Early use of sodium-glucose cotransporter 2 inhibitors after acute myocardial infarction: a systematic review and meta-analysis of randomized controlled trials
Key words: acute myocardial infarction, dapagliflozin, empagliflozin, heart failure, SGLT2 inhibitors

 CC BY 4.0
CC BY 4.0
Early use of sodium-glucose cotransporter 2 inhibitors after acute myocardial infarction: a systematic review and meta-analysis of randomized controlled trials
Introduction: Acute myocardial infarction (AMI) continues to be a primary cause of posthospitalization heart failure (HF), severely impacting morbidity, health care resource consumption, and mortality rates.
Objectives: This meta‑analysis sought to assess the efficacy and safety of the early introduction of sodium‑glucose cotransporter 2 inhibitors (SGLT2is) in patients hospitalized for AMI, irrespective of previous HF or diabetes history.
Patients and methods: A comprehensive search was carried out, up until June 10, 2025, in 6 major databases, including randomized controlled trials (RCTs) assessing SGLT2is that were started within 14 days of hospitalization for AMI.
Results: Seven RCTs were included (n = 11 405) comparing SGLT2is with placebo or standard medical therapy without SGLT2is, with follow‑up ranging from 6 to 18 months. The commencement of SGLT2i therapy markedly diminished the odds of HF hospitalization (odds ratio [OR], 0.71; 95% CI, 0.58–0.86; P = 0.004). No notable changes were detected in all‑cause mortality (OR, 1.05; 95% CI, 0.77–1.43), cardiovascular mortality (OR, 1.04; 95% CI, 0.83–1.3), major adverse cardiovascular events (OR, 0.94; 95% CI, 0.85–1.05), recurrent MI (OR, 1.12; 95% CI, 0.73–1.72), or stroke (OR, 0.58; 95% CI, 0.26–1.27).
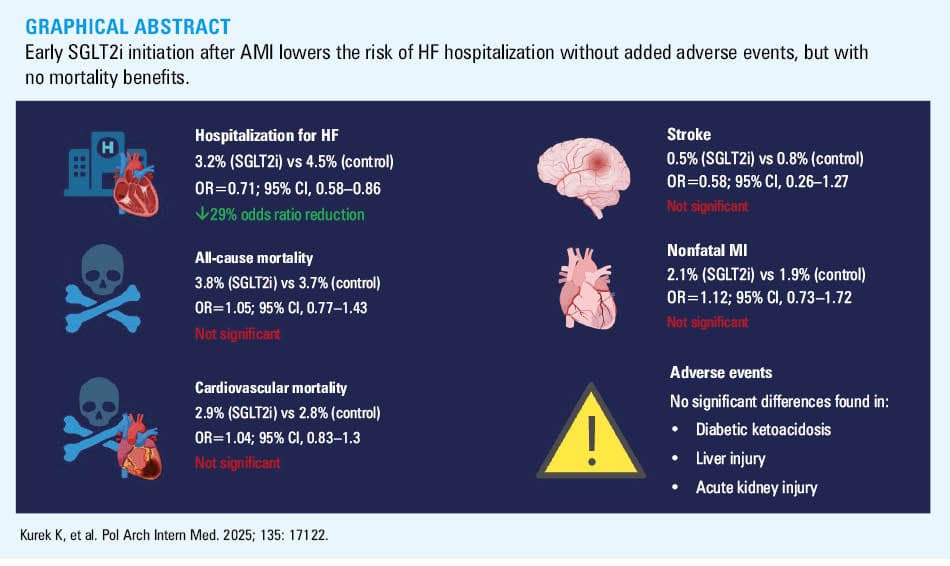
Conclusions: Early initiation of SGLT2is post‑AMI significantly reduces the risk of subsequent HF hospitalization without increasing the risk of adverse events. However, no mortality benefit was observed. These findings support the selective use of SGLT2is in post‑AMI patients at a high risk for HF, while highlighting the need for further large‑scale trials to assess long‑term outcomes and refine patient selection.
What's new?
This is the first meta‑analysis focusing exclusively on the early commencement of sodium‑glucose cotransporter 2 inhibitors (SGLT2is) in patients admitted for acute myocardial infarction (AMI). This study, analyzing data from over 11 000 patients across 7 randomized controlled trials, indicated that SGLT2is dramatically decreased the incidence of heart failure (HF) hospitalization by 29%, as compared with placebo. This advantage was evident even in those without a history of HF or diabetes. Nonetheless, no substantial changes were observed in all‑cause or cardiovascular mortality, severe adverse cardiovascular events, recurrent MI, or stroke. Safety outcomes were analogous in the treatment and control groups. The findings emphasize the potential of SGLT2is as a targeted approach to avoid post‑AMI HF, while highlighting the necessity for more trials to elucidate mortality impacts and optimize patient selection.
Introduction
Cardiovascular disease remains the leading cause of morbidity and mortality worldwide, with coronary artery disease as its primary contributor.1 Despite significant therapeutic advances over the past 2 decades, acute myocardial infarction (AMI) continues to represent the most common cause of heart failure (HF).2 Based on the temporal relationship between AMI and the onset of HF, 3 distinct clinical phenotypes can be identified: 1) HF present at the time of AMI, 2) HF developing during the index hospitalization, and 3) HF emerging after discharge.
Postdischarge HF is particularly prevalent. It is diagnosed in approximately 13% of patients within 30 days, and in 20%–30% within 1 year after discharge following AMI.3,4 The highest incidence is observed within the first month postinfarction, followed by a stable annual rate of 1.3%–2.2%.5 Recent evidence indicates that in the patients who develop HF within the 3 months post‑MI, the median (interquartile range [IQR]) time to diagnosis is as short as 12 (6–27) days.6 Notably, even among those with preserved left ventricular ejection fraction (LVEF; ≥50%) during index hospitalization, the 12‑month incidence of HF remains substantial, at 11.8%, which exceeds the rate of recurrent MI 3‑fold (3.5%).7,8 In a cohort of patients without prior HF, 23.8% developed incident HF within 3 months of discharge, with distributions across EF strata as follows: 42.2% with EF below 40%, 26.7% with EF at 41%–49%, and 31.1% with EF equal to or above 50%. Importantly, the onset of HF, regardless of EF, was associated with a higher risk of death and hospitalization (both P <0.001).
Sodium‑glucose cotransporter 2 inhibitors (SGLT2is) have demonstrated robust efficacy in reducing adverse outcomes in patients with type 2 diabetes (T2D), chronic kidney disease (CKD), and HF,9 and their use is endorsed in current guidelines for post‑MI patients with such comorbidities.10 However, the utility of SGLT2is in the patients without pre‑existing HF, T2D, or CKD remains uncertain. As emphasized in the 2021 European Society of Cardiology HF guidelines,11 it has yet to be determined whether SGLT2is improve outcomes in patients with acute coronary syndrome who do not have HF or diabetes.
Although accumulating evidence supports the cardiovascular benefits of SGLT2is that extend beyond glycemic control, most major trials have excluded patients with recent MI. Moreover, a recent randomized trial evaluating SGLT2is in the post‑MI setting has yielded neutral or inconclusive results.12 Therefore, the efficacy and clinical value of SGLT2is in this particular patient population remain unclear. These uncertainties underscore the need for further investigation to assess whether the mechanistic advantages of SGLT2 inhibition translate into meaningful clinical benefits in the early post‑MI phase.
This meta‑analysis aimed to assess the efficacy and safety of SGLT2is, as compared with placebo, initiated during hospitalization and administered as adjunctive therapy in adult patients with AMI. The predefined outcomes of interest included all‑cause mortality, major adverse cardiovascular events (MACEs), cardiovascular mortality, hospitalization for HF, recurrent nonfatal MI, and stroke.
Patients and methods
Study design
The 2020 PRISMA guidelines13 were followed in the reporting of this study, which was carried out as a systematic review and meta‑analysis in compliance with the Cochrane Handbook for Systematic Reviews of Interventions.14 The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD420251073395). Ethical approval and informed consent were not necessary because the analysis was solely based on aggregate data from previously published randomized controlled trials (RCTs) and did not include identifiable health information, experimental interventions, or patient data.
Eligibility criteria
The selection of studies was directed by the PICOS (Population, Intervention, Comparator, Outcomes, Study design) framework to guarantee methodological rigor and pertinence to the study issue. We incorporated studies involving adult patients (aged ≥18 y) hospitalized for AMI, including both ST‑segment elevation myocardial infarction (STEMI) and non–ST‑segment elevation myocardial infarction (NSTEMI). The trials were eligible regardless of the presence or absence of baseline comorbidities, such as T2D, CKD, or HF, as long as SGLT2is were commenced in the context of the index AMI.
The studies that met the eligibility requirements assessed SGLT2is, such as empagliflozin, dapagliflozin, canagliflozin, or ertugliflozin. The intervention had to be started either within 14 days of discharge or during the index hospitalization for AMI. Regarding the comparator, either a placebo or conventional medical treatment without SGLT2i initiation was given to the control group. To be eligible for this meta‑analysis, the studies had to report at least 1 of the following predetermined clinical outcomes: hospitalization for HF as a primary outcome or all‑cause mortality, cardiovascular mortality, MACE, recurrent nonfatal MI, or stroke as secondary outcomes. We only included RCTs published in peer‑reviewed journals. The studies were excluded if they did not meet the criteria for RCT design. In particular, we did not include case series, nonrandomized trials, single‑arm studies, observational studies, or trials with no comparator group. The studies in which SGLT2i therapy was started more than 14 days after the index AMI were also disqualified, as were the trials that only included patients who had established chronic HF at baseline. We eliminated the studies that only reported on surrogate end points, such as N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) levels or echocardiographic parameters, without corresponding clinical outcomes (eg, hospitalization for HF or cardiovascular mortality), in order to guarantee clinical relevance of the included outcomes. In the cases of data overlap from the same study population, only the most thorough, peer‑reviewed, and recent publication was included in the analysis.
Data sources and search strategy
The Cochrane Central Register of Controlled Trials (CENTRAL), PubMed / MEDLINE, Embase, Web of Science, Scopus, and ClinicalTrials.gov were the 6 main electronic databases searched. The search was limited to studies published in English, with no restrictions on the publication status or geographic location, and it included all records from the database creation until June 10, 2025.
The search strategy was developed by combining 2 text key words associated with “SGLT2i”, and “acute myocardial infarction” with controlled vocabulary (such as MeSH and Emtree terms). Details of the search strategies for each database are presented in Supplementary material, Table S1. To enhance sensitivity of the search and ensure that no eligible studies were missed, the reference lists of all included articles and relevant systematic reviews or meta‑analyses were manually screened. This additional step allowed us to identify potentially eligible studies that may not have been indexed in the searched electronic databases or published in peer‑reviewed journals. Covidence (Veritas Health Innovation, Melbourne, Australia), a web‑based systematic review platform, was used to facilitate dual independent screening and to streamline data management in accordance with best practices in evidence synthesis.
Study selection and data extraction
For deduplication, all the recovered records were loaded into a reference management program (EndNote X9, Clarivate Analytics, Philadelphia, Pennsylvania, United States). Two reviewers (KK and MP), who had both previously conducted systematic reviews, independently screened the titles and abstracts. The articles that satisfied the initial inclusion requirements or whose applicability could not be definitively ruled out were obtained for full‑text evaluation. The full texts were evaluated for eligibility independently by the same reviewers. Any disagreements regarding the selection of studies at any point were settled through discussion or, if required, by a third senior reviewer (LS).
The selection procedure was carried out in accordance with the PRISMA 2020 guidelines, and a PRISMA flow diagram was used to present the number of records that were found, screened, excluded, and included, along with justifications for any full‑text exclusions.
Data from all included studies were extracted utilizing a designed and piloted standardized extraction form. The following essential variables were gathered: study identifiers (authors, year of publication, country); study design and setting; sample size and baseline characteristics of the study population; inclusion and exclusion criteria; type and dosage of SGLT2i used; timing of SGLT2i initiation (eg, during hospitalization or early post‑discharge); comparator intervention; duration of follow‑up; reported clinical outcomes, including definitions and effect measures; funding sources; and declarations of conflict of interest.
To reduce bias and guarantee accuracy, the data extraction was carried out independently and in duplicate by both reviewers. When information was unclear or missing, attempts were made to contact the corresponding authors for clarification. Before quantitative synthesis, the senior reviewer cross‑checked the extracted data to preserve uniformity and guarantee data integrity across studies.
Risk of bias and quality assessment
The Cochrane Risk of Bias 2.0 (RoB 2.0) tool15 was used to evaluate the methodological quality of all included RCTs. The RoB 2.0 measures the risk of bias in 5 standard domains: 1) the randomization process, 2) deviations from intended interventions, 3) missing outcome data, 4) measurement of the outcome, and 5) selection of the reported results. Two reviewers independently carried out the evaluation, and each trial was assessed using the RoB 2.0 template that best suited its design (eg, individually randomized, parallel‑group trials). To guarantee consistency and openness in judgment, any disputes were settled through discussion or, if necessary, by the senior investigator (LS). An overall risk‑of‑bias rating was created for each study by combining the evaluations of each domain, which were classified as having “low risk of bias,” “some concerns,” or “high risk of bias”.
The GRADE (Grading of Recommendations Assessment, Development, and Evaluation) framework was used to assess the certainty of evidence for each primary and secondary outcome, in addition to the risk of bias.16 This method rates the quality of evidence as high, moderate, low, or very low by taking into account study limitations, inconsistency, indirectness, imprecision, and the possibility of publication bias. The GRADE evaluations were carried out twice, and disagreements were settled by consensus.
Statistical analysis
All statistical analyses were conducted in accordance with established guidelines for meta‑analyses of RCTs. As summary effect estimates, odds ratios (ORs) and matching 95% CIs were computed for every dichotomous outcome. The DerSimonian–Laird method was used to apply a random‑effects model to account for expected methodological and clinical heterogeneity across studies. The I² statistic quantified statistical heterogeneity among the included studies by expressing the proportion of overall variation across studies that is attributable to heterogeneity rather than chance. The Cochran Q test was used to evaluate statistical heterogeneity, with P value below 0.1 indicating significance. Low, moderate, and high heterogeneity were the respective interpretations for thresholds of 25%, 50%, and 75%. The publication bias was assessed quantitatively using the Egger regression test, and visually by looking at funnel plots when there were at least 10 studies available for a particular outcome. A P value of less than 0.1 was deemed suggestive of asymmetry. The robustness of the primary findings was tested in prespecified sensitivity analyses. These involved excluding studies with a high risk of bias and performing subgroup analyses according to the duration of follow‑up, the presence of comorbid diabetes, and the timing of SGLT2i initiation (in‑hospital vs early postdischarge). We also performed leave‑one‑out analyses, where appropriate, to evaluate the impact of individual studies on the pooled estimates. Stata version 18.0 (StataCorp LLC, College Station, Texas, United States) and RevMan version 5.4 packages (the Cochrane Collaboration, London, United Kingdom) were used for all meta‑analyses. To show the effect sizes and 95% CI graphically, forest plots were created. Unless otherwise noted, all primary analyses were deemed significant if the 2‑sided P value was below 0.05.
Results
Study selection
A total of 6762 records were identified via electronic database searches. Following the elimination of duplicates, 3127 distinct records were evaluated based on the title and abstract. A total of 173 full‑text papers were evaluated for eligibility. In total, 7 RCTs, comprising 11 405 patients, satisfied the inclusion criteria, and were incorporated into the final meta‑analysis (Figure 1).12,17-22

Study characteristics
The included studies were published between 2020 and 2024, with individual sample sizes ranging from 108 to 6522 participants. The follow‑up duration ranged from 6 to 18 months. Across trials, SGLT2is were initiated during hospitalization for AMI or within 14 days postdischarge. The agents evaluated included empagliflozin (in 5 trials) and dapagliflozin (in 2 trials). Baseline characteristics were generally well balanced between the treatment and control groups. However, the patients in the SGLT2i group had a slightly lower prevalence of prior MI (10.5% vs 11.9%; P = 0.02) and a marginally higher mean body mass index (27.6 vs 27.4 kg/m²; P <0.001), though the difference was not clinically significant. Detailed study and patient characteristics are summarized in Table 1 and Supplementary material, Table S2.
Study | Country | Study group | Sample size, n | Age, y, mean (SD) | Men, n (%) | BMI, kg/m2, mean (SD) | Hypertension, n (%) | T2D, n (%) | Dyslipidemia, n (%) | Previous MI, n (%) |
Abbreviations: BMI, body mass index; MI, myocardial infarction; NS, not specified; T2D, type 2 diabetes | ||||||||||
Adel et al17 | Iran | Empagliflozin | 45 | 54.9 (4.6) | 27 (60) | NS | 26 (57.8) | NS | NS | NS |
Control | 48 | 57.7 (4.2) | 29 (60.4) | NS | 32 (66.7) | NS | NS | NS | ||
Butler et al12; EMPACT‑MI trial | International | Empagliflozin | 3260 | 63.6 (11) | 812 (24.9) | NS | 2262 (69.4) | 1035 (31.7) | NS | 388 (11.9) |
Control | 3262 | 63.7 (10.8) | 813 (24.9) | NS | 2276 (69.8) | 1046 (32.1) | NS | 459 (14.1) | ||
Dayem et al19; DACAMI trial | Egypt | Dapagliflozin | 50 | 55.2 (13.2) | 42 (84) | 29.96 (4.9) | 32 (64) | NS | 7 (14) | NS |
Control | 50 | 56.7 (11.5) | 41 (82) | 30.13 (4.6) | 29 (58) | NS | 8 (16) | NS | ||
James et al20; DAPA‑MI trial | United Kingdom / Sweden | Dapagliflozin | 2019 | 63 (11.1) | 1631 (80.8) | 28.2 (4.7) | 766 (37.9) | NS | NS | 178 (8.8) |
Control | 1998 | 62.8 (10.6) | 1579 (79) | 28.3 (4.9) | 716 (35.8) | NS | NS | 189 (9.5) | ||
Khani et al21; EMI‑STEMI trial | Iran | Empagliflozin | 50 | 59.2 (10.3) | 39 (78) | 26.8 (9.8) | 24 (48) | NS | NS | NS |
Control | 51 | 61.6 (12.3) | 40 (78.4) | 27 (3.6) | 22 (43) | NS | NS | NS | ||
Shimizu et al22; EMBODY trial | Japan | Empagliflozin | 46 | 63.9 (10.4) | 38 (82.6) | 25.2 (3.7) | 38 (82.6) | 46 (100) | 34 (73.9) | NS |
Control | 50 | 64.6 (11.6) | 39 (78) | 25.2 (4.1) | 39 (78) | 50 (100) | 36 (72) | NS | ||
von Lewinski et al18; EMMY trial | Austria | Empagliflozin | 237 | 57.5 (2) | 195 (82) | 27.8 (0.8) | 92 (39) | 30 (13) | 71 (30) | 14 (5.9) |
Control | 239 | 57.8 (2.2) | 197 (82) | 27.4 (0.9) | 107 (45) | 33 (14) | 64 (27) | 9 (3.8) | ||
Meta‑analysis outcomes
Initiation of SGLT2is was associated with a significant reduction in the risk of hospitalization for HF. Events occurred in 3.2% of the patients in the SGLT2i group and 4.5% in the control group, corresponding to a 29% relative risk reduction (OR = 0.71; 95% CI, 0.58–0.86; P = 0.004; Figure 2).

All‑cause mortality was reported in 6 randomized trials including a total of 11 227 participants. Events occurred in 213 patients (3.8%) in the SGLT2i group and 211 patients (3.7%) in the control group. The pooled analysis yielded the OR of 1.05 (95% CI, 0.77–1.43; P = 0.75; Table 2). Cardiovascular mortality was analyzed in 4 trials, with 162 events in the SGLT2i arm and 156 in the control arm. The pooled effect estimate was not significant (OR = 1.04; 95% CI, 0.83–1.3; P = 0.76; I² = 0%). Regarding MACEs, a total of 833 events (15.9%) occurred in the SGLT2i group, as compared with 870 (16.6%) in the control group. A meta‑analysis of 2 large‑scale trials resulted in the OR of 0.94 (95% CI, 0.85–1.05; P = 0.28; I² = 0%). In terms of nonfatal MI, 45 events occurred in the intervention group and 40 in the control group. The pooled OR was 1.12 (95% CI, 0.73–1.72; P = 0.62; I² = 0%). For stroke, only 2 trials reported data. The event rate was numerically lower in the SGLT2i group (n = 10) than in the control group (n = 17); however, the difference did not reach significance (OR = 0.58; 95% CI, 0.26–1.27; P = 0.17). No significant differences were observed in adverse event rates between the patients receiving SGLT2is and those in the placebo / control groups. Specifically, there was no significant increase in the risk of ketoacidosis, hepatic injury, or acute kidney injury associated with SGLT2i use (Supplementary material, Table S3).
Outcome | Number of studies | Events per participants, n/N (%) | Events | Heterogeneity between trials | P value for differences across groups | |||
SGLT2i group | Control group | MD / OR | 95% CI | P value | I2, % | |||
Abbreviations: HF, heart failure; MD, mean difference; n, number of patients who experienced an event; N, total number of patients; NA, not available; OR, odds ratio; SGLT2, sodium‑glucose cotransporter 2 inhibitor; others, see Table 1 | ||||||||
Hospitalization for HF | 7 | 184/5707 (3.2) | 257/5698 (4.5) | 0.71 | 0.58–0.86 | 0.8 | 0 | 0.004 |
Cardiovascular mortality | 5 | 162/5611 (2.9) | 156/5597 (2.8) | 1.04 | 0.83–1.3 | 0.67 | 0 | 0.76 |
All‑cause mortality | 6 | 213/5662 (3.8) | 211/5650 (3.7) | 1.05 | 0.77–1.43 | 0.26 | 27 | 0.75 |
Nonfatal MI | 3 | 45/2114 (2.1) | 40/2097 (1.9) | 1.12 | 0.73–1.72 | 0.95 | 0 | 0.62 |
Stroke | 2 | 10/2064 (0.5) | 17/2046 (0.8) | 0.58 | 0.26–1.27 | NA | NA | 0.17 |
Ketoacidosis | 2 | 2/3471 (<0.1) | 1/3468 (<0.01) | 2.00 | 0.18–22.04 | NA | NA | 0.57 |
Hepatic injury | 3 | 9/3517 (0.3) | 4/3518 (0.1) | 2.03 | 0.55–7.49 | 0.35 | 5 | 0.29 |
Acute kidney injury | 2 | 27/3471 (0.8) | 43/3468 (1.2) | 0.62 | 0.38–1.01 | NA | NA | 0.06 |
HF | 1 | 0/46 (0) | 1/50 (2) | 0.35 | 0.01–8.93 | NA | NA | 0.53 |
Major adverse cardiovascular events | 2 | 833/5253 (15.9) | 870/5227 (16.6) | 0.94 | 0.85–1.05 | 0.95 | 0 | 0.28 |
Any adverse events | 2 | 891/3280 (27.2) | 888/3279 (2.7) | 0.47 | 0.05–4.31 | 0.1 | 62 | 0.51 |
In agent‑specific subgroup analyses, empagliflozin vs control reduced the incidence of HF hospitalization (pooled OR = 0.68; 95% CI, 0.55–0.84; I² = 0%), whereas dapagliflozin vs control did not (pooled OR = 0.84; 95% CI, 0.51–1.39; I² = 0%). A formal between‑agent interaction could not be robustly assessed due to the small number of dapagliflozin trials (Figure 2). No additional significant changes were seen in the subgroup analysis by agent (Supplementary material, Table S3).
In the subgroup analysis, no significant differences in treatment effects were observed between the patients with and without diabetes across all evaluated end points (Supplementary material, Table S4). In both the T2D and non‑T2D groups, the results were consistent, and did not suggest a meaningful modification of treatment effect by diabetes status (P <0.05).
Risk of bias and certainty of evidence
The RoB 2.0 tool was used to evaluate the risk of bias in each of the 7 included RCTs. Two trials (EMMY [Impact of Empagliflozin on Cardiac Function and Biomarkers of Heart Failure in Patients with Acute Myocardial Infarction18]and EMI‑STEMI [Empagliflozin Effects in Patients with ST‑Elevation Myocardial Infarction Undergoing Primary PCI21]) presented some concerns based on this evaluation, mainly because of their limited prespecification of outcomes and departures from the initial statistical plan. The overall risk of bias for the remaining 5 trials (DAPA‑MI [Dapagliflozin Effects on Cardiometabolic Outcomes in Patients With an Acute Heart Attack20],EMPACT‑MI [Empagliflozin Effects in Patients with ST‑Elevation Myocardial Infarction Undergoing Primary PCI12], EMBODY [Effects of Empagliflozin Versus Placebo on Cardiac Sympathetic Activity in Acute Myocardial Infarction Patients with Type 2 Diabetes Mellitus22],DACAMI [Impact of Dapagliflozin on Cardiac Function Following Anterior Myocardial Infarction in Non‑Diabetic Patients19],and the study by Adel et al17) was deemed to be low. None of the included studies had a high risk of bias rating (Figure 3).

Abbreviations: see Table 2
The reliability of evidence for each outcome was evaluated using the GRADE framework, and is presented in Table 3. The key outcome—hospitalization for HF—was assessed with moderate certainty, yielding a pooled OR of 0.71 (95% CI, 0.58–0.86) from 7 trials including 11 405 patients. The rating was reduced by 1 notch due to a lack of precision, primarily associated with the event rate. The data on cardiovascular mortality and all‑cause mortality were of poor certainty, with no significant differences between the SGLT2i and control groups (OR = 1.04 and OR = 1.05, respectively). The evidence for all‑cause mortality was further lowered due to inconsistency (I² = 27%). Other secondary outcomes—including nonfatal MI, stroke, diabetic ketoacidosis, and hepatic injury—were also rated as of low certainty, primarily due to imprecise effect estimates, low event rates, and the limited number of contributing studies. The evidence for acute kidney injury indicated a potential benefit (OR = 0.62; 95% CI, 0.38–1.01), and was assessed as having moderate certainty, with 1 step of downgrading due to imprecision and borderline significance.
Outcome | Effect estimate, OR (95% CI) | Number of studies (participants) | Certainty of evidence | Comments |
Hospitalization for HF | 0.71 (0.58–0.86) | 7 (11 405) | Moderate | Significant reduction; consistent results; downgraded for imprecision due to event rate |
Cardiovascular mortality | 1.04 (0.83–1.3) | 5 (11 208) | Low | No effect; downgraded for imprecision and low number of events |
All‑cause mortality | 1.05 (0.77–1.43) | 6 (11 312) | Low | No effect; downgraded for imprecision and inconsistency (I² = 27%) |
Nonfatal MI | 1.12 (0.73–1.72) | 3 (4211) | Low | Imprecise estimate with wide 95% CI; few studies |
Stroke | 0.58 (0.26–1.27) | 2 (4110) | Low | Very low event rate and few studies; downgraded for imprecision |
Ketoacidosis | 2 (0.18–22.04) | 2 (6939) | Low | Rare events; wide 95% CI; imprecise |
Hepatic injury | 2.03 (0.55–7.49) | 3 (7035) | Low | Rare outcome; wide 95% CI; downgraded for imprecision |
Acute kidney injury | 0.62 (0.38–1.01) | 2 (6939) | Moderate | Suggestive benefit; borderline significance; downgraded for imprecision |
Discussion
Principal findings
To our best knowledge, this is the first meta‑analysis that is limited to RCTs assessing the early initiation of SGLT2is during the index hospitalization or the early post‑AMI period. We present a current agent‑level synthesis demonstrating that the main short‑term benefit is a 29% relative reduction in the incidence of HF‑related rehospitalization, with neutral effects on mortality and ischemic outcomes. Therefore, 2 large RCTs (EMPACT‑MI12 and DAPA‑MI20) provided the majority of the information for the pooled estimate, with 4 smaller single- or 2‑center trials (n <200 each) contributing a limited amount of weight. On the other hand, rather than indicating a clear lack of effect, the lack of mortality or MACE benefit within 6–18 months most likely resulted from low absolute event rates and the design of the large trials. This was achieved by standardizing end points across the studies and incorporating the most recent large RCTs.
After AMI, patients are at an increased risk for HF and death, particularly if they present with congestion or a decreased LVEF.23-25 Our findings contribute to the growing body of evidence supporting the efficacy of SGLT2is as therapeutic adjuncts in the patients following AMI. In particular, we observed a 29% relative risk reduction in HF‑related rehospitalization, a clinically and organizationally relevant outcome. All estimates reflected short‑term follow‑up (6–18 months) and comparisons against placebo or standard care without SGLT2is. Hospital readmissions impose substantial burdens on health care systems, contribute to psychological stress and physical decline in patients, and are associated with increased risk of hospital‑acquired complications.26,27
Mechanistic rationale
The strategy of early initiation and sustained use of SGLT2is after AMI remains compelling due to their potential mechanistic effects on the disease progression. These include attenuation of adverse ventricular remodeling, delay in the development of chronic HF,28 and interruption of the cardiorenal syndrome cycle,29 characterized by diminished renal perfusion and progressive renal decline. SGLT2is may exert these effects through multiple pathways, including improved hemodynamic stability,30 reduced oxidative stress and inflammation,31 enhanced myocardial energy efficiency via a metabolic shift toward fatty acid oxidation,32 and reduced myocardial sodium and calcium overload. Collectively, these mechanisms may reduce arrhythmic burden,33 improve endothelial function, and enhance coronary microvascular perfusion.34 Moreover, SGLT2is alleviate cardiac fibrosis and promote post‑MI angiogenesis.35 This integrated pathophysiological profile supports the expanded role of SGLT2is in the secondary prevention of HF in post‑AMI patients.
In the early post‑AMI phase, it is biologically possible to reduce the incidence of HF hospitalization selectively, without an impact on mortality or ischemic end points. Although osmotic diuresis and natriuresis, the 2 main short‑term actions of SGLT2is, reduce cardiac filling pressures and relieve interstitial / pulmonary congestion, preventing decompensation and readmissions, they do not directly alter the arrhythmic or recurrent‑ischemic mechanisms that primarily cause early mortality following MI.26,27,30 However, these tissue‑level effects likely take weeks to months to translate into severe outcomes, such as cardiovascular or all‑cause mortality, which is consistent with our follow‑up durations and the neutral findings for MACEs and death.28-35 In addition to decongestion, SGLT2is improve cardiorenal coupling and myocardial energetics (greater metabolic flexibility), attenuate inflammation and oxidative stress, and may limit adverse remodeling. Therefore, while structural and electrophysiological remodeling—possible mediators of mortality reduction—may only manifest with longer exposure and in higher‑risk populations, the early benefit we observed most likely reflects hemodynamic stabilization and prevention of congestion‑driven events.23-25,28-35
Clinical implications and safety
Our meta‑analysis did not demonstrate a significant reduction in all‑cause or cardiovascular mortality with SGLT2is. As the signal for fewer HF readmissions is class‑consistent, but statistically powered primarily by EMPACT‑MI12 and DAPA‑MI20 studies, clinicians should interpret these pooled effects knowing that generalizability is strongest for populations that are similar to those in these trials. These trial‑level findings align with population‑level estimates from Poland indicating that system‑wide implementation of SGLT2is could prevent a large number of HF readmissions and cardiovascular deaths in routine practice.36 This finding raises important questions regarding the routine use of SGLT2is in the early post‑AMI setting, particularly in view of cost‑effectiveness and long‑term safety considerations. While the overall safety profile of SGLT2is is acceptable, the agents are not devoid of adverse effects. These include complications associated with glycosuria, such as genital infections, volume depletion, and, more rarely, diabetic ketoacidosis or Fournier gangrene.37-39
Given these considerations, current evidence does not yet justify the universal initiation of SGLT2is immediately after AMI in all patients. A more nuanced, personalized approach targeting patients at the highest risk for developing HF may yield greater clinical benefit. Until further data are available, guideline‑directed therapies with proven mortality benefits should remain the cornerstone of post‑MI management, while SGLT2is may be selectively considered in patients with high‑risk features.
Context within prior evidence
An essential clinical dilemma emerges regarding the patients without a prior diagnosis of HF who undergo routine echocardiography during the index hospitalization and are found to have reduced LVEF. Should SGLT2is be initiated immediately in these individuals, or is it more appropriate to reassess cardiac function through follow‑up imaging before making therapeutic decisions? Current guidelines11 do not clearly define this scenario, and no current trials have directly compared early vs delayed SGLT2i initiation based on repeated imaging, leaving this an open and clinically relevant question.
The relative treatment effect of SGLT2is on all evaluated cardiovascular outcomes was the same for the patients with and without diabetes, according to our predefined subgroup analysis stratified by diabetes status. Early SGLT2i initiation in the post‑AMI setting may have cardioprotective benefits beyond glycemic control, as evidenced by the observed decrease in HF hospitalization and the neutral effects on mortality and ischemic events that did not significantly differ by diabetes status. The use of SGLT2is in the patients with and without diabetes who are at an increased risk of HF following AMI is supported by the increasing amount of evidence showing that hemodynamic, renal, and myocardial effects are primarily independent of baseline glycemic status.
Observational data in post‑MI populations suggest that the patients who exhibit LVEF recovery within the first month postinfarction have significantly better outcomes than those with persistently reduced function.40,41 The prognostic value of early LVEF recovery has been confirmed in cohorts with long‑term follow‑up exceeding 10 years.42 Considering the above, delaying the decision to initiate SGLT2is until follow‑up imaging may help refine patient selection.
In the EMPACT‑MI trial,12 it has been hypothesized that a proportion of patients with reduced LVEF or congestion at the time of randomization may have had myocardial stunning rather than irreversible dysfunction. This is particularly plausible in the subgroup of patients with STEMI, who constituted approximately 75% of the trial population, and nearly 90% of whom underwent early revascularization. In these cases, the potential for spontaneous recovery of ventricular function might have blunted the therapeutic signal of SGLT2is in lower‑risk individuals.43-45
Empagliflozin decreased HF hospitalization rate when compared with control in subgroup analyses by agent,12,17,18,21,22 while dapagliflozin did not reach significance when compared with control19,20; due to the limited number of trials and a lack of direct head‑to‑head comparisons, these findings should be interpreted with caution. Interestingly, a recent multicenter retrospective cohort study in patients with HF, including those with ischemic heart disease but not in the acute post‑MI phase, also suggested a modest advantage of empagliflozin over dapagliflozin in reducing mortality and hospitalization risk.46 Despite the availability of 4 Federal Drug Administration–approved SGLT2is (canagliflozin, dapagliflozin, empagliflozin, and ertugliflozin), comparative evidence of the agents in the post‑AMI setting is lacking. The observed class effect may not apply uniformly, and further head‑to‑head trials are needed to delineate individual drug profiles.
Limitations
This meta‑analysis has several limitations. Most of the included studies had relatively short follow‑up durations, ranging from 6 months to approximately 18 months, which may have not adequately reflected the long‑term impact of SGLT2is on cardiovascular outcomes. Many of the trials were conducted in 1 or 2 centers and enrolled a predominantly homogeneous population, which may limit generalizability of the findings. Also, 4 of the 7 included studies recruited fewer than 200 participants, reducing the statistical power to detect significant differences in clinical end points. The definition of end points varied considerably. While 2 trials (EMPACT‑MI12 and the DAPA‑MI20 substudy) investigated hard clinical outcomes, such as cardiovascular death and HF hospitalization, the remaining studies primarily relied on surrogate markers, including NT‑proBNP levels and echocardiographic parameters. Although informative, these surrogate end points may not fully capture patient‑centered clinical benefit.
There was also notable heterogeneity in the choice of SGLT2is and the timing of treatment initiation, which ranged from within the first 24 hours post‑MI to up to 2 weeks after hospital discharge. Moreover, safety data, including adverse events, such as genital infections or ketoacidosis, were not consistently reported, preventing a reliable pooled safety assessment. None of the studies directly compared different SGLT2is, which limits conclusions about class effects or agent‑specific benefits. Our review’s mechanistic interpretations inevitably led to the development of hypotheses. The agent‑level subgroup analysis was underpowered due to low event rates and no head‑to‑head comparisons, and none of the included trials were built to measure mechanistic surrogates (such as serial congestion indices or remodeling markers) concurrently with clinical outcomes across both arms. Therefore, rather than being conclusive drug‑specific effects, the observed differences between empagliflozin and dapagliflozin should be considered exploratory, primarily due to intertrial heterogeneity. Finally, as this meta‑analysis was conducted using study‑level data, it was impossible to perform detailed subgroup analyses or adjust for potential confounding variables. As a result, the ability to tailor interpretations to specific clinical scenarios or patient subpopulations remains limited.
Future directions
In order to identify pathways to benefit, future trials should include longer follow‑up, optimize for patients at the highest risk of congestion and adverse remodeling, and integrate mechanistic evaluations (such as imaging‑based remodeling markers, biomarkers, and serial congestion indices). Practice would be directly informed by head‑to‑head comparisons of SGLT2is and approaches that use repeat imaging to randomly assign early vs delayed initiation.
Conclusions
Early SGLT2i initiation compared with placebo / standard care decreased subsequent hospitalization for HF without increasing adverse events in RCTs with short‑term follow‑up (6–18 months). During this period, there were no discernible impacts on MACEs, recurrent MI, stroke, or cardiovascular or all‑cause mortality. Larger and longer‑term trials are required to ascertain the SGLT2is effects on mortality and ischemic outcomes, but these results support the selective use of SGLT2is in the post‑AMI patients at an elevated HF risk.
- Roth GA, Mensah GA, Johnson CO, et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990‑2019: update from the GBD 2019 Study. J Am Coll Cardiol. 2020; 76: 2982‑3021. | Crossref
- Cahill TJ, Kharbanda RJ. Heart failure after myocardial infarction in the era of primary percutaneous coronary intervention: mechanisms, incidence and identification of patients at risk. World J Cardiol. 2017; 9: 407‑415. | Crossref
- Hung J, Teng TH, Finn J, et al. Trends from 1996 to 2007 in incidence and mortality outcomes of heart failure after acute myocardial infarction: a population‐based study of 20,812 patients with first acute myocardial infarction in Western Australia. J Am Heart Assoc. 2013; 2: e000172. | Crossref
- Sulo G, Igland J, Vollset SE, et al. Heart failure complicating acute myocardial infarction; burden and timing of occurrence: a nation‐wide analysis including 86 771 patients from the cardiovascular disease in Norway (CVDNOR) project. J Am Heart Assoc 2016; 5: e002667. | Crossref
- Jenča D, Melenovský V, Stehlik J, et al. Heart failure after myocardial infarction: incidence and predictors. ESC Heart Fail. 2021; 8: 222‑237. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION