High‑risk percutaneous coronary interventions (PCIs) are complex procedures that often require the use of mechanical circulatory support (MCS) devices, such as a percutaneous microaxial blood pump, to mitigate the risk of hemodynamic collapse. However, MCS devices require large‑bore arterial access, most commonly via the common femoral artery (CFA), making vascular complications, primarily bleeding or thromboembolic events, a significant concern.1-3
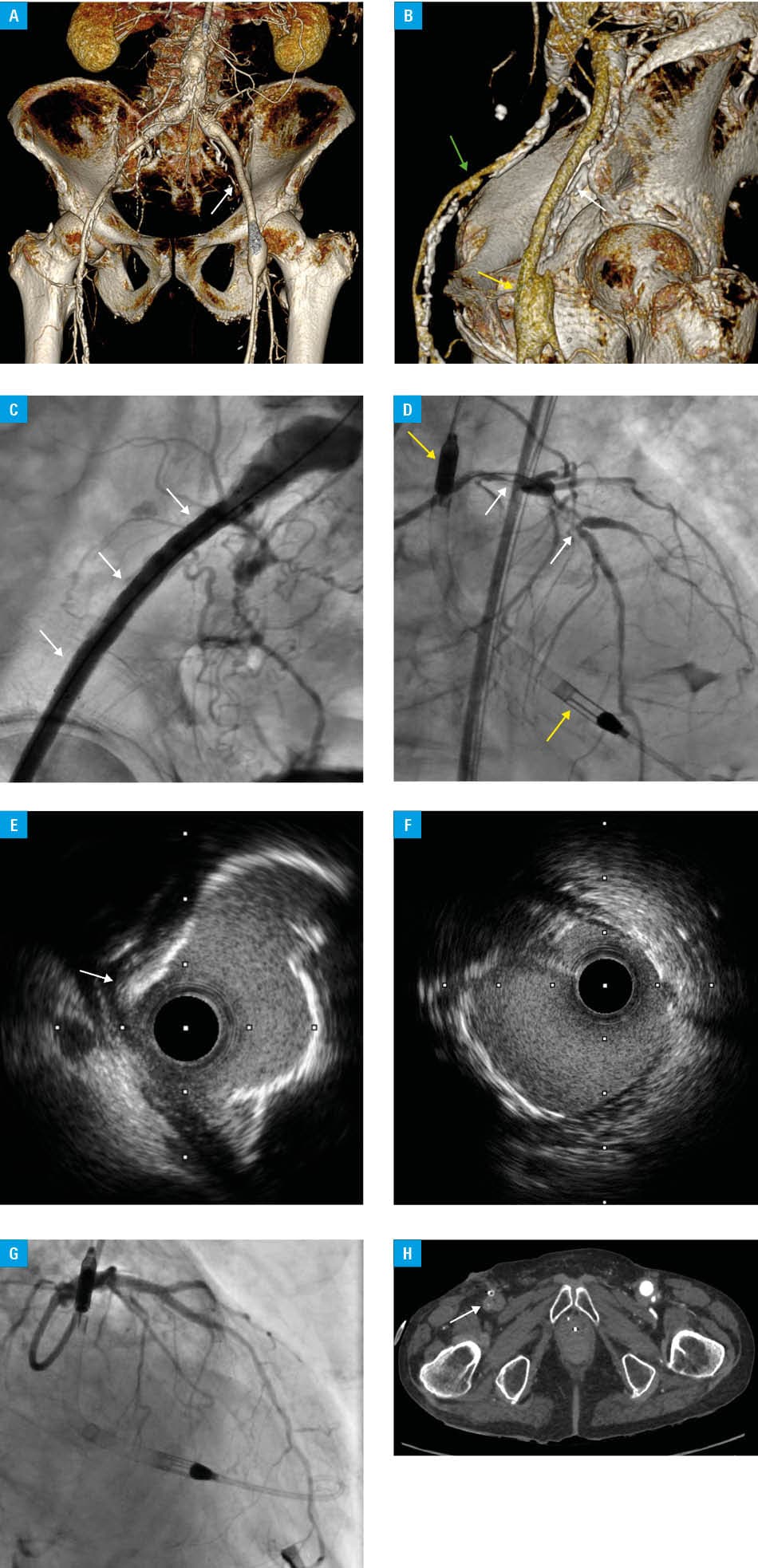
A 77‑year‑old man with a history of arterial hypertension, mixed hyperlipidemia, and advanced atherosclerosis already treated with left‑sided iliofemoral bypass (Figure 1A and 1B) was referred to a cardiology department with a diagnosis of non–ST‑segment elevation myocardial infarction. Transthoracic echocardiography performed on admission showed a dilated left ventricle (60 mm) with decreased left ventricular ejection fraction of 20%. Coronary angiography identified critical stenoses of the left main (LM) and left anterior descending (LAD) coronary arteries on bifurcation with the first diagonal branch (D1), diffuse borderline stenoses in the left circumflex artery, and chronic total occlusion of the right coronary artery. The heart team disqualified the patient from coronary artery bypass grafting and qualified him instead for LM/LAD and LAD /D1 PCI, protected by MCS. Out of the possible MCS options, Impella CP (Abiomed, Danvers, Massachusetts, United States) was selected as the option providing the best hemodynamic support, especially during prolonged and complex procedures. Given the multilevel peripheral atherosclerosis with an aneurysm at the distal implantation site of the graft identified on computed tomography angiography (CTA), open right femoral access (supported by a vascular surgeon) was opted for. Firstly, a peripheral stent (Zilver, Cook Medical, Bloomington, Indiana, United States; 7 mm × 80 mm) was implanted in the right CFA (Figure 1C), preceding the insertion of the Impella CP peel‑away sheath (14F × 25 cm), through which single access was provided to minimize the risk of vascular complications. Due to massive calcification found on intravascular ultrasound (IVUS), rotational atherectomy (6 passages, 3 times with a 1.25‑mm burr and 3 times with a 1.5‑mm burr), followed by provisional stenting of LM/LAD and LAD/D1 with the implantation of 2 drug‑eluting stents were performed, showing satisfactory angiographic and IVUS results (Figure 1D–1G). Following the onset of acute right lower limb pain 1 hour after the procedure, CTA was performed, showing occlusion of the right CFA (Figure 1H), which was immediately treated endovascularly, achieving reperfusion and symptom relief. Further hospitalization was uneventful, and the patient was discharged in a stable condition, without coronary complaints or signs of lower limb ischemia.
MCS devices can be safely and effectively used in high‑risk PCIs; however, there is no compelling evidence supporting the superiority of such management over optimal medical therapy alone are lacking, and more targeted research is required.1,3,4 Vascular access remains a challenge in device‑supported PCIs, with significant atherosclerosis being a considerable limitation. Here, we demonstrated that nonstandard access methods for Impella CP implantation can be used, though complications are still possible, underlining the importance of cooperation with other medical specialties. It should be noted that this approach remains off‑label and may not be applied in all patients with peripheral vascular disease, as the anatomical variability considerably limits possible access options, requiring individualized planning.
- Alqarqaz M, Basir M, Alaswad K, O’Neill W. Effects of impella on coronary perfusion in patients with critical coronary artery stenosis. Circ Cardiovasc Interv. 2018; 11: e005870. | Crossref
- Masiero G, Arturi F, Panza A, Tarantini G. Mechanical circulatory support with impella: principles, evidence, and daily practice. JCM. 2024; 13: 4586. | Crossref
- Skorupski WJ, Pietrasik A, Gąsecka A, et al. Short- and long‑term outcomes of impella‑protected, high‑risk, elective PCI in patients with multivessel coronary disease and low ejection fraction ‑ Polish Impella Registry. Cardiol J. 2025; 32: 248‑257. | Crossref
- Ferro E, Kim J, Lalani C, et al. Mechanical circulatory support for complex, high‑risk percutaneous coronary intervention. https://eurointervention.pcronline.com/article/mechanical‑circulatory‑support‑for‑complex‑high‑risk‑percutaneous‑coronary‑intervention. Accessed July 17, 2025. | Crossref
ARTICLE INFORMATION