De novo type 1 diabetes in a patient with lupus nephritis treated with steroids and a history of proximal venous thrombosis

 CC BY 4.0
CC BY 4.0
De novo type 1 diabetes in a patient with lupus nephritis treated with steroids and a history of proximal venous thrombosis
Chronic glucocorticoid therapy, commonly used across many specialties, increases the risk of numerous diseases, including diabetes and venous thromboembolism.1,2 Steroid‑induced diabetes can occur de novo or as an exacerbation of pre‑existing hyperglycemia.1 Effective management includes insulin therapy, often in combination with metformin, and reducing steroid dose.3 This case highlights 2 key diagnostic challenges: thrombosis as a complication and difficulty in diagnosing diabetes. Although chronic glucocorticoid use typically suggests steroid‑induced diabetes, this case report demonstrates the need for broader diagnostic consideration in certain clinical contexts.
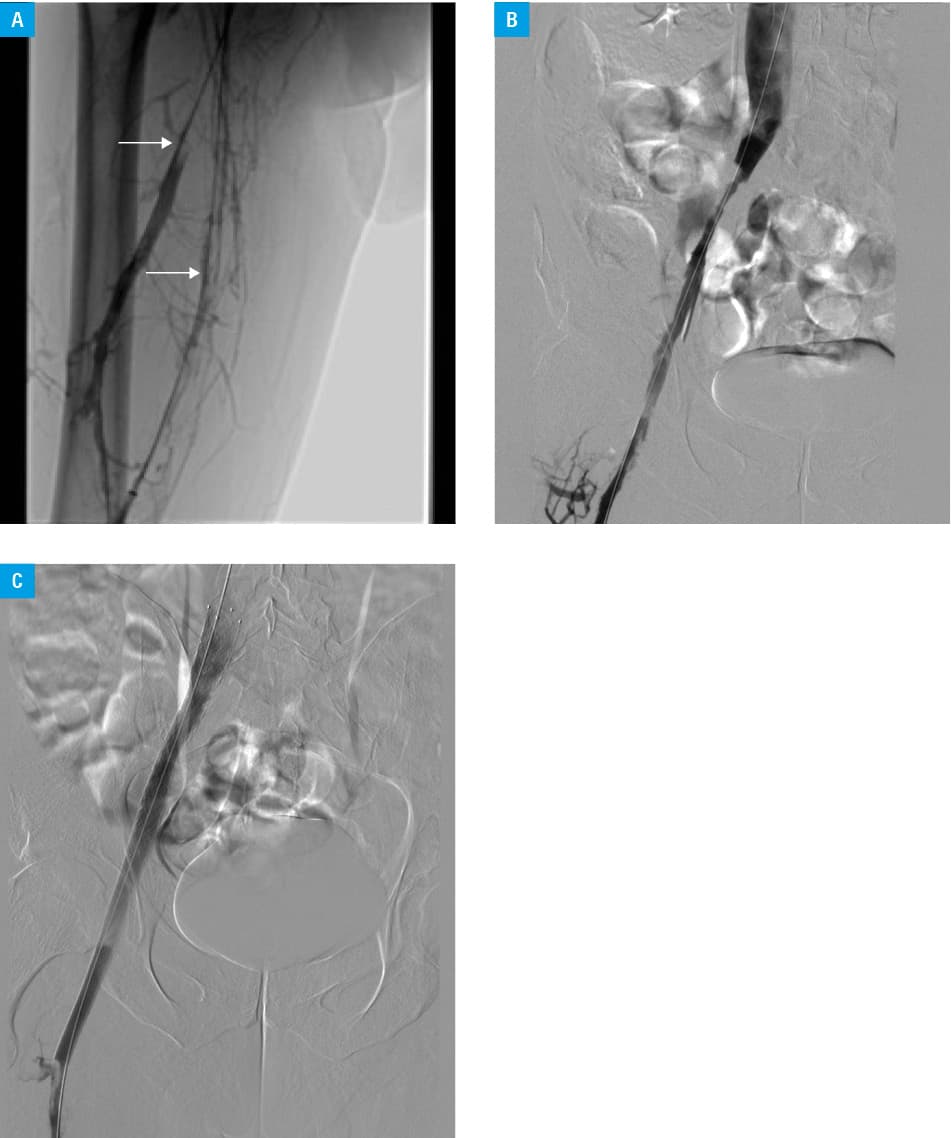
A 28‑year‑old man with a 9‑year history of class IV lupus nephropathy was admitted to evaluate nephrotic syndrome treatment. Previously, he was treated with prednisone (10–60 mg/day), mycophenolate mofetil (1250 mg/day), and chloroquine (250 mg/day). A month before hospitalization in a nephrology department, the patient was admitted to an angiology department due to proximal deep‑vein thrombosis of the right lower limb, involving the common iliac vein, external iliac vein, common femoral vein, deep femoral vein, and popliteal vein, which was treated with stenting and thrombectomy using the Lightning 12 system (Penumbra, Alameda, California, United States; Figure 1A–1C). Upon admission, the patient presented with several weeks of increased thirst, polyuria, and worsening visual acuity. In addition to typical nephrotic syndrome abnormalities, such as hypercholesterolemia, hypoalbuminemia, and massive proteinuria, laboratory tests identified fasting hyperglycemia (438 mg/dl; reference range [RR], 70–99 mg/dl). Urine analysis showed the presence of ketones, although no signs of acidosis were found on the blood gas analysis. The patient body mass index was 24 kg/m².
A diabetic consultation was requested, during which the diagnostic workup was expanded to include the measurement of fasting C‑peptide levels and testing for antiglutamic acid decarboxylase (anti‑GAD) antibodies. The glycated hemoglobin (HbA1c) level was 11.7% (RR, 4.4%–5.7%), C‑peptide was at the lower end of the normal range, and the anti‑GAD antibody result was positive.
Based on this, type 1 diabetes (T1D) was diagnosed, and a basal‑bolus insulin regimen was initiated (12 units of glargine, 4–6 units of lispro before meals), along with a continuous glucose monitoring system. Prednisone was reduced to 10 mg daily, and mycophenolate mofetil was increased to 2 g daily. Planned kidney biopsy was postponed for 6 months due to recent thrombosis and rivaroxaban use. Tests for antiphospholipid syndrome and genetic thrombophilias were performed, with results pending.
One month later, the patient was admitted for insulin dose education. The level of HbA1c was 8.4%, with 90% time‑in‑range. The C‑peptide level was slightly below normal.
Patients with autoimmune diseases on immunosuppressants may develop hyperglycemia in various ways. Distinguishing between T1D and steroid‑induced diabetes is crucial, as it guides treatment. Steroid‑induced diabetes, in contrast to T1D, is not caused by an autoimmune process, but results from insulin resistance and increased hepatic gluconeogenesis combined with impaired glucose uptake by muscles and adipose tissue.4 At the molecular level, recent studies highlight the role of Krüppel‑like factor 9 and its hepatic induction as a mechanism underlying steroid‑induced diabetes.5 The risk of developing diabetes increases with the length of therapy and the average daily steroid dose.4 Diagnosis is made using general diagnostic criteria for diabetes, without elevated islet autoantibodies or reduced C‑peptide levels.1 The disease develops gradually and is often detected during routine glucose monitoring; hence, glucose levels should be regularly checked in patients taking high doses of glucocorticoids, defined as more than 20 mg of prednisone or its equivalent. The times of day when hyperglycemia occurs depend on the timing of steroid administration, and for the most common regimen of taking a fixed dose in the morning, hyperglycemia is typically observed from late morning to early evening, while nighttime and morning values, including fasting levels, are usually normal.1 Unlike T1D, steroid‑induced diabetes offers a broader range of therapeutic options, including diet, metformin, incretin‑based drugs, and insulin therapy, particularly recommended for significant hyperglycemia.2 Additionally, in some patients, glucose normalization after discontinuation of glucocorticoids eliminates the need for long‑term hypoglycemic treatment.1 The differences between T1D and steroid‑induced diabetes are summarized in Supplementary material, Table S1.
In this case, based on the initial history, hyperglycemia could have been mistakenly diagnosed as steroid‑induced diabetes. This would be supported by the patient’s chronic steroid use and the absence of ketoacidosis in the blood gas analysis. However, the presence of symptoms not fitting the typical steroid‑induced diabetes pattern, such as hyperglycemia present throughout the day, the presence of ketones in the urine, and the patient’s normal body weight, suggested a need for further diagnostic workup. Expanding the tests to include C‑peptide and anti‑GAD antibody measurements led to a change in diagnosis and an adjustment of further management.
Interestingly, although the patient did not ultimately develop steroid‑induced diabetes per se, another issue related to chronic steroid therapy, that is, venous thromboembolism, is evident in his history. This results from the prothrombotic effects of glucocorticoids. An increase in prothrombotic factors, such as factor VIII and von Willebrand factor, combined with a reduction in fibrinolytic activity due to elevated levels of plasminogen activator inhibitor, induces a hypercoagulable state, particularly in the first 30 days of therapy or with high doses. Despite factors promoting hypercoagulability, common in comorbidities and inflammatory states, this effect has also been demonstrated in healthy individuals, mainly through increased thrombin generation and coagulation factor levels.2
In the absence of clear guidelines, diagnosing steroid‑induced diabetes mainly relies on the clinical picture and patient history. When uncertain, testing C‑peptide and anti‑GAD antibodies is recommended. Misdiagnosis and inappropriate treatment can lead to potentially life‑threatening complications in a short period.
Furthermore, while chronic steroid therapy increases thromboembolism risk, genetic causes, antiphospholipid syndrome, or prothrombin gene mutation, should be considered in younger patients. Early identification allows for better prevention and treatment.
- Roberts A, James J, Dhatariya K. Joint British Diabetes Societies (JBDS) for inpatient care. Management of hyperglycaemia and steroid (glucocorticoid) therapy: a guideline from the Joint British Diabetes Societies (JBDS) for inpatient care group. Diabet Med. 2018; 35: 1011‑1017. | Crossref
- Simion C, Campello E, Bensi E, et al. Use of glucocorticoids and risk of venous thromboembolism: a narrative review. Semin Thromb Hemost. 2021; 47: 654‑661. | Crossref
- Elena C, Chiara M, Angelica B, et al. Hyperglycemia and diabetes induced by glucocorticoids in nondiabetic and diabetic patients: revision of literature and personal considerations. Curr Pharm Biotechnol. 2018; 19: 1210‑1220. | Crossref
- Fathallah N, Slim R, Larif S, et al. Drug‑induced hyperglycaemia and diabetes. Drug Saf. 2015; 38: 1153‑1168. | Crossref
- Cui A, Fan H, Zhang Y, et al. Dexamethasone‑induced Krüppel‑like factor 9 expression promotes hepatic gluconeogenesis and hyperglycemia. J Clin Invest. 2019; 129: 2266‑2278. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION