When first impressions lead in a wrong direction: a spectacular presentation of facial erysipelas



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
When first impressions lead in a wrong direction: a spectacular presentation of facial erysipelas
According to the World Health Organization, Streptococcus pyogenes causes around 500 000 deaths per year.1 It is an etiological factor for a range of clinical conditions of different severity, including pharyngitis, scarlet fever, impetigo, erysipelas, cellulitis, type II necrotizing fasciitis, streptococcal toxic shock syndrome, acute rheumatic fever, and poststreptococcal glomerulonephritis.2
Erysipelas is a skin infection involving the dermis layer of the skin, and it can also affect the superficial lymphatic vessels of the skin. In most cases, it is caused by group A streptococci and responds well to antibiotics.3
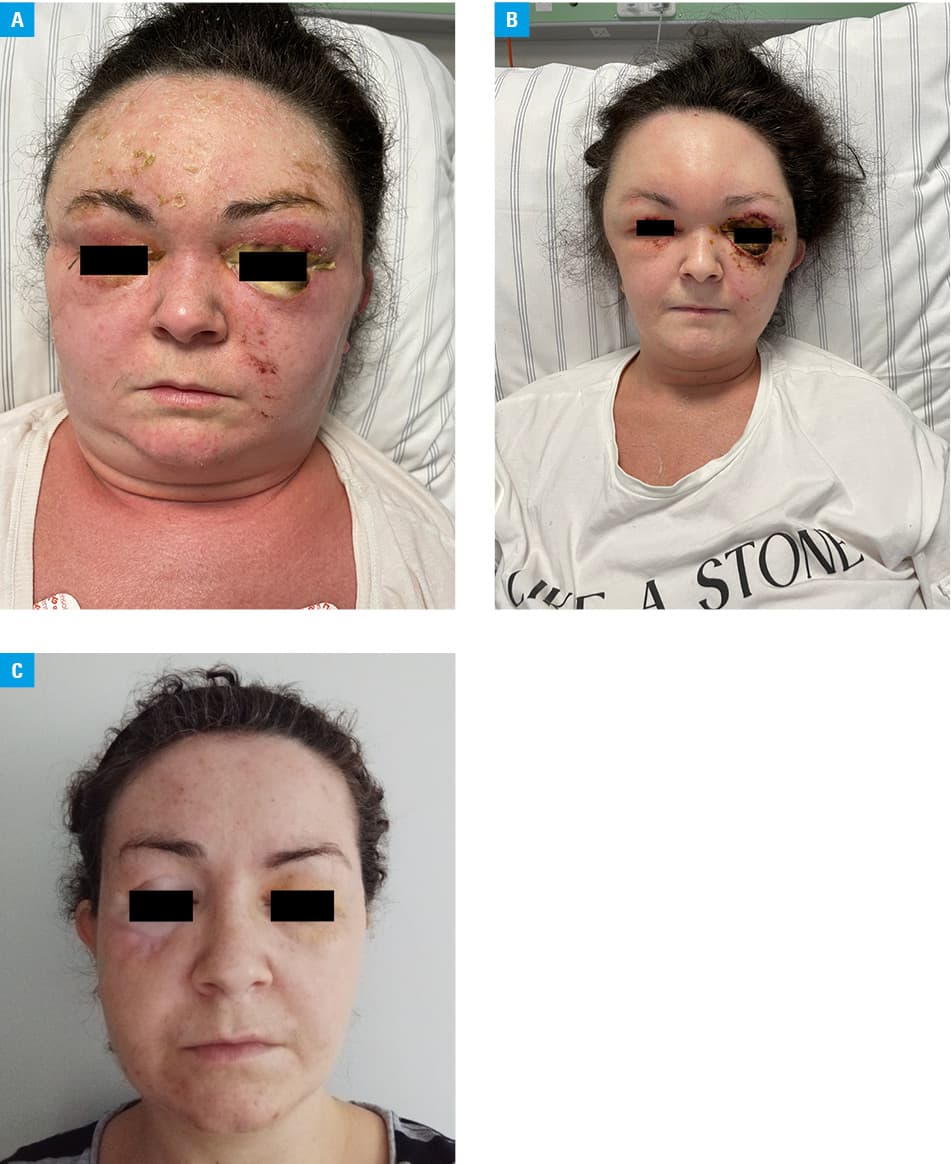
A 35‑year‑old woman was admitted to a department of internal medicine because of massive edema of the face, neck, and subcutaneous tissue of the chest, swollen eyelids, and pink ocular discharge (Figure 1A).
Six days before admission, the patient reported a painful red papule on her forehead, headache, cough, and fever. After 3 days, a general practitioner diagnosed herpes zoster and prescribed acyclovir and naproxen.
On the fifth day from the onset of the symptoms, the patient presented to an ophthalmology emergency department with edema of the upper part of the face, extending to both ears and the alae of the nose, and red, peeling skin. The patient received intravenous dexamethasone and was discharged with a prescription for oral bilastine, fludrocortisone, dexamethasone, and olopatadine eye drops. On the same day, at an emergency department of an internal medicine department of another hospital, she was diagnosed with angioedema with no modification of the treatment.
On day 6 after the onset of the symptoms, the patient was again admitted to a department of internal medicine. Physical examination showed significant swelling of the face, neck, and subcutaneous tissues of the chest, as well as ocular constriction and pink ocular discharge. Additionally, an extensive, fine‑spotted rash was observed over the entire body. Tachycardia was present. The patient was consulted at an ophthalmology emergency department. Ophthalmological examination was not possible due to massive eyelid edema. The eyeballs were not visible on ultrasound.
The patient reported a history of streptococcal and staphylococcal infections with skin lesions on the forehead and lower limbs, roughly a year earlier, and episodes of ankle swelling with blister formation 6 months earlier.
Laboratory tests showed markedly elevated inflammatory markers (C‑reactive protein, 517 mg/l; reference range [RR] <5 mg/l and procalcitonin, 5.2 ng/ml; RR <2 ng/ml), increased activity of liver enzymes (alkaline phosphatase, 156 U/l; RR <35 U/l; aspartate transaminase, 71.5 U/l; RR <35 U/l), and D‑dimer concentration was 3686 ng/ml (RR <500 ng/ml). Blood and conjunctival swab cultures were taken, and the patient was immediately started on intravenous broad‑spectrum antibiotics: ceftriaxone and vancomycin. She was also given subcutaneous low‑molecular‑weight heparin in a prophylactic dose.
Noncontrast computed tomography (CT) of the head demonstrated massive soft‑tissue edema, while high‑resolution (HR) CT of the chest identified small areas of ground‑glass opacity and subpleural edema bilaterally in the neck region. There were no abnormalities on CT angiography of the neck and head and abdominal ultrasound. Echocardiography did not identify any vegetation on the heart valves.
After dermatologic consultation, immediate antibiotic therapy was recommended. Further recommendations included continued treatment of the edema (intravenous dexamethasone and antihistamines), isolating the patient, and awaiting culture results.
The blood cultures returned positive for S. pyogenes, sensitive to penicillin, vancomycin, and linezolid. The conjunctival swab cultures from both eyes were positive for S. pyogenes, sensitive to penicillin, erythromycin, clindamycin, tetracycline, levofloxacin, ofloxacin, and moxifloxacin. The conjunctival swab culture of the right eye was also positive for Staphylococcus epidermidis. Mycological conjunctival swab culture was negative from both eyes.
During treatment, regression of the edema and the appearance of necrotic lesions on the left eyelids were observed (Figure 1B). The antimicrobial treatment was modified: intravenous clindamycin was added, and topical chloramphenicol and ofloxacin eye ointments, as well as moxifloxacin eye drops were introduced. On the third day of hospitalization, mucormycosis was suspected and amphotericin B was initiated. The mycological cultures remained negative, but the prophylactic treatment was continued.
The patient was also consulted at an oxygen hyperbaric unit, but was disqualified due to the lesions observed on HRCT. After follow‑up imaging, the patient was qualified for therapy which continued for 3 months (Figure 1C).
Why was the first diagnosis missed? In the case of herpes zoster, initial skin lesions are red spots and papules, but within 7–10 days, they evolve into blisters which then change to pustules and scabs. In addition, 3–4 days before skin lesions appear, there is usually pain and paresthesia in the affected dermatomes.
Why was the second diagnosis also incorrect? Angioedema is a swelling of the subcutaneous tissue caused by dilation and increased permeability of blood vessels. It develops within minutes to hours, is well demarcated, and asymmetrical. It typically affects eyelids, red lips, genital area, and distal parts of the extremities, as well as the mucous membranes of the upper respiratory and gastrointestinal tracts.
The patient’s spectrum of symptoms, including massive edema and significantly elevated inflammatory markers, strongly suggested an infectious cause of the edema. Positive blood cultures and clinical improvement after antibiotic therapy were decisive for the final diagnosis.
Our medical case shows a spectacular presentation of facial erysipelas. Erysipelas can be severe, but it responds quickly and favorably to antibiotics. This case highlights the relevance of a thorough medical interview and the importance of a diagnostic process based on the entire clinical picture rather than individual symptoms.
- World Health Organization. The current evidence for the burden of group a streptococcal diseases. https://www.who.int/publications/i/item/WHO‑FCH‑CAH‑05.07. February 10, 2025. | Crossref
- Kimberlin DW, Brady MT, Jackson MA. Group A streptococcal infections. Pediatr Rev. 2011; 10: 423‑439. | Crossref
- Kanwal S, Vaitla P. Streptococcus Pogenes. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan. https://www.ncbi.nlm.nih.gov/books/NBK554528/. Accessed February 13, 2025. | Crossref
ARTICLE INFORMATION