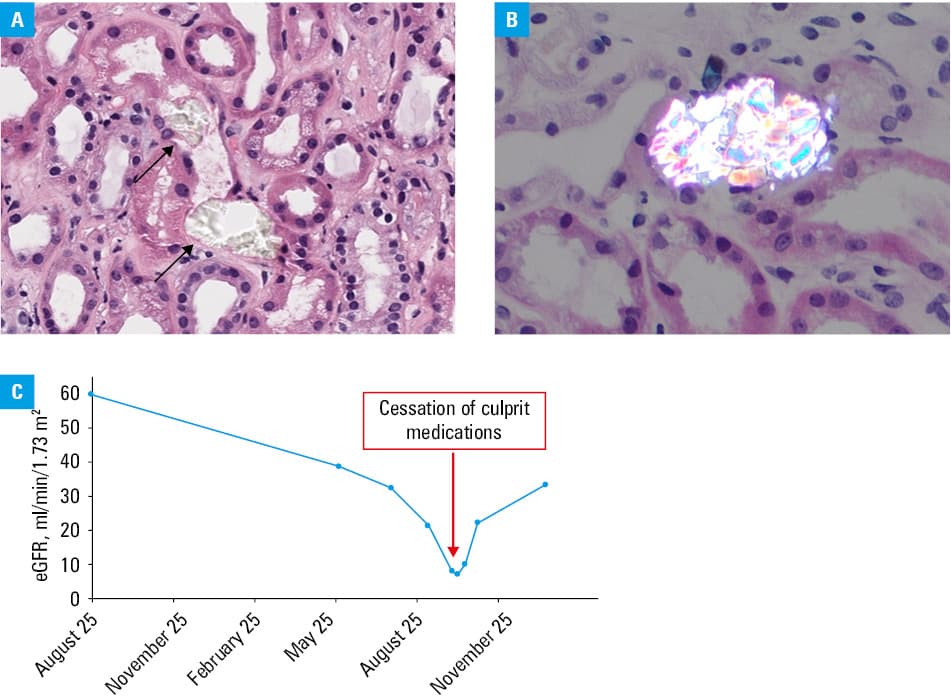
Renal biopsy was performed 3 weeks later. It showed oxalate nephropathy—calcium oxalate crystals deposited in the lumens of the kidney tubules (Figure 1A and 1B).
Upon questioning after the biopsy result, the patient reported having been buying orlistat, an intraluminal lipase inhibitor, over the internet as an aid in the weight loss process. He also declared the use of a large number of vitamin supplements which he had been buying from a high street health shop. These were calculated to include supratherapeutic dosages of 2440 mg of vitamin C and 13 200 units of vitamin D3 daily. It was suspected that these medications, in combination, were the underlying cause of his oxalate nephropathy.
The over‑the‑counter orlistat and vitamin supplements were stopped. The patient was closely monitored and the following week, eGFR reached a nadir of 8 ml/min/1.73 m2, and uremic symptoms developed. A plan was put in place to commence hemodialysis the following week if the patient continued to deteriorate, but thankfully his renal function began to improve. His eGFR value reached 34 ml/min/1.73 m2 3 months later and has remained at this level chronically (Figure 1C).
The association between orlistat use and secondary hyperoxaluria is well established, based on increased presence of dietary fats in the intestinal lumen, binding free calcium ions. This reduces the availability of calcium ions to bind to dietary oxalate in the gut, leading to increased absorption of free oxalate. This in turn reduces the proportion of dietary oxalate excreted fecally and increases urinary oxalate excretion.1
In this case, supratherapeutic intake of vitamin C and vitamin D3 appears to have played a synergistic role. Vitamin C (ascorbic acid) is partially metabolized to oxalic acid in the intracellular compartment,1 leading to increased urinary oxalate concentration. Therefore, supratherapeutic oral intake of vitamin C is a risk factor for oxalate nephropathy, independent of orlistat use.2 Supratherapeutic intake of vitamin D3 promotes increased intestinal calcium absorption and osteoclastic bone resorption, leading to further reduction in the availability of luminal calcium, hypercalcemia (as demonstrated in this case), and hypercalciuria. In the case of this patient, hypercalciuria, alongside the hyperoxaluria caused by orlistat and vitamin C ingestion, will have contributed to tubular supersaturation of calcium oxalate and subsequent pathological crystallization.1
The culprit over‑the‑counter medications in this case were bought both on the internet and in a high street health shop. Despite being available without prescription, these agents have caused this patient significant irreversible morbidity in the form of chronic kidney disease (CKD), narrowly avoiding dialysis. The use of the internet to access medications is becoming more prevalent around the world,3 so it is important for health care professionals to be aware that nonprescription medications, even vitamin supplements, have the propensity to interact with each other and may cause severe harm.
In addition, as this case demonstrates, patients may not offer the information that they are using over‑the‑counter medications of their own volition. This may be due to assumptions that they are harmless or a presumption that medical professionals will disapprove of their use, both of which the patient in this case reported. History‑taking should therefore include a nonjudgmental exploration of unprescribed medication and substance use.
This patient’s glycemic control had improved significantly due to his weight loss, assisted by orlistat. It is a shame that it came at the cost of CKD, and the overall impact on his cardiovascular risk is therefore uncertain. Glucagon‑like peptide‑1 (GLP‑1) receptor agonists improve glycemic control and weight management in T2D,4 while also demonstrating cardiovascular and renoprotective benefits.5 These agents should therefore be recommended for managing obesity in patients with T2D, in preference to alternatives, such as orlistat.
Orlistat use may become more common as the role of medications in weight loss becomes more widely recognized. Its potentially nephrotoxic interaction with vitamin C supplementation should be acknowledged by health care professionals, and safer alternatives, such as GLP‑1 receptor agonists, should be offered to eligible patients.
Over‑the‑counter medication use is prevalent and increasing, as they can be easily accessed over the internet. This case demonstrates even though their purchase does not require a prescription, these medications may cause significant harm. Information about nonprescription medication and substance use should be actively sought from patients.
- Rosenstock JL, Joab TMJ, DeVita MV, et al. Oxalate nephropathy: a review. Clin Kidney J. 2021; 15: 194‑204. | Crossref
- Knight J, Madduma‑Liyanage K, Mobley JA, et al. Ascorbic acid intake and oxalate synthesis. Urolithiasis. 2016; 44: 289‑297. | Crossref
- Sánchez‑Sánchez E, Fernández‑Cerezo FL, Díaz‑Jimenez J, et al. Consumption of over‑the‑counter drugs: prevalence and type of drugs. Int J Environ Res Public Health. 2021; 18: 5530. | Crossref
- Yao H, Zhang A, Li D, et al. Comparative effectiveness of GLP‑1 receptor agonists on glycaemic control, body weight, and lipid profile for type 2 diabetes: systematic review and network meta‑analysis. BMJ. 2024; 384: e076410. | Crossref
- Badve SV, Bilal A, Lee MMY, et al. Effects of GLP‑1 receptor agonists on kidney and cardiovascular disease outcomes: a meta‑analysis of randomised controlled trials. Lancet Diabetes Endocrinol. 2025; 13: 15‑28. | Crossref
ARTICLE INFORMATION