How to effectively treat arterial hypertension in elderly individuals?
Key words: antihypertensive therapy, clinical trials, elderly, frailty, hypertension

 CC BY 4.0
CC BY 4.0
How to effectively treat arterial hypertension in elderly individuals?
Hypertension is the most common cardiovascular risk factor in older adults, significantly contributing to morbidity and mortality. Its prevalence rises with age and is strongly associated with vascular aging, isolated systolic hypertension, and comorbidities, such as cognitive impairment and chronic kidney disease. However, treatment in older adults—especially those with frailty—requires a careful balance between benefit and potential harm. This review aimed to provide an updated synthesis of pathophysiological mechanisms, epidemiological trends, diagnostic considerations, and evidence‑based therapeutic approaches to arterial hypertension in older adults. Emphasis was placed on tailoring treatment strategies according to frailty and functional status. We conducted a narrative review of major international guidelines (European Society of Cardiology, European Society of Hypertension), clinical trials, and real‑world studies addressing hypertension in aging populations. Special focus was given to randomized controlled trials and observational studies stratified by frailty. Evidence supports blood pressure lowering in fit older adults, as demonstrated in trials such as HYVET, SPRINT‑SENIOR, and STEP, which showed significant reductions in cardiovascular events and mortality. Conversely, some studies (eg, PARTAGE, OPTiMiSE, and DANTE) highlighted the risks of overtreatment in frail or institutionalized patients, including hypotension, falls, and increased mortality. The presence of orthostatic hypotension, impaired renal function, and polypharmacy further complicates management. In conclusion, hypertension management in the elderly should follow a personalized approach based on a comprehensive geriatric assessment and frailty evaluation; patient‑centered goals are essential to guide treatment intensity, aiming to protect cardiovascular health without compromising safety, cognition, or functional independence. Future studies must include frailer populations to better inform clinical decisions.
Introduction
Hypertension is the leading modifiable cardiovascular risk factor in individuals aged 65 years and older. Its prevalence progressively increases with age, and it is often associated with several comorbid conditions, such as diabetes, chronic kidney disease (CKD), and cognitive decline.1,2 As populations age, the global burden of hypertension‑related complications—stroke, heart failure (HF), and ischemic heart disease—is consequently expected to grow. In the elderly, isolated systolic hypertension (ISH) becomes the dominant subtype due to vascular stiffening.3
Although blood pressure (BP) lowering has proven benefits in older populations, there is growing recognition that a “one‑size‑fits‑all” approach may not be appropriate. Frailty, polypharmacy, cognitive status, and life expectancy must be considered when determining treatment thresholds and targets.4-8 This review aims to synthesize current knowledge on the pathophysiology, diagnosis, and treatment of hypertension in the elderly, with emphasis on individualized care.
Epidemiology
The prevalence of hypertension significantly increases with age.9,10 According to the Noncommunicable Disease Risk Factor Collaboration, more than 70% of adults over 70 years of age have hypertension,4 and even higher rates (up to 80%) are reported in individuals living with frailty.11
These findings are in line with trends observed in the Polish population,10,12 where among older individuals, hypertension affects more women than men (prevalence of 82.5% and 78.3%, respectively).
Data from the NHANES III study (The Third National Health and Nutrition Examination Survey) confirmed that ISH was the most common subtype among untreated hypertensives aged 60 years and older, particularly affecting postmenopausal women.8,13
While awareness and treatment of hypertension have improved over the past decades, control rates remain suboptimal in elderly populations, and less than 50% of patients achieve optimal control.12 Several factors contribute to this, including resistant hypertension, therapeutic inertia, adverse drug reactions, and decreased adherence due to cognitive or functional impairments.14 Moreover, the presence of white‑coat and masked hypertension further complicates diagnosis and management in this population.15
Pathophysiology
Aging affects both the heart and the arterial system. One of the most significant age‑related cardiovascular changes is the increase in systolic BP (SBP), primarily due to structural and functional alterations of the arterial wall.16,17 The main pathophysiological mechanisms leading to hypertension in older adults are presented in Figure 1.
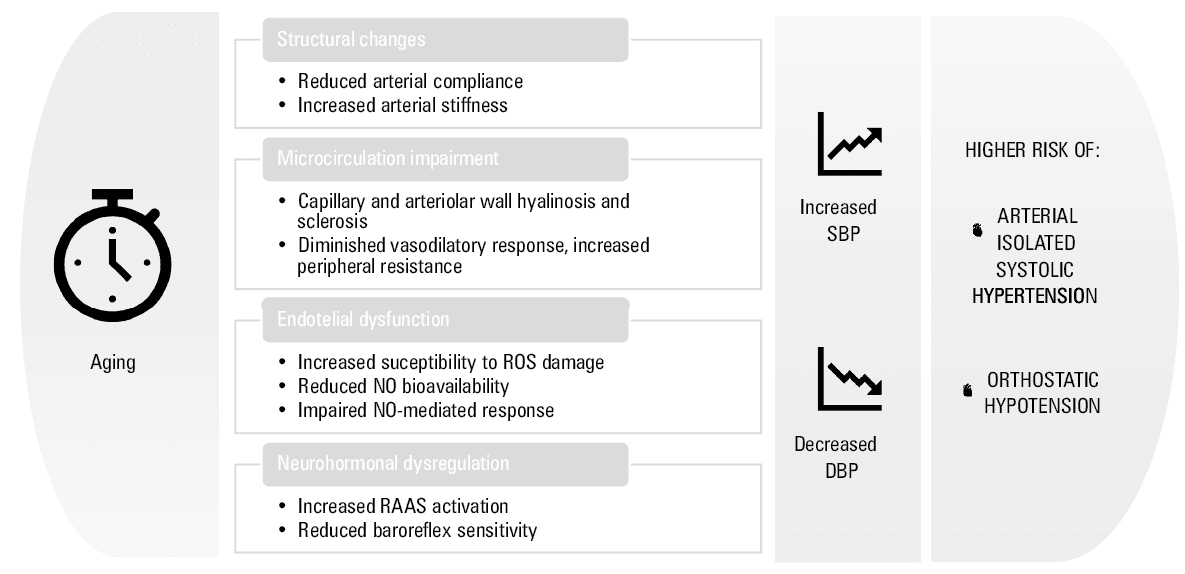
Abbreviations: DBP, diastolic blood pressure; NO, nitric oxide; RAAS, renin‑angiotensin‑aldosterone system; SBP, systolic blood pressure
Arterial compliance and structural changes
Arterial compliance—the ability of arteries to expand and contract in response to pressure changes—declines with age.18 This decline results from alterations in the balance of elastin and collagen within the arterial wall. For instance, the aorta contains approximately 70% elastic fibers and 30% collagen fibers. With age, fragmentation and calcification of elastin, accumulation of collagen, and increased intimal thickness occur, even in individuals without significant atherosclerosis.
These structural changes impair the ability of arteries to buffer pressure waves, leading to increased arterial stiffness and higher pulse wave velocity.19 The reflected pressure wave, which normally augments diastolic pressure and coronary perfusion, returns earlier in the cardiac cycle due to increased stiffness. This premature return elevates systolic pressure and left ventricular afterload while reducing diastolic pressure and coronary flow.
Microcirculation and endothelial dysfunction
Aging also affects the microcirculation, with hyalinosis and sclerosis leading to a reduction in capillary and arteriole diameter. This results in a diminished vasodilatory response, contributing to increased peripheral resistance.
Endothelial dysfunction is another critical component of vascular aging. Endothelial cells exhibit reduced replicative capacity and impaired response to injury. Reactive oxygen species contribute to cellular aging by damaging DNA (especially telomeric DNA), inhibiting telomerase, and inducing mitochondrial dysfunction. Senescent endothelial cells express proinflammatory and prothrombotic markers, such as interleukin 1α, intercellular adhesion molecule 1, and plasminogen activator inhibitor 1. Additionally, nitric oxide (NO) bioavailability declines due to reduced endothelial NO synthase activity and increased NO degradation by superoxide anions.20-23
Flow‑mediated dilation, an indicator of endothelium‑dependent vasodilation, is reduced in the elderly,24 reflecting impaired NO‑mediated responses. Furthermore, endothelial response to prostacyclin (PGI2)-induced vasodilation is also diminished due to decreased NO synthesis.
Neurohormonal activation
Aging is associated with increased sympathetic nervous system activity and activation of the renin‑angiotensin‑aldosterone system (RAAS), further exacerbating vasoconstriction and sodium retention. This neurohormonal dysregulation contributes to BP elevation and reduces baroreflex sensitivity, limiting the ability to buffer BP fluctuations.25
These anatomical and functional alterations in the cardiovascular system contribute to the pathogenesis of hypertension in the elderly. Over time, adaptive mechanisms are exhausted, leading to the development of clinical hypertension, especially ISH.
Clinical trial evidence: fit vs frail older adults
Evidence in fit older adults
The HYVET trial (Hypertension in the Very Elderly Trial)2 remains a cornerstone in hypertension management among the oldest old. It enrolled 3845 patients aged 80 years or older (mean age, 83.6 y), with sustained SBP greater than or equal to 160 mm Hg. The participants were community‑dwelling, mostly independent, and free from severe cognitive impairment. Treatment with indapamide, with the option of adding perindopril, achieved a mean SBP reduction of 15 mm Hg. Over a median follow‑up of 1.8 years, active treatment led to a 30% reduction in stroke, 64% reduction in heart failure, and 21% reduction in all‑cause mortality, as compared with placebo, with minimal adverse events.2 HYVET demonstrated that antihypertensive treatment was both effective and safe even in the patients older than 80 years, when they were functionally independent and well selected.
The SPRINT‑SENIOR substudy of a larger SPRINT trial (Systolic Blood Pressure Intervention Trial)26 specifically evaluated patients aged 75 years and older (n = 2636), excluding those with diabetes, prior stroke, or nursing home residency. The trial compared an intensive SBP target of below 120 mm Hg to a standard target of below 140 mm Hg. After a median follow‑up of 3.1 years, the intensive group showed a 34% reduction in cardiovascular events and a 33% reduction in all‑cause mortality.26 However, the trial also reported higher rates of hypotension, syncope, and acute kidney injury in the intensive group, especially in the participants with mild frailty. Most participants were ambulatory, with preserved cognitive function and low levels of dependency, thus limiting generalizability to frailer populations.
The STEP (Strategy of Blood Pressure Intervention in the Elderly Hypertensive Patients) trial,25 conducted in China, enrolled 8511 hypertensive patients aged 60 to 80 years (mean age, 66.2 y), excluding those with frailty or severe comorbidities. The participants were randomized to intensive SBP control (target, 110–130 mm Hg) or standard control (130–150 mm Hg). After 3.3 years, intensive treatment resulted in a 26% reduction in stroke, 28% reduction in acute coronary syndrome, and 49% reduction in HF.25 Notably, the trial reported a favorable safety profile, with low incidence of serious adverse events, reinforcing the concept that earlier and tighter BP control is feasible and beneficial in relatively healthy older adults.
Historical trials, such as SHEP (Systolic Hypertension in the Elderly Program)20,27 and Syst‑Eur (Systolic Hypertension in Europe),28 were among the first to demonstrate the benefit of treating ISH in older adults. SHEP included 4736 patients with ISH aged 60 years or older, and showed a 36% reduction in stroke and 27% reduction in cardiovascular events following chlorthalidone‑based therapy.20,27 Syst‑Eur (n = 4227), using nitrendipine with optional angiotensin‑converting enzyme inhibitors (ACEIs) or diuretics, reported a 42% reduction in stroke, 26% reduction in cardiac events, and—uniquely—a 50% reduction in incident dementia.28 These findings underscore the pivotal role of SBP control in preventing both vascular and cognitive outcomes.
Evidence in frail older adults
In contrast to the trials mentioned above, frail and institutionalized older adults are underrepresented in randomized studies. However, several observational and pragmatic studies have explored this domain.
The PARTAGE study (Predictive Analysis of Response to Therapy by Age Group in Elderly),3 a multicenter observational cohort study, included 1130 nursing home residents aged 80 years or older, most of whom were frail and on antihypertensive therapy. A striking finding was that the patients with SBP lower than 130 mm Hg receiving at least 2 antihypertensive drugs had a significantly higher mortality rate, suggesting possible harm from overtreatment in this vulnerable group. This aligns with concerns that low BP in frailty may compromise organ perfusion, particularly cerebral and renal.
The OPTiMiSE trial (Optimising Treatment for Mild Systolic Hypertension in the Elderly),29 a pragmatic randomized controlled study performed in the United Kingdom, enrolled 569 patients aged 80 years and older with controlled SBP (<150 mm Hg) and multimorbidity or frailty. The participants were randomized to continue therapy or undergo deprescribing (removal of 1 antihypertensive agent). At 12 weeks, BP control was maintained, and no increase in adverse events was observed in the deprescribing arm.29 Although short in duration, the trial provides preliminary evidence that medication reduction may be safe and feasible in selected older adults, particularly when polypharmacy and fall risk are concerns.
The DANTE Study Leiden (Discontinuation of Antihypertensive Treatment in Elderly People)30 included 385 individuals aged 60 years or older with mild cognitive impairment and controlled hypertension. The patients were randomized to continuation or withdrawal of antihypertensives. Over 4 months, discontinuation did not worsen cognitive outcomes, and a nonsignificant trend toward fewer falls and orthostatic symptoms was observed in the withdrawal group.30 While the study was not powered to detect hard cardiovascular outcomes, it reinforces the importance of individualizing treatment goals in patients with cognitive impairment.
Two Japanese trials—JATOS (Japanese Trial to Assess Optimal Systolic Blood Pressure in Elderly Hypertensive Patients)21 and VALISH (Valsartan in Elderly Isolated Systolic Hypertension Study)31—explored differing SBP targets in older patients without selecting for frailty status. JATOS (n = 4418; age range, 65–85 y) compared SBP targets of below 140 mm Hg vs below 160 mm Hg and found no significant difference in cardiovascular outcomes, suggesting that more intensive treatment may not yield additional benefit in this age group.21 Similarly, the VALISH trial (n = 3260; age range, 70–84 y) reported no added cardiovascular protection with an SBP target of below 140 mm Hg, as compared with 140–150 mm Hg.31 Importantly, both trials included patients with varying degrees of comorbidity and different functional statuses, reflecting real‑world complexity.
Summary of evidence and implications
Taken together, these trials (Table 1) support a stratified approach to hypertension management in older adults: 1) fit, community‑dwelling patients aged 60–80 years benefit from intensive BP lowering, with consistent reductions in stroke and cardiovascular events (eg, STEP, SPRINT, HYVET); 2) in frail or institutionalized individuals, less aggressive targets or deprescribing may be safer, especially in those with orthostatic hypotension (OH), polypharmacy, or cognitive decline (eg, PARTAGE, OPTiMiSE, DANTE); 3) trials such as JATOS and VALISH provide reassurance that moderate SBP targets (140–150 mm Hg) are acceptable in older adults with comorbidities.
Trial | Year | Participants, n | Population | Frailty status | SBP target, mm Hg | Intervention | Main findings | Study type |
Abbreviations: ↓, decrease; ↑, increase; ACS, acute coronary syndrome; BP, blood pressure; CV, cardiovascular; DM, diabetes mellitus; HF, heart failure; ISH, isolated systolic hypertension; MCI, mild cognitive impairment; OH, orthostatic hypotension; RCT, randomized controlled trial; SR, sustained release; UK, United Kingdom; others, see Figure 1 | ||||||||
HYVET2 | 2008 | 3845 | ≥80 y, community‑dwelling | Fit | <150 | Indapamide SR 1.5 mg; perindopril 2–4 mg vs placebo | ↓ Stroke, ↓ HF, ↓ all‑cause mortality | RCT |
SPRINT‑SENIOR26 | 2016 | 2636 | ≥75 y, high CV risk, no DM | Mostly fit | <120 vs <140 | Intensive vs standard control of SBP (drug treatment) | ↓ CV events & mortality, ↑ syncope & hypotension | RCT (substudy) |
STEP25 | 2021 | 8511 | 60–80 y, Chinese | Fit | 110–130 | Intensive vs standard control of SBP (drug treatment, including olmesartan, amlodipine, and hydrochlorothiazide) | ↓ Stroke, ↓ ACS, ↓ HF | RCT |
SHEP20 | 1985 | 551 | ≥60 y, ISH | Fit | <140 | Chlorthalidone vs placebo; if BP target not met: one of the following drugs in addition to chlorthalidone: reserpine, hydralazine, or metoprolol | ↓ Stroke and CV events | RCT |
Syst‑Eur28 | 1997 | 4695 | ≥60 y, ISH | Fit | <150 | Active treatment: nitrendipine (10–40 mg/d), with or without enalapril (5–20 mg/d) and hydrochlorothiazide (12.5–25 mg/d), as necessary, vs placebo | ↓ Stroke, ↓ HF, ↓ dementia incidence | RCT |
JATOS21 | 2008 | 4418 | 65–85 y, Japanese | Mixed | <140 vs <160 | Strict vs mild treatment, baseline drug: efonidipine hydrochloride | No difference in outcomes | RCT |
VALISH31 | 2008 | 3260 | 70–84 y, Japanese | Mixed | <140 vs 140–150 | Valsartan as first‑line drug; strict (<140 mm Hg) vs mild (140–149 mm Hg) SBP control | No significant benefit of lower BP | RCT |
PARTAGE3 | 2012 | 1126 | ≥80 y, institutionalized | Frail | Observational | – | SBP <130 mm Hg + multiple BP medications = ↑ mortality | Observational |
OPTiMiSE29 | 2020 | 569 | ≥80 y, community‑dwelling, UK | Frail | Deprescribing vs usual | Usual care vs medication reduction (removal of 1 antihypertension drug) | Noninferior BP control, safe short‑term effects | Pragmatic RCT |
DANTE30 | 2015 | 385 | ≥60 y with MCI | Frail with cognitive decline | Withdrawal vs continuation | Discontinuation vs continuation of antihypertensive treatment | ↓ OH and falls, no cognitive worsening | RCT |
Therapeutic targets and treatment approach
When considering older adults, antihypertensive treatment is a major issue. BP lowering is crucial to reduce the risk of cardiovascular events, stroke, HF, and renal impairment. However, given the presence of several hallmarks of the aging process, concomitance of other comorbidities, and functional impairment,32 it should be acknowledged that some unintended consequences of BP lowering, such as hypotension, syncope, and falls, might play a detrimental role in older patients.33 Thus, there is no universal threshold that would apply to all older adults, and different thresholds should be considered, in line with the frailty status of the patient.
Fit older adults are more likely to show better compliance and tolerance to medical therapies, as compared with frail individuals. Therefore, in fit older adults younger than 80 years, medical treatment should be intriduced if SBP is greater than or equal to 140 mm Hg. However, a higher threshold might be applied in older patients; moreover, in the case of institutionalized or severely frail individuals, personalized decisions should be made.1
Frailty status should also guide the BP target during medical treatment, and individual tolerance of the treatment is crucial in all cases.
A SBP target of 130–139 mm Hg is accepted for fit and independent older adults, whereas a less strict target (140–150 mm Hg) is deemed acceptable for patients with a mild grade of frailty. However, in the case of severe frailty or when considering institutionalized patients, symptom management and quality of life should be the main goals, accepting SBP values of 150 mm Hg or higher.1
Several drug classes can be used in older adults. Calcium channel blockers (eg, amlodipine),34 and thiazide diuretics35 are proven to be effective in ISH. ACEIs / angiotensin receptor blockers (ARBs) should be primarily considered in patients with concomitant cardiovascular conditions, such as diabetes, HF, or CKD.33 In the presence of other cardiovascular comorbidities, namely, atrial fibrillation or coronary artery disease, β-blockers are proven to be beneficial. Moreover, the HYVET trial supported the use of thiazide‑like diuretics (eg, indapamide) in individuals aged over 80 years.2
Regular monitoring for orthostatic BP, renal function, and electrolyte levels is essential at any stage of treatment.
Along with medical treatment, different nonpharmacological strategies should be applied and targeted to the patient’s profile and attitude.1,36 Moderate aerobic activity should be regularly performed, and weight loss interventions for overweight and obese patients should be taken into account when indicated.37 Smoking cessation and moderation of alcohol consumption should be pursued, and particular attention should be paid to salt intake in dietary habits.37,38
The main messages of latest guidelines (European Society of Cardiology [ESC], European Society of Hypertension [ESH], American College of Cardiology / American Heart Association) on treatment approaches are summarized in Table 2.
Parameter | 2024 ESC guidelines1 | 2023 ESH guidelines34 | 2017 ACC/AHA guidelines69 | Clinical practice advice |
BP target | 120–129 / 70–79 mm Hg; <140/90 mm Hg in patients with: pretreatment symptomatic OH; age >85 y; clinically significant moderate‑to‑severe frailty; limited predicted lifespan (as low as reasonably achievable principle) | 18–64 y: 130/80 mm Hg; 65–79 y:140/80 mm Hg; >80 y: 140–150/80 mm Hg | 18–64 y: 130/80 mm Hg; 65–79 y: 130/80 mm Hg; >80 y: 130/80 mm Hg | Individualized thresholds, defined based on a comprehensive geriatric assessment, clinical comorbidities, and CV risk profile; general principle of “as low as reasonably achievable” |
Treatment initiation | At BP of 140/90 mm Hg if low CVD risk; at BP of 130–139/80–89 mm Hg if high CVD risk; at BP of 140/90 mm Hg if high CVD risk + any of the following: pretreatment symptomatic OH; age >85 y; clinically significant moderate‑to‑severe frailty; limited predicted lifespan | At BP of 140/90 mm Hg if age <80 y; at SBP of 160 mm Hg if age ≥80 y | At BP of 140/90 mm Hg if low CVD risk; at BP of 130–139/80–89 mm Hg if high CVD risk | Individualized evaluation, defined based on comprehensive geriatric assessment, clinical comorbidities, and the CV risk profile |
Medications | No age‑specific drug indications | Combination therapy, caution with 3‑drug combinations determining too fast / excessive BP reduction in the elderly; no α-blockers | No age‑specific drug indications | Simplified treatment, with frequent medication review |
Frailty | To be evaluated using an easily applicable clinical frailty scale | To be evaluated using an easily applicable clinical frailty scale + comprehensive geriatric assessment | To be evaluated (no preferred scale) | To be evaluated using an easily applicable clinical frailty scale + comprehensive geriatric assessment; baseline evaluation and reassessment every 6 months (earlier in the case of clinical instability) |
Challenges in older adults
Managing hypertension in older adults presents unique challenges, largely driven by age‑related physiological changes, comorbidity burden, functional impairment, and increased vulnerability to treatment‑related adverse events.32
Although the SPRINT trial showed that targeting SBP below 120 mm Hg in older adults (≥75 y) can significantly reduce major cardiovascular events and mortality,26 these findings must be interpreted with caution in real‑world settings. In fact, data from the TILDA study (Irish Longitudinal Study on Ageing)33 demonstrated that older adults meeting the SPRINT inclusion criteria experienced 5‑fold higher rates of injurious falls and syncope than reported in the trial, raising concerns about the external validity of such strict BP targets in frail or functionally impaired individuals.39
The complexity of hypertension management in the elderly requires a nuanced, individualized approach, based on a comprehensive geriatric assessment.
Cognitive impairment and dementia risk
The relationship between BP control and cognitive outcomes is complex, and separate considerations should be taken into account in dementia prevention or in patients with established cognitive disorders. In the first setting, BP control is crucial for risk factor management. Studies suggest that aggressive BP lowering may compromise cerebral perfusion, particularly in patients with existing cognitive impairment or impaired autoregulation.40 However, a recent meta‑analysis involving over 28 000 patients showed that a SBP/DBP reduction by 10/4 mm Hg, respectively, was associated with a significant decrease in dementia incidence.41
On the other hand, in patients with established dementia, firm BP control is potentially harmful, and most guidelines recommend less strict BP targets, prioritizing safety and quality of life over strict cardiovascular prevention. Close monitoring is essential to avoid excessive BP lowering, which may accelerate cognitive decline due to hypoperfusion.
Polypharmacy and therapeutic complexity
Older hypertensive patients often receive multiple medications. Polypharmacy increases the risk of drug–drug interactions, adverse events, and nonadherence, all of which can undermine BP control and increase morbidity.42,43
Medication review
A medication review is warranted in all older individuals with hypertension to prevent the occurrence of significant adverse drug reactions.
Polaczyk et al44 examined a population of 1000 patients and reported that those with hypertension and other comorbidities commonly presented multiple drug intolerance syndrome, which was shown to be more frequent among women and individuals with concomitant therapies, such as analgesics, β-blockers, antiplatelet drugs, and antibiotics.
Medication classes such as α-blockers, centrally‑acting drugs, and nondihydropyridine calcium channel blockers deserve particular attention because of their higher burden on the central nervous system and orthostatic effects.
Deprescribing strategies, such as those tested in the OPTiMiSE trial,29 may offer a safe and effective way to reduce treatment burden in selected patients.45 The use of various tools, for example, the STOPP/START criteria46 and the Beers list,47 is strongly encouraged to optimize medication regimens. Early identification of patients at a high risk of treatment‑related adverse effects is key, as highlighted by a recent expert review advocating for proactive deprescribing protocols.45
Frailty and end of life
Frailty is a key issue in the management of hypertension and a significant number of other conditions among older people.48 It is defined as a state of reduced physiological reserve and increased vulnerability to adverse health outcomes.49 The relationship between frailty and hypertension is dual and challenging; along with other comorbidities and conditions, hypertension can contribute to cumulating deficits and increase frailty status (and noteworthy, hypertension diagnosis is included in cumulative models)50,51; on the other hand, facing hypertension in frail individuals is a significant challenge.52
There is strong evidence that pinpoints the role of frailty as a strong predictor of mortality and poor cardiovascular outcomes.53 However, a relatively small number of trials on BP‑lowering approaches included a significant proportion of frail patients.1 Nevertheless, the latest guidelines1,34 recommend periodic assessment of frailty level and functional status to recognize patient needs and to guide treatment decisions.
There is a need for agreement on frailty evaluation. Nowadays, different frailty models and scales can be applied to estimate frailty status, some of which are too complex for routine clinical practice. The latest ESC guidelines endorse the use of electronic scales (eg, the electronic frailty index50), and both ESC and ESH guidelines1,34 suggest the use of the Rockwood Clinical Frailty Scale,51 which represents a fairly applicable and standardized tool to evaluate frailty in older adults (Supplementary material, Table S1).
In frail individuals with limited life expectancy, multimorbidity, or advanced disease, the clinical focus may shift from strict BP targets to symptom control, maintenance of function, and preservation of autonomy. In such cases, palliative care principles and shared decision‑making should guide antihypertensive management.
Lastly, social and environmental determinants—such as cognitive barriers, social isolation, poor nutrition, and caregiver support—can influence adherence and treatment safety, and should be routinely assessed as part of comprehensive care.
Orthostatic hypotension
OH is a common and often underdiagnosed condition in the elderly, affecting over 20% of individuals aged over 70 years,54 with prevalence higher than 40% when considering older hospitalized individuals.55,56 It is defined by a SBP reduction greater than or equal to 20 mm Hg or DBP reduction greater than or equal to 10 mm Hg upon standing.1 OH is more prevalent among older hypertensive individuals,57 partly due to age‑related baroreflex dysfunction, reduced vascular compliance, and altered autonomic regulation.58-61 Pharmacological overtreatment can further exacerbate OH, as shown in the PARTAGE study.3,57
OH is associated with an increased risks of falls, fractures, syncope, and cardiovascular mortality, and may coexist with postprandial hypotension, an underrecognized cause of syncope in frail older adults.62 In fact, OH can be recognized in almost 1 out of 4 older adults reporting to an emergency department for syncope, and in 1 out of 5 presenting due to trauma.56 As such, routine evaluation for OH—including orthostatic BP measurements—should be integrated into hypertension management in this population.
Renal function and electrolyte imbalances
Antihypertensive drugs frequently impact renal hemodynamics and electrolyte balance. ACEIs and ARBs, though beneficial in patients with cardiovascular and renal comorbidities, can lead to an increased serum levels of creatinine and hyperkalemia, particularly in the individuals with CKD. Thiazide diuretics may induce hypokalemia and hyponatremia, which are more frequent in older patients with impaired renal function.1,63
Mild hyponatremia, although often asymptomatic, has been associated with increased risks of falls, fractures, and cognitive impairment.64 Similarly, hyperkalemia can predispose to life‑threatening arrhythmias, particularly in the patients treated with RAAS inhibitors.65 Therefore, careful monitoring of renal function and electrolyte levels is essential in older patients receiving antihypertensive therapy, especially during initiation or dose escalation.
Data from TILDA further highlight that over 80% of older adults with CKD also have hypertension, but more than half are undertreated, often due to concerns over adverse effects.66
Uncontrolled hypertension
Uncontrolled hypertension is frequent in older patients, particularly those presenting to emergency departments, of whom up to 1 in 4 has been shown to exhibit BP disorders.67 Among patients with uncontrolled hypertension, older individuals frequently have recurrences and concomitant electrolyte imbalances.67
Noteworthy, the age‑related pathophysiological changes, along with increased arterial stiffness and reduced arterial wall compliance, may increase the risk of acute BP elevation, complications, and less predictable magnitude of treatment response; thus, the use of easily titratable agents should be prioritized.68
It is of paramount importance to perform a comprehensive evaluation of the patient’s condition and to establish the potential presence of a triggering factor that should be addressed and managed.1 Timely evaluation of organ(s) damage may guide any other interventions. In the case of acute BP raise, clinicians should plan the magnitude of BP lowering and the appropriate time to pursue it.1
Conclusions
Arterial hypertension is a frequent finding among older adults, and due to the pathophysiological changes related to the aging process, the most frequent pattern is ISH. Evidence strongly supports BP reduction in fit older individuals, with significant benefits in terms of stroke prevention and mortality reduction. Trials such as HYVET, SPRINT‑SENIOR, and STEP confirm the safety and efficacy of intensive BP control in this population. In contrast, frail or institutionalized individuals often experience adverse outcomes with overly aggressive BP lowering. The PARTAGE, OPTiMiSE, and DANTE trials underscore the importance of balancing benefits with risks, such as hypotension, falls, and cognitive decline. Although appropriate treatment is crucial for cardiovascular event prevention, it should be noted that in older adults, tailored treatment based on the patient’s frailty status is of paramount importance, and several challenges related to older age (eg, OH, syncope, and falls) should always be considered.
Clinical decisions should therefore be based on a comprehensive geriatric assessment, including frailty evaluation, and patient preferences, with treatment goals prioritizing function, safety, and quality of life. Future randomized studies should include more frail and cognitively impaired patients to fill current knowledge gaps.
- McEvoy JW, McCarthy CP, Bruno RM, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024; 45: 3912‑4018. | Crossref
- Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008; 358: 1887‑1898. | Crossref
- Benetos A, Labat C, Rossignol P, et al. Treatment with multiple blood pressure medications, achieved blood pressure, and mortality in older nursing home residents: the PARTAGE study. JAMA Intern Med. 2015; 175: 989‑995. | Crossref
- NCD Risk Factor Collaboration (NCD‑RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population‑representative studies with 104 million participants. Lancet. 2021; 398: 957‑980. | Crossref
- Benetos A, Petrovic M, Strandberg T. Hypertension management in older and frail older patients. Circ Res. 2019; 124: 1045‑1060. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION