Positron emission tomography / computed tomography–guided nodal triage in a lymphoma survivor undergoing en-bloc robot-assisted nephroureterectomy and cystectomy for distal ureteral carcinoma

 CC BY 4.0
CC BY 4.0
Positron emission tomography / computed tomography–guided nodal triage in a lymphoma survivor undergoing en-bloc robot-assisted nephroureterectomy and cystectomy for distal ureteral carcinoma
A 73‑year‑old man with follicular lymphoma completed 8 cycles of rituximab‑based immunochemotherapy in March 2024. Baseline computed tomography (CT) in September 2023 demonstrated bulky retroperitoneal and iliac lymph node (LN) conglomerates. On response assessment fluorine‑18 fluorodeoxyglucose (18F‑FDG) positron emission tomography (PET)/CT in July 2024, the LNs showed no abnormal uptake, consistent with complete metabolic response according to the Lugano / Deauville scoring system.1
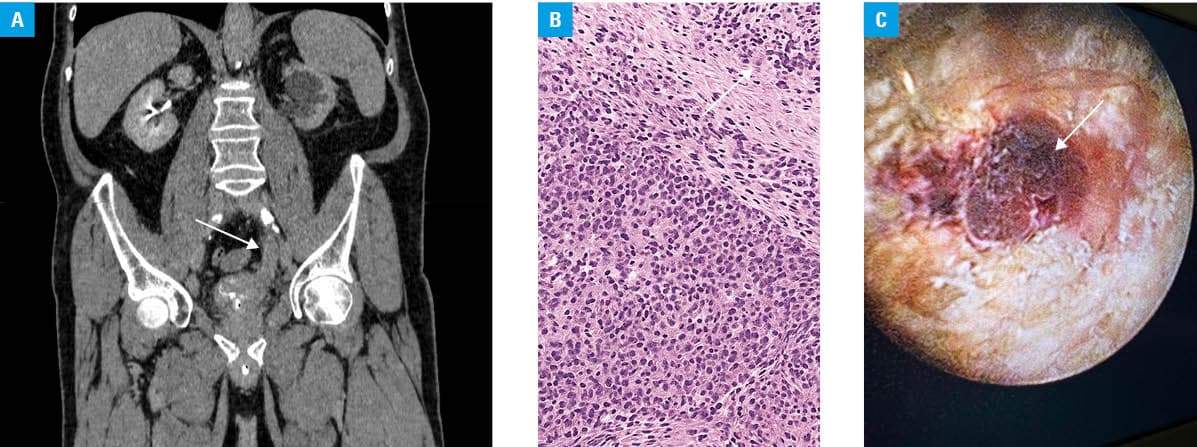
In January 2025, contrast enhanced CT performed for gross hematuria identified a 30‑mm mass in the distal left ureter, extending into the bladder with ipsilateral ureterohydronephrosis (Figure 1A), as well as pelvic and para‑aortic nodes measuring up to 10 mm. PET/CT and CT, although performed within a short time frame, served different purposes: PET/CT (negative) assessed lymphoma activity, whereas CT demonstrated mechanical obstruction from a distal ureteral lesion—often PET‑inconspicuous in the pelvis due to physiological urinary 18F‑FDG excretion. Transurethral resection in January 2025 targeted a left ureteric orifice lesion invading the bladder wall. Histopathology demonstrated high‑grade, nonpapillary, infiltrating urothelial carcinoma (UC) invading the muscularis propria (Figure 1B), with angioinvasion (micro‑pT2, sampling, understaged). Left nephrostomy had been placed for decompression.
Pre‑existing lymphoma complicated nodal interpretation. Because urinary 18F‑FDG excretion can obscure pelvic disease, another negative PET/CT of March 2025 was interpreted cautiously and integrated with ureteroscopic, histological, and cross‑sectional findings from the same time. In upper‑tract UC (UTUC), 18F‑FDG‑PET/CT shows only moderate accuracy for nodal metastases (sensitivity, 82%; specificity, 84%). Major guidelines concur that PET/CT is not a standard tool for UTUC staging: the European Association of Urology positions PET/CT as an adjunct, mainly when CT is contraindicated, while the American Urological Association reserves it for problem‑solving when conventional staging is equivocal.2-4 Thus, although negative PET/CT could not exclude micrometastatic UC, in this clinical context it favored reactive / post‑treatment lymphadenopathy and supported proceeding to curative surgery with definitive pathologic staging.
In April 2025, in a surgically fit (Eastern Cooperative Oncology Group score, 0) patient with endoscopic evidence of a distal ureteral tumor (Figure 1C) infiltrating the prostatic urethra, muscle‑invasive high‑grade histology, and obstructive uropathy, bladder‑sparing strategies (endoscopic ablation, segmental ureterectomy, or partial cystectomy) were considered oncologically inferior. Estimated glomerular filtration rate (eGFR) was 67 ml/min/1.73 m², urine cytology / bladder mapping was omitted, and the January–April interval reflected staged workup and scheduling. One‑stage, totally intracorporeal, robot‑assisted en‑bloc left nephroureterectomy with radical cystectomy was performed, with an uneventful postoperative course. Final pathology confirmed high‑grade UC of the distal left ureter with transmural invasion and direct extension across the bladder wall into the perivesical fat, with negative surgical margins (pT4aN0Mx). At 30 days, no complications were noted, with eGFR of 49 ml/min/1.73 m². PET/CT surveillance in July 2025 showed no evidence of disease, with ongoing protocolized follow‑up.
In lymphoma survivors with suspected UTUC, PET/CT—limited by urinary tracer excretion—should be integrated with endoscopy, histology, and CT to triage lymphadenopathy and avoid misstaging. In this case, PET/CT served a problem‑solving purpose, complementing conventional imaging rather than being employed as part of the routine staging algorithm.2,3 For organ‑confined disease with direct bladder extension, single‑session, totally intracorporeal robot‑assisted nephroureterectomy with cystectomy is feasible and streamlines definitive care.4,5
- Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non‑Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014; 32: 3059‑3067. | Crossref
- Lakhani A, Khan SR, Bharwani N, et al. FDG PET/CT pitfalls in gynecologic and genitourinary oncologic imaging. Radiographics. 2017; 37: 577‑594. | Crossref
- Chandra R, Subesinghe M, Bradley KM. PET/CT in bladder cancer: an update. Semin Nucl Med. 2021; 52: 475‑485. | Crossref
- Masson‑Lecomte A, Gontero P, Birtle A, et al. European Association of Urology guidelines on upper urinary tract urothelial carcinoma 2025. Arnhem, The Netherlands: EAU Guidelines Office; 2025. | Crossref
- Liu Y, Zhang H, Wen Z, et al. Simultaneous radical cystectomy and nephroureterectomy in the treatment of panurothelial carcinoma: a systematic review and single‑arm meta‑analysis. Front Oncol. 2023; 13: 1233125. | Crossref
ARTICLE INFORMATION