A 73‑year‑old woman, diagnosed with seronegative rheumatoid arthritis (RA) and RA‑associated interstitial lung disease, was admitted to the Rheumatology Department of the Lower Silesian Specialist Hospital in September 2022 for routine monitoring of the safety and efficiency of adalimumab therapy.
The patient had been qualified for biological therapy in June 2022 due to persistent moderate disease activity despite treatment with methotrexate and hydroxychloroquine. At the monitoring visit, she reported progressive deterioration of general well‑being and a loss of 10 kg of body weight. On physical examination, pallor, cachexia, tenderness, swelling, and limited range of motion of the knees, as well as pitting edema of the feet were observed.
Laboratory test results showed elevated erythrocyte sedimentation rate (>140 mm/h; reference range [RR] <15 mm/h) and C‑reactive protein level (173 mg/l; RR, 0–6 mg/l), moderate normocytic anemia (hemoglobin, 9.7 g/dl; RR, 10.8–15 g/dl), lymphopenia (white blood cell count, 0.65 × 103/µl; RR, 1.2–3.3 × 103/µl), and increased cancer antigen 125 concentration (64.7 U/ml; RR <35 U/ml). The patient deteriorated over the next days, developing tachyarrhythmia with signs of heart failure. Due to suspicion of pneumonia in the presence of respiratory symptoms, she was empirically started first on amoxicillin with clavulanic acid, to little effect, and next on levofloxacin, with some improvement.
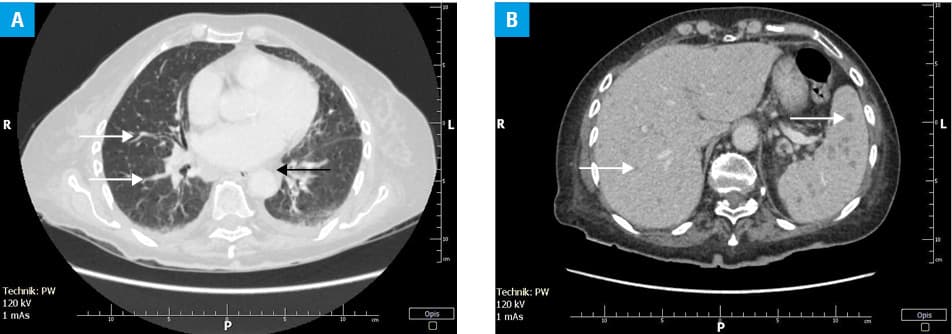
Contrast‑enhanced computed tomography (CT) of the chest (Figure 1A), abdomen (Figure 1B), and pelvis identified mediastinal and abdominal lymphadenopathy, with lung lesions described as lymphangitis carcinomatosa, as well as uncountable lesions of up to 0.6 cm in the liver and spleen. The radiologic diagnosis was metastatic cancer, possibly originating in the lung.
The patient was consulted by a pulmonologist who stated that the clinical and radiologic picture could correspond to an advanced malignant process, possibly originating from the right lung. Due to the patient’s general condition (Eastern Cooperative Oncology Group 3/4), she was disqualified from further invasive procedures, including bronchoscopy. In the opinion of the consulting pulmonologist, even if histopathologic confirmation of the lung cancer diagnosis were possible to obtain, the patient would be disqualified from oncologic treatment. Symptomatic treatment under the care of a home hospice was recommended.
An alternative diagnosis, reactivation of latent tuberculosis (TB) in the course of anti‑tumor necrosis factor α therapy, was considered. The QuantiFERON‑TB Gold Plus test (QIAGEN, Venlo, Netherlands) result was positive (in contrast to the negative result obtained prior to the biological treatment). However, quick blood and urine polymerase chain reaction (PCR) tests for Mycobacterium tuberculosis (the patient did not cough up sputum which could be collected for examination) were negative. A literature search performed in order to establish whether TB could mimic lung carcinoma on CT showed that few such cases had indeed been reported.
In the light of the positive QuantiFERON‑TB Gold Plus test result and temporal correlation of sudden health deterioration with introduction of adalimumab, despite the lack of definitive microbiological confirmation, the patient was discharged from the hospital with a tentative diagnosis of mycobacteriosis, to be differentiated from metastatic malignant process based on response to treatment with antimycobacterial therapy consisting of pyrazinamide, isoniazid, rifampicin, and levofloxacin. Early follow‑up at a pulmonology clinic was recommended.
At 1‑year follow‑up at a rheumatology clinic, the patient was well recovered. Follow‑up CT showed regression of lymphadenopathy and disseminated pulmonary, hepatic, and splenic lesions. Her RA was satisfactorily managed with low‑dose prednisone and 10 mg of leflunomide daily. Other than a spectacular response to antimycobacterial drugs, the diagnosis of mycobacteriosis was never definitively confirmed.
Systemic mycobacteriosis and metastatic lung cancer may be undistinguishable based on clinical course or imaging results. Symptoms, such as hemoptysis, weight loss, or fever, are nonspecific and may occur in both diseases. Older age is a risk factor for both mycobacteriosis and cancer. The 2 diseases may coexist, or one can precede the other, and both can have extrapulmonary involvement.1
Mycobacterioses pose a diagnostic challenge also in low‑incidence countries, despite access to advanced imaging modalities. No imaging modality, including positron emission tomography / CT, is capable of confidently differentiating between miliary TB and metastatic lung cancer, as lesions in both diseases present with increase in fluorodeoxyglucose uptake, and frequently coexistent lymphadenopathy.2 Other than lung cancer, mycobacterioses may be difficult to distinguish from sarcoidosis, lymphoproliferative disorders, and fungal infections, such as actinomycosis or mucormycosis, or nocardiosis.3,4
In clinical practice, the diagnostic process for lung cancer should include chest CT, transbronchial or CT‑guided biopsy, and histopathology.4 However, due to high mortality in untreated patients with disseminated mycobacterioses, in the presence of multiple lung lesions, it is no less important to exclude systemic mycobacterial infection than to exclude metastatic cancer, especially as the former is a curable disease. TB diagnostic workup includes sputum examination, autofluorescence bronchoscopy, culture, and a PCR test. Interferon-γ release assays detect sensitization to Mycobacterium spp. and cannot differentiate between active and latent infections.
Finally, mycobacterioses and lung cancer may coexist. Patients diagnosed with TB that are at a high risk of lung cancer according to the American Association of Thoracic Surgery, that is patients of 55 years and older, with a smoking history of 30 pack‑years or more, should be assessed with chest CT for underlying malignancy prior to anti‑TB treatment, even in the presence of a microbiologic confirmation of TB.
Opportunistic mycobacterial infections will be an ever‑increasing problem due to a rise in the number of patients on chronic immunosuppressive therapies. In a nationwide Japanese study, out of 7755 RA patients on adalimumab treatment, 22 TB cases were identified, all symptomatic and mostly (77%) with extrapulmonary involvement. Risk factors for TB determined by a multivariate analysis were age over 65 years, past or current renal dysfunction, RA activity, and diabetes mellitus, in descending order.5
Mycobacterioses are great mimickers and can present both clinically and radiologically similar to metastatic cancer. Microbiology is useful for mycobacterial infection diagnosis, although negative results do not exclude mycobacteriosis. Lung biopsy is the gold diagnostic standard for lung cancer, although it may not always be available. Taking a pause to consider a probability of mycobacteriosis, curable yet fatal if left untreated, in the clinical context, is crucial in the evaluation of disseminated lung lesions in immunocompromised patients.
- Romaszko‑Wojtowicz A, Malinowska E, Doboszyńska A. Unmasking Pott disease: a diagnostic challenge mimicking metastatic lung cancer ‑ a case report. Am J Case Rep. 2024; 25: e943578. | Crossref
- Zheng Z, Pan Y, Guo F, et al. Multimodality FDG PET/CT appearance of pulmonary tuberculoma mimicking lung cancer and pathologic correlation in a tuberculosis‑endemic country. South Med J. 2011; 104: 440‑445. | Crossref
- Madhusudhan KS, Gamanagatti S, Seith A, Hari S. Pulmonary infections mimicking cancer: report of four cases. Singapore Med J. 2007; 48: e327‑e331. | Crossref
- Cardinale L, Nika L, Teti M, et al. Pulmonary tuberculosis in diagnostic imaging: the great mime [in Italian]. Recenti Prog Med. 2018; 109: 220‑225.
- Watanabe A, Matsumoto T, Igari H, et al. Risk of developing active tuberculosis in rheumatoid arthritis patients on adalimumab in Japan. Int J Tuberc Lung Dis. 2016; 20: 101‑108. | Crossref
ARTICLE INFORMATION