In October 2024, a 34‑year‑old man with no significant medical history was hospitalized twice in an orthopedic department due to lower limb pain and recurrent, extensive hematomas within the quadriceps muscles. He denied systemic symptoms, such as fever or weight loss. On both occasions, large volumes of blood were evacuated from the quadriceps muscles, but no samples were submitted for histopathologic examination.
Following the second evacuation, the patient developed life‑threatening anemia (hemoglobin, 6 g/dl; reference range [RR], 13.7–16.5 g/dl), requiring transfer to a department of trauma and orthopedic surgery. He received multiple transfusions of red blood cells and fresh frozen plasma. Computed tomography (CT) angiography showed hematomas in both quadriceps (Figure 1A), the right gluteus maximus, and left pelvic girdle muscles, all with signs of active bleeding.
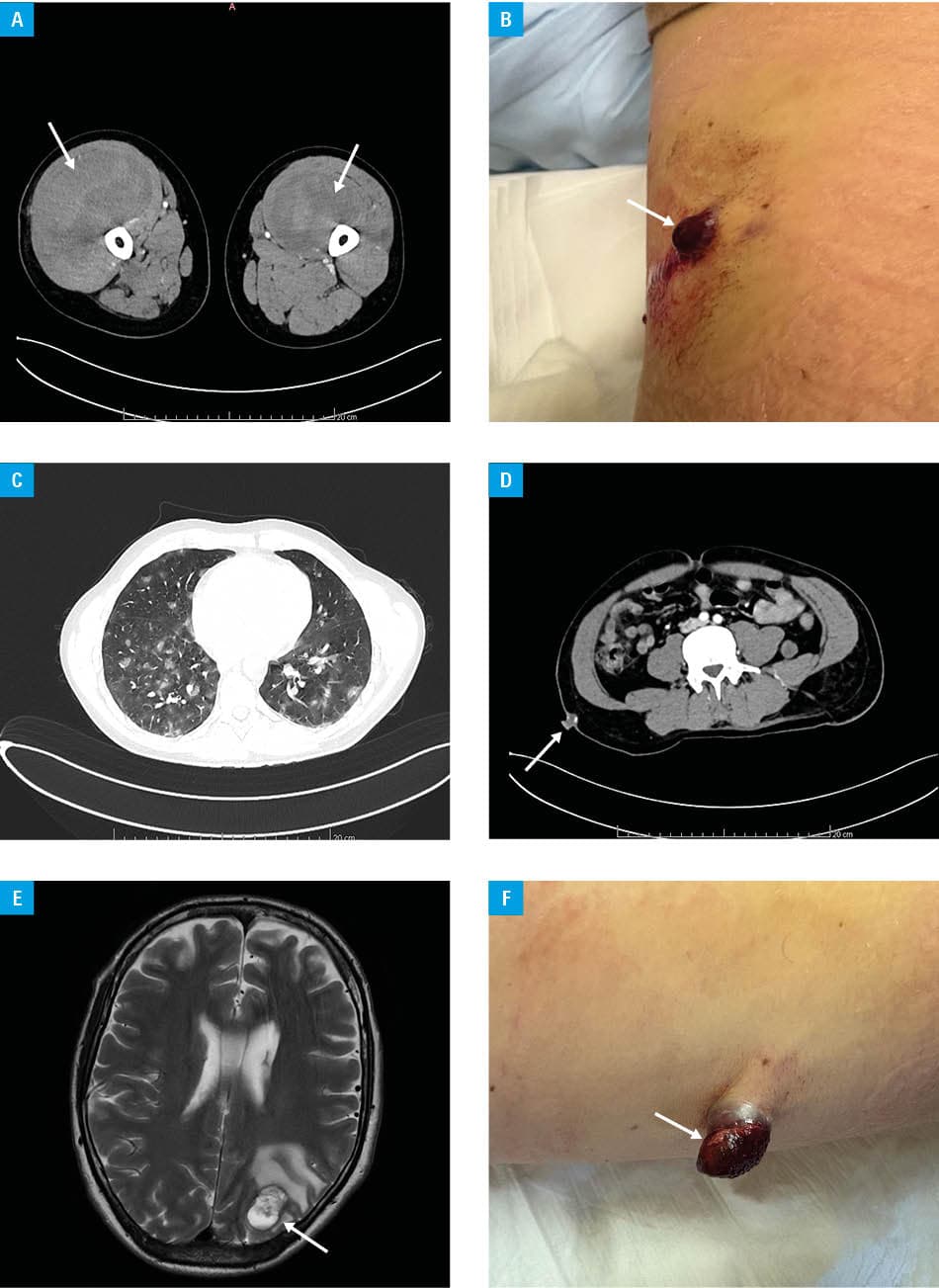
The patient was referred to a department of internal medicine, metabolic diseases, and angiology. Physical examination showed widespread subcutaneous hematomas and a flat hemorrhagic lesion in the right lumbar region (Figure 1B). Laboratory tests indicated severe thrombocytopenia (platelet count, 8 × 10³/μl; RR, 135–350 × 10³/μl), prolonged prothrombin time (26.2 s; RR, 9.4–13.4 s), a low fibrinogen concentration (0.47 g/l; RR, 1.8–3.5 g/l), and a highly elevated D‑dimer level (>36 800 ng/ml; RR, 0–500 ng/ml), consistent with disseminated intravascular coagulation. Sepsis was excluded; mild leukocytosis was attributed to corticosteroid use. Bone marrow biopsy ruled out hematologic malignancy.
Contrast‑enhanced CT of the chest, abdomen, and pelvis identified bilateral pulmonary ground‑glass opacities (suggestive of alveolar hemorrhage; Figure 1C), a soft tissue lesion in the right lumbar region (Figure 1D), a mass in the left retroperitoneum, and multiple muscular hematomas. Brain magnetic resonance imaging showed hemorrhagic metastases with cerebral edema (Figure 1E) and a lesion in the C4 vertebra.
During hospitalization, the lumbar skin lesion progressed into a 3–4 cm cauliflower‑like tumor (Figure 1F). The patient received corticosteroids, mannitol, immunoglobulins, and transfusions (red cells, plasma, platelets, and cryoprecipitate). This stabilized blood coagulation sufficiently to allow surgical excision of the skin lesion.
Histopathologic analysis confirmed angiosarcoma. The patient was referred to an oncology department and started on doxorubicin and ifosfamide chemotherapy along with radiotherapy. After 3 cycles, coagulation normalized, and the hemoglobin level remained stable.
Angiosarcoma is a rare, aggressive vascular malignancy with a poor prognosis and a recognized association with disseminated intravascular coagulation. Its clinical presentation may resemble spontaneous or chronic hematomas, frequently contributing to delayed diagnosis.1-3 Lymphangiosarcoma, an exceptionally rare subtype originating from lymphatic endothelium, constitutes only a small proportion of soft tissue sarcomas. The principal risk factor is chronic lymphedema, most often following mastectomy with axillary dissection and / or radiotherapy, although congenital, infectious, or traumatic lymphatic obstruction may also predispose to its development. Clinically, lymphangiosarcoma may present with bruise‑like or violaceous skin lesions, nonhealing ulcers, enlarging nodules, or soft‑tissue masses that bleed or ulcerate, and can mimic hematomas or cellulitis. The disease typically metastasizes early, most commonly to the lungs, liver, bone, and brain.4,5
This case underscores the importance of histopathologic evaluation of unexplained or recurrent hematomas, especially when bleeding is disproportionate to the trauma.
- Rosen EA, Vallurupalli M, Choy E, et al. Management of disseminated intravascular coagulation in a patient with hepatic angiosarcoma: a case report. Medicine (Baltimore). 2018; 97: e13321. | Crossref
- Babińska A, Hellmann A, Skowronek F, et al. Unveiling the enigma of primary angiosarcoma of the adrenal gland: a rare and aggressive malignancy. Pol Arch Intern Med. 2024; 134: 16687. | Crossref
- Alshalfan R, Almalki S, Alnasser M, Alhaqbani A. Case report: chronic expanding hematoma becomes angiosarcoma. J Surg Case Rep. 2025; 2025: rjaf063. | Crossref
- Young RJ, Brown NJ, Reed MW, et al. Angiosarcoma. Lancet Oncol. 2010; 11: 983‑991. | Crossref
- Mark RJ, Poen JC, Tran LM, et al. Angiosarcoma: a report of 67 patients and a review of the literature. Cancer. 1996; 77: 2400‑2406. | Crossref
ARTICLE INFORMATION