Epidemiology of venous thromboembolism: implications for clinical practice
Key words: epidemiology, incidence, mortality, pulmonary embolism, venous thromboembolism

 CC BY 4.0
CC BY 4.0
Epidemiology of venous thromboembolism: implications for clinical practice
Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common disorder with annual incidence rates of 150 (95% CI, 131–169), 90 (95% CI, 72–109) and 67 (95% CI, 54–80) per 100 000 population for VTE, DVT, and PE, respectively in Western countries. Of note, reported VTE incidences are considerably lower in East Asia. VTE incidence increases with age and is comparable between sexes, although men exhibit a higher risk of recurrence. Incidence rates of PE, but not of DVT, have been increasing in the last decades, reflecting changes in diagnostic workup and risk factors. VTE has a significant impact on mortality, and it is estimated that death from PE, which includes sudden death from undiagnosed, untreated PE, may be responsible for approximately 3% of all deaths. Nevertheless, diagnosed and treated VTE still carries a substantial risk with case fatality rates up to 10% in contemporary cohorts. Even when conservative calculations are applied, VTE death rate is approximately 26 (95% CI, 19–32) per 100 000, which makes it—at least in Europe and North America—the third most common reason of death from cardiovascular diseases and fifth from all causes. In this article, we summarize the current state of knowledge and recent data on the epidemiology of VTE with a particular focus on mortality from PE and its clinical implications.
Introduction
Venous thromboembolism (VTE) is a common and potentially preventable and treatable condition that includes deep vein thrombosis (DVT) and pulmonary embolism (PE). It is the third most common cardiovascular disease after myocardial infarction (MI) and ischemic stroke (IS), with an estimated annual incidence of approximately 150 per 100 000 individuals in the general population.1 VTE covers a wide range of severity, from isolated distal DVT, which is usually treated for several weeks only, to iliofemoral thrombosis and high‑risk PE that may require invasive treatment approaches.2,3 The burden of VTE is particularly significant because of its recurrent nature, potential for sudden death, and long‑term complications, such as post‑thrombotic syndrome (PTS) and chronic thromboembolic pulmonary hypertension (CTEPH).4 Despite these clear epidemiological data, the impact of VTE on cardiovascular and total mortality is often greatly underestimated. For example, the Global Burden of Disease Study does not list VTE or PE as a cause of death.5 Likewise, public awareness regarding the potential danger of VTE is considerably lower than that of MI or IS.6 In this article, we summarize the current state of knowledge and recent data on the epidemiology of VTE, including age- and sex‑specific differences, with a particular focus on mortality. We also discuss the clinical consequences and implications of these epidemiological data.
Incidence rates including age- and sex‑related aspects
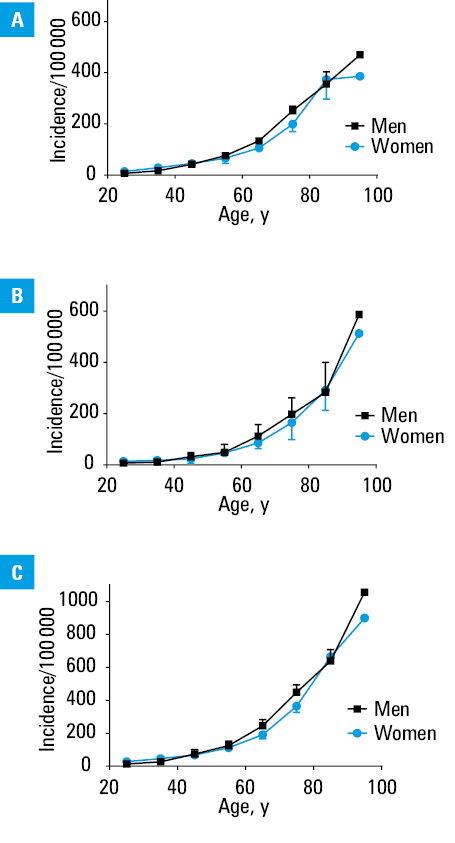
VTE can manifest as isolated DVT, DVT with concomitant PE, or PE without diagnosed DVT. Table 1 lists the incidence for DVT, PE, and VTE in studies almost exclusively from high‑income countries, spanning from 1980 until 2025.7-47 In Europe and North America, VTE is a common disease with annual incidence rates of 150 (95% CI, 131–169), 90 (95% CI, 72–109), and 67 (95% CI, 54–80) per 100 000 population for VTE, DVT, and PE, respectively. It is well known that the incidence of VTE increases with age, with rates starting from less than 5 per 100 000 in children, and reaching over 500 per 100 000 in individuals aged 80 years and older (Figure 1).11,18,36 It has been reported that VTE may be more frequent in women, probably due to the effects of estrogens on the coagulation cascade.17,41 However, this was not consistently found in all studies (Table 1).22 When the incidence rates are standardized for age, no clear difference between men and women can be found (Figure 1).33 Importantly, the risk of recurrent VTE after the first episode of VTE without an identified major trigger is more than 3 times higher in men than in women.48
Country | DVT | PE | VTE | Reference |
Data are presented as number of cases per 100 000/year.
a East Asian countries are listed separately due to comparably low incidence.
b France, Germany, Italy, Spain, Sweden, and United Kingdom
c Means and 95% CIs were calculated without East Asian countries and territories.
Abbreviations: DVT, deep vein thrombosis; M, men; NR, not reported; PE, pulmonary embolism; VTE, venous thromboembolism; W, women | ||||
Sweden | 85 M; 68 W | NR | NR | Kierkegaard et al7 |
United States | 48 | 23 | 107 | Anderson et al9 |
Sweden | 155 M; 162 W | NR | NR | Nordstrom et al10 |
United States | 48 | 69 | 117 | Silverstein et al11 |
France | 124 | 60 | 183 | Oger et al12 |
United States | 117 | 45 | 161 | Cushman et al13 |
United States | 104 | 36 | 130 | Stein et al14 |
Europeb | 148 | 95 | NR | Cohen et al16 |
United Kingdom | 40 | 34 | 75 | Huerta et al17 |
Norway | 93 | 50 | 143 | Naess et al18 |
Australia | 52 | 31 | 83 | Ho et al19 |
Denmark | NR | NR | 269 | Holst et al20 |
Italy | NR | 19 | NR | Moretti et al21 |
Denmark | 65 | 51 | 115 | Severinsen et al22 |
United States | NR | 112 | NR | Wiener et al25 |
United States | 152 | 121 | 239 | Yusuf et al26 |
Canada | 78 | 45 | 122 | Tagalakis et al27 |
Australia | NR | 53 | NR | Shiraev et al28 |
Argentina | 130 | 64 | 165 | Vazquez et al29 |
Norway | NR | NR | 148 | Hald et al30 |
Spain | – | 33 | – | De Miguel‑Diez et al31 |
United States | 68 | 65 | 133 | Huang et al32 |
Italy | NR | 40 M; 56 W | NR | Dentali et al33 |
France | NR | 110 | 157 | Delluc et al34 |
Canada | 100 | 38 | 138 | Alotaibi et al35 |
United States | 47 | 62 | 123 | Heit et al36 |
Norway | 88 | 113 | 201 | Arshad et al37 |
Sweden | NR | 76 | 193 | Wändell et al38 |
Denmark | 70 | 81 | 151 | Münster et al39 |
Canada | NR | NR | 129 | Payne et al40 |
Denmark | NR | NR | 117 M; 128 W | Arnesen et al41 |
United Kingdom | NR | NR | 183 | Conrad et al42 |
France | 25 | 91 | 116 | Gabet et al44 |
Switzerland | NR | 119 | NR | Wolf et al45 |
Austria | NR | 73 | NR | Leinweber et al47 |
Mean (95% CI)c | 90 (72–109) | 67 (54–80) | 150 (131–169) | |
East Asian countries and territories | ||||
Hongkong | NR | NR | 8 | Woo et al8 |
Taiwan | NR | NR | 16 | Lee et al23 |
Korea | 5 | 7 | 14 | Jang et al24 |
China | NR | NR | 48 | Hu et al43 |
China | NR | 14 | NR | Zhen et al46 |
Global burden
Most of the data on the incidence of VTE come from high‑income countries, and the burden in low- and middle‑income countries is likely underreported due to limited diagnostic capabilities. Notably, considerably lower incidence rates of VTE have consistently been reported from East Asia in comparison with the European and North American countries (Table 1).
Recently, however, incidence rates appear to increase also in Asia.43 In large studies from the United States, the incidence of VTE was higher in African Americans than white people, and the lowest in individuals of Asian or Pacific Islander descent.14,49,50
Risk factors for venous thromboembolism
The occurrence of VTE is influenced by a variety of risk factors, both acquired and inherited. The acquired risk factors include surgery, trauma, cancer, hospitalization, immobilization, pregnancy, and the use of hormonal therapy. Inherited traits of thrombophilia, such as factor V Leiden or the G20210A prothrombin gene mutation, also contribute to the frequency of VTE (Table 2).51 The risk factors for VTE can be classified according to their duration into permanent and temporary, and according to their mode of action into provoking and not provoking.52 In practical terms, their predictive value for VTE is of interest. Table 2 lists common risk factors according to their odds ratio.4,53 Recently, is has been acknowledged that the risk factors for VTE may partly overlap with risk factors for arterial thrombosis.54 A considerable number of cases are observed during or shortly after hospitalization, making VTE a partially preventable disorder.
Strong risk factors (OR >10) | Moderate risk factors (OR, 2–9) | Weak risk factors (OR <2) |
Abbreviations: OR, odds ratio | ||
Fracture of lower limb | Arthroscopic knee surgery | Arterial hypertension |
Hospitalization for heart failure | Autoimmune disease | Bed rest >3 days |
Hip or knee replacement | Blood transfusion | Diabetes |
Major surgery | Indwelling venous catheters and leads | Immobility due to sitting (eg, prolonged car or air travel) |
Major trauma | Chemotherapy | Laparoscopic surgery |
Myocardial infarction | Erythropoiesis‑stimulating agents | Obesity |
Previous venous thromboembolism | Hormone replacement therapy | Strenuous exercise |
Spinal cord injury | Infection | Varicose veins |
– | Inflammatory bowel disease | – |
– | In vitro fertilization | – |
– | Malignancy | – |
– | Oral contraceptive use | – |
– | Stroke with paralysis | – |
– | Pregnancy | – |
– | Puerperium | – |
– | Superficial vein thrombosis | – |
– | Thrombophilia | – |
Temporal trends and emerging risk factors for venous thromboembolism
While the incidence of DVT has remained relatively stable over the past 2 decades, the incidence of PE has increased. This trend is largely attributed to the broader availability and use of computed tomography pulmonary angiography, enabling the detection of subsegmental PE, which often has unclear clinical significance (Table 1).32,55 This phenomenon may also be linked to suboptimal adherence to evidence‑based diagnostic pathways outlined in current guidelines.56,57
Reproductive and hormonal risk factors
The use of estrogen‑containing oral contraceptives, particularly third‑generation formulations, is an important risk factor for VTE in young women. These agents are widely used in developed countries, and their association with elevated thrombotic risk, especially in those with inherited thrombophilia, continues to be clinically relevant. A German hospital‑based study58 carried out between 2005 and 2014 demonstrated a disproportionate rise in PE incidence among young women, which has been attributed to the use of oral contraceptives. Pregnancy continues to be a well‑established risk factor for VTE. Of note, the increasing maternal age, especially in Europe, has introduced new challenges. Older pregnant women, often receiving thromboprophylaxis, still show an elevated VTE risk.59 A Swedish registry study covering the years from 1987 to 2019 revealed an upward trend in pregnancy‑associated PE, further underscoring the need for targeted risk assessment and prevention.60
Surgery-, trauma-, and hospitalization‑associated venous thromboembolism
Major orthopedic procedures, such as total hip or knee arthroplasty and hip fracture repair, carry a high thrombotic risk, and routine prophylaxis has demonstrated efficacy in reducing VTE‑related events.61 This is also true for a large proportion of nonorthopedic surgical interventions, where the risk of thromboembolism should be evaluated on an individual basis using validated risk scores.62 Trauma patients, especially those with pelvic fractures, spinal cord injuries, or prolonged immobilization, also benefit significantly from early pharmacological and mechanical prophylaxis.63 Despite advancements in high‑resource settings, especially low- and middle‑income countries continue to experience inconsistent implementation of VTE prophylaxis guidelines. A multinational study by Cohen et al64 found that only 58% of surgical and 40% of medical patients at risk received appropriate prophylaxis according to evidence‑based guidelines.
Cancer‑associated thrombosis
VTE in cancer patients, also known as cancer‑associated thrombosis (CAT), shows rising numbers and affects up to 20% of all cancer patients. This is particularly concerning, since CAT confers a worse prognosis and is the second most frequent cause of death in these patients after cancer itself. The increase in CAT is primarily due to an increase in PE, which may be partly due to an aging patient population and new targeted therapies with an increased risk for VTE.65 As in other clinical scenarios, the adequate use of primary prevention is crucial to reduce the risk of VTE in this particularly vulnerable patient group.66 The increasing use of indwelling venous catheters, including central venous ports for chemotherapy and long‑term antibiotics, is a growing contributor to DVT. It is estimated that such devices are responsible for up to 10% of DVT cases. Vigilant monitoring and catheter care protocols are essential to mitigate this risk.67
Obesity and the impact of the obesity pandemic
The global obesity epidemic plays a significant role in the rising VTE burden. Obesity has been identified as an established independent risk factor for both DVT and PE.68,69 Large‑scale epidemiological data demonstrate a dose‑dependent association between body mass index and VTE risk, with obese individuals exhibiting a 2.5‑fold higher risk than those with normal weight, particularly in younger patients and women using estrogen‑containing contraceptives.69 Antiobesity interventions—including structured lifestyle modification and bariatric surgery—have been associated with reductions in VTE risk. While bariatric surgery transiently increases thrombotic risk, long‑term follow‑up studies consistently show significant reductions in VTE incidence and cardiovascular morbidity.70 Likewise, the available short‑time data on pharmacological therapies inducing sustained weight loss, such as glucagon‑like peptide‑1 receptor agonists, have demonstrated an increased risk for VTE.71 It remains to be clarified whether long‑term treatment with these agents may contribute to VTE risk mitigation.
Pulmonary embolism as an important cause of death
Severe PE can lead to right heart failure due to acute pressure overload, and is a leading cause of death.4 However, since approximately 90% of fatal PE cases appear to be sudden deaths or follow undiagnosed and untreated PE, the exact number of PE‑related fatalities is difficult to determine.16,72 Valuable data come from post mortem studies, especially in countries with high autopsy rates.73-77 Additional evidence is available from cohort studies, national databases, and estimates from population‑based studies.6,16,18,21,25,27,28,31,33,35,43-47,78-82 Based on the numbers shown in Table 3, the mean annual number of deaths from VTE per 100 000 equals 26 (95% CI, 19–32), and the mean percentage of PE deaths per all deaths is about 3.1% (95% CI, 1.2%–5.1%).
Data | VTE deaths / 100 000 | % of all deaths | PE case fatality rate (30 d), % | Reference |
a In‑hospital mortality
b Mortality after introduction of computed tomography pulmonary angiography
Abbreviations: see Table 1 | ||||
Post mortem studies | ||||
United Kingdom | 37 | 10 | NR | Sandler et al73 |
Sweden | 77 | 7.5 | NR | Nordström et al74 |
United States | 9.4 | 1.3 | NR | Horlander et al75 |
Brazil | NR | 2.5 | NR | Carvalho Bricola et al76 |
Austria | NR | 6.5 | NR | Konschake et al77 |
Data from cohort studies and national databases | ||||
Norway | NR | NR | 9.7 | Naess et al18 |
Austria | 12.8 | 1.3 | NR | Hoffmann et al78 |
NR | NR | 4.2 | Leinweber et al47 | |
Netherlands | 2.5 | 0.3 | NR | Hoffmann et al78 |
Italy | NR | NR | 10.9a | Moretti et al21 |
United States | 11.9b | 1.5 | 7.8 | Wiener et al25 |
Canada | NR | NR | 10.6 | Tagalakis et al27 |
NR | NR | 3.9 | Alotaibi et al35 | |
Spain | NR | NR | 8.3 | De Miguel‑Diez et al31 |
5.1 M; 4.4 W | 0.6 | NR | Cayuela et al79 | |
Italy | NR | NR | 10.1 | Dentali et al33 |
China | NR | NR | 2.1a | Hu et al43 |
France | 6 | 0.7 | 7.5 | Gabet et al44 |
Switzerland | 13 | 2.3 | 7.9 | Wolf et al45 |
Estimates from population‑based studies | ||||
Europe | 119 | 10 | NR | Cohen et al16 |
United States | 33 | 4 | NR | Galson et al80 |
100 | 12 | NR | Raskob et al81 | |
19–32 | 2.2–3.6 | NR | Wendelboe et al6 | |
17–29 | 2.2–3.6 | NR | Glazier et al82 | |
Even the calculated mean case fatality rate is relatively high (8.2%; 95% CI, 6.6%–9.8%), and in the range of other major cardiovascular diseases, such as MI (8.9%) and IS (8.7%).67,83 The seeming decrease in mortality from PE over time may be due to the decreasing autopsy rate in most countries.84 Interestingly, an autopsy study carried out in 1987 in Sweden with an autopsy rate of 79%74 and an analysis of death certificates of body donors in an Austrian anatomical department from 201477 yielded similar results, arguing against a decreasing trend in mortality from PE (Table 3). However, as can be seen in Table 3, the case fatality rate of diagnosed and treated VTE appears to decrease over time, reflecting advances in the management of the disease, such as improved diagnostic workup and advanced therapies, including catheter‑directed thrombolysis and catheter‑based mechanical thrombus removal.3 As an additional factor for these epidemiologic changes, overdiagnosis of PE (segmental and subsegmental occlusion) by improved imaging technologies has been discussed.25 The wide variation in mortality numbers may be partly explained by inaccuracies in assigning the underlying cause of death and / or erroneous coding of the hospital records.78 Moreover, due to current low autopsy rates in nearly every country, there is a tendency to considerably underdiagnose PE as a cause of death.72 Of note, cancer patients have a particularly high risk of dying from PE.85 In the early phase of the COVID‑19 pandemic, a high number of fatal PE cases was described in autopsy studies.86 The 30‑day mortality for PE can be estimated by combining clinical, imaging, and laboratory parameters, and it ranges from low‑risk (30‑day mortality <1%) to high‑risk PE (30‑day mortality >15%; Table 4).4 Even after the acute phase, long‑term mortality remains elevated, particularly in patients with CAT and recurrent events. Importantly, VTE recurrence itself contributes to the morbidity and mortality burden, with recurrence rates approaching 30% at 10 years without extended anticoagulation.87
30‑day mortality risk | Hemodynamic instability | PESI class III–V or sPESI ≥1 | RV dysfunction (TTE, CTPA) | Elevated cardiac troponin | Percentage |
Patients with signs of RV dysfunction on TTE (or CTPA) or with elevated cardiac troponin and a calculated PESI class I or II or a sPESI of 0 should be classified as intermediate risk.
Abbreviations: CTPA, computed tomography pulmonary angiography; PESI, pulmonary embolism severity index; RV, right ventricle; sPESI, simplified pulmonary embolism severity index; TTE, transthoracic echocardiography | |||||
High (>15%) | + | + | + | + | <5 |
Intermediate (3%–15%) | 60 | ||||
Intermediate‑high | – | + | + | + | |
Intermediate‑low | – | + | 1 (or none) positive | ||
Low (<1%) | – | – | – | – | 35 |
Clinical implications
To reduce the burden and especially the mortality from VTE, adequate diagnosis and early initiation of anticoagulant treatment are crucial. However, in many countries, the diagnosis of acute PE remains suboptimal due to restricted availability of continuous imaging services, insufficient access to multidisciplinary consultations, inadequate protocols for transferring patients to higher‑tier referral centers, and limited physician awareness of established risk stratification principles. These deficiencies may compromise the comprehensiveness of diagnostic evaluation, thereby contributing to both under- and overdiagnosis. Improving access to diagnostic tools, standardizing referral pathways (eg, via PE response teams), and strengthening medical education are necessary steps to address these deficiencies.88 Effective risk stratification tools, such as the Pulmonary Embolism Severity Index, help clinicians in identifying patients at a higher risk of mortality and complications.4,89 Appropriate anticoagulant therapy is the cornerstone of VTE treatment, and has significantly improved survival. However, the risk of bleeding remains an important limitation, particularly in elderly patients and in the presence of comorbidities.
Given its preventable nature, hospital‑associated VTE is a major target for health interventions. Thromboprophylaxis in high‑risk patients—including those undergoing surgery or experiencing prolonged immobilization—has been shown to significantly reduce VTE incidence. Despite guidelines, implementation remains inconsistent, and there is an urgent need for improved adherence and constant re‑evaluation of prophylactic strategies.90
Survivors of VTE events often face substantial morbidity. PTS occurs in up to 50% of patients with proximal DVT, leading to chronic leg pain, swelling, and ulceration.91 CTEPH, a rare but severe complication, is expected to develop in approximately 2.4% of patients with acute PE, and it contributes to long‑term functional decline and increased mortality.92 Both PTS and CETPH have distinct risk factors in patients with VTE that are summarized in Table 5.92-94 A recent meta‑analysis reported similar rates of PTS across different anticoagulation regimens (vitamin K antagonists [VKAs], direct oral anticoagulants [DOACs], low‑molecular‑weight heparin) with a possible lower rate of severe PTS in patients treated with a DOAC than a VKA.95
Post‑thrombotic syndrome | Chronic thromboembolic pulmonary hypertension |
Abbreviations: INR, international normalized ratio; others, see Table 1 | |
Proximal DVT | (Sub-)massive PE |
Age | Recurrent PE |
Obesity | Unprovoked PE |
Previous ipsilateral DVT | Splenectomy |
Pre‑existing primary venous insufficiency | Ventriculoatrial shunt |
Inadequate INR control during the first 3 months | Chronic inflammatory diseases |
Persistent symptoms after 1 month | Malignancy |
– | Antiphospholipid syndrome |
– | Hypothyroidism |
The epidemiological data summarized in this article have direct clinical implications. Important risk factors, such as the age of an individual patient should be integrated in the diagnostic workup. The higher risk for recurrent VTE in men has profoundly influenced clinical prediction scores for discontinuing anticoagulation.96,97
Conclusions
VTE is a leading cause of cardiovascular mortality, ranking—at least in Europe and North America—at the third place for cardiovascular diseases and at the fifth place for death from all causes (Figure 2). Greater emphasis on risk assessment, adherence to prophylaxis guidelines, early diagnosis, and effective long‑term management are essential to reduce the burden of the disease. Improved surveillance and public health initiatives, such as the World Thrombosis Day, which has been organized every year since 2014, are needed to address these issues and to improve awareness of VTE.81,98 Nevertheless, mortality from PE is greatly underestimated, and has not been included in the Global Burden of Disease Study.5 VTE should urgently be recognized as a distinct entity, similarly to other main vascular diseases, and not summarized under “other cardiovascular diseases”, since risk factors and treatment modalities differ significantly from those applying to arterial diseases.
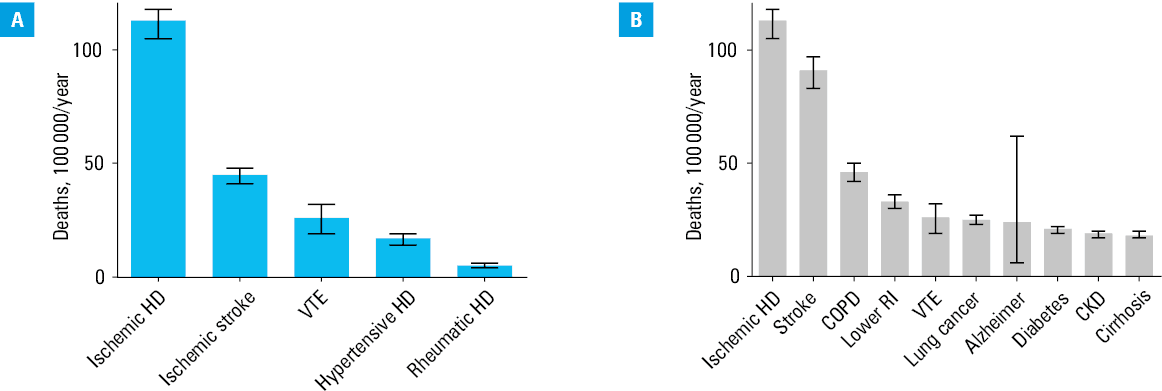
Abbreviations: CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; HD, heart disease; RI, respiratory infection; others, see Table 1
- Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol. 2015; 12: 464‑474. | Crossref
- Potere N, Ageno W. How to treat isolated distal deep vein thrombosis. Pol Arch Intern Med. 2023; 133: 16543. | Crossref
- Schlager O, Campello E, Madaric J, et al. 2025 ESVM Guidelines on interventional treatment of venous thromboembolism. Vasa. 2025 Jun 30. [Epub ahead of print]. | Crossref
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020; 41: 543‑603. | Crossref
- Mensah GA, Fuster V, Murray CJL, et al. Global Burden of Cardiovascular Diseases and Risks, 1990‑2022. J Am Coll Cardiol. 2023; 82: 2350‑2473. | Crossref
ARTICLE INFORMATION