Risk of hepatocellular carcinoma recurrence in liver transplant recipients following treatment of hepatitis C with direct-acting antivirals
Key words: direct-acting antivirals, hepatitis C virus, hepatocellular carcinoma, liver transplant

 CC BY 4.0
CC BY 4.0
Risk of hepatocellular carcinoma recurrence in liver transplant recipients following treatment of hepatitis C with direct-acting antivirals
Introduction: Data on the risk of hepatocellular carcinoma (HCC) recurrence in a transplanted liver following direct‑acting antiviral (DAA) therapy for hepatitis C virus (HCV) infection are sparse and inconsistent.
Objectives: This study aimed to evaluate the safety and efficacy of DAA treatment in patients with a history of orthotopic liver transplant (OLTx) performed due to HCV‑related cancer, and to assess the risk of HCC recurrence.
Patients and methods: This real‑world retrospective study included all consecutive patients with chronic hepatitis C who underwent LTx for HCV‑related HCC before DAA therapy. Treatment efficacy (measured by sustained virologic response) and patient outcomes (adverse events, mortality, HCC recurrence) were assessed during treatment, 12 weeks after treatment completion, and in long‑term follow‑up.
Results: The analyzed population included 58 patients at a median (interquartile range [IQR]) age of 59 (53–63) years; predominantly men (70.7%). The majority of patients had comorbidities (83%) and were infected with the genotype 1b of HCV (86.2%). Less than half of the population was treatment‑experienced. The median (IQR) time from OLTx to DAA initiation was 19.5 (9.8–36) months. Twelve patients had cirrhosis at the start of DAA therapy, including 4 with decompensated cirrhosis. Ttreatment effectiveness was 98.2%, with no differences according to the stage of fibrosis, time since OLTx, and type of DAA regimen used. During a median (IQR) long‑term follow‑up of 8 (6–9) years, 3 patients (5.4%) developed recurrent HCC in the transplanted liver; one during DAA therapy, one 12 weeks after treatment initiation, and one 2 years after the DAA therapy completion. All these patients died from liver cancer dissemination.
Conclusions: DAA therapy in patients who received antiviral treatment after OLTx performed due to HCV‑related HCC was highly effective, and the long‑term HCC recurrence rate was 5.4%, which is lower than expected based on the natural history of the disease.
What's new?
Our multicenter study documented a good safety profile and very high effectiveness (>98%) of direct‑acting antiviral (DAA) therapy in patients infected with hepatitis C virus (HCV) who previously underwent liver transplant due to hepatocellular carcinoma. In long‑term observation, the tumor recurrence rate was only 5.4%, which is much lower than the expected historical value of 8%–20%. Thus, we provided evidence to support DAA therapy in patients with a history of liver transplant due to HCV‑related cancer, without concerns about worsening prognosis. This study is the third largest in the world in terms of the population size. Its novelty lies in the inclusion of patients treated with new pangenotypic options and the longest follow‑up period, averaging 8 years.
Introduction
A decade ago, the introduction of interferon (IFN)-free direct‑acting antiviral (DAA) drugs revolutionized the treatment of chronic hepatitis C (CHC).1 This type of therapy provides individuals with hepatitis C virus (HCV) infection with a highly effective and short‑duration option for eradicating the virus. It reduces the risk of the most serious complications of the disease, namely, cirrhosis, liver failure, and hepatocellular carcinoma (HCC).2 These severe consequences of CHC result in approximately 240 000 deaths each year among the estimated 50 million people infected worldwide.3
In HCV infection, HCC develops almost exclusively in patients with cirrhosis. During the era of IFN‑based regimens, this patient population had severely limited access to treatment due to contraindications, a high risk of side effects, and a lack of significant survival benefit.4,5 Currently, orthotopic liver transplant (OLTx) serves as a life‑saving option for the patients with HCC who meet prespecified tumor‑related criteria.6 However, HCV infection recurrence in the transplanted liver in the individuals who had active viral infection at the time of surgery is common. It may lead to accelerated progression of fibrosis and graft failure, and the risk of post‑transplant HCC recurrence in such patients can be as high as 20%.7,8
In the era of DAAs, abundant evidence from both clinical trials and real‑world experience (RWE) studies supports the beneficial impact of effective antiviral therapy on reducing disease progression and improving survival in patients with end‑stage liver disease, including those with liver cirrhosis and HCC.9 However, such patients still represent a special population requiring increased attention and an individualized approach to the choice of optimal management, with close monitoring not only during but also after therapy.10-12 Choosing not only the proper treatment approach but also the most appropriate timing and sequence of actions is crucial for patients placed on the OLTx waiting list for due to end‑stage liver disease.13
Patients diagnosed with HCV‑related HCC who are candidates for LTx should be treated for HCV infection before or after OLTx, in close collaboration between hepatologists and transplantologists, taking into account planned cancer therapies, the likelihood of treatment response, and access to transplantation.10,11
The importance of evaluating the risk of HCC recurrence stems from doubts raised by reports from the early DAA era describing unexpectedly high rates of HCC recurrence in patients following cancer cure after DAA treatment.14-16 Moreover, while several observational studies documented a lack of association between DAA therapy and an increased risk of de novo / recurrent HCC, there are concerns that patients with liver cancer may be excluded from antiviral treatment because of these conflicting findings.17,18 Notably, of the analyses published to date that included patients after different types of radical therapy for HCC, only a few analyzed individuals with a history of OLTx, as did this study, including 2 with larger populations.19,20
In our retrospective, multicenter RWE analysis, we focused on patients who first underwent LTx for HCC, and then received DAA therapy. The study aimed to evaluate the effectiveness and safety of DAA regimens in these patients, as well as to assess long‑term survival and the risk of HCC recurrence to provide evidence supporting appropriate management in this population.
Patients and methods
The study included all consecutive patients with chronic HCV infection treated with DAA drugs at Polish hepatology centers who underwent LTx for HCV‑related HCC before starting antiviral therapy. The patients received medications for CHC under the reimbursed therapeutic program of the National Health Fund (NHF). The choice of the therapeutic regimen was made by the treating physicians based on product characteristics, requirements of the drug program, and recommendations of international scientific societies and the Polish HCV Expert Group.10,21
Patient data were collected retrospectively from medical records and entered into an electronic web‑based platform managed by Tiba (Wrocław, Poland). Data captured at baseline included demographic and clinical parameters: sex, age, comorbidities, hepatitis B virus (HBV) and HIV coinfections, and comedications. Laboratory parameters analyzed included complete blood count, alanine aminotransferase (ALT) activity, creatinine concentration, and parameters defining liver function, namely, bilirubin and albumin levels and international normalized ratio (INR). Data characterizing HCV infection included virologic test results, such as genotype and viral load of HCV RNA measured by real‑time polymerase chain reaction with a lower detection limit of 10 IU/ml (56 copies/ml).
The severity of liver disease in terms of the presence of cirrhosis was evaluated noninvasively on transient elastography with FibroScan or shear wave elastography with Aixplorer (SuperSonic Imagine, Aix‑en‑Provence, France). The elastographic findings, comprising liver stiffness expressed in kilopascals (kPa), were presented in correlating degrees of fibrosis (F) on the Metavir scale, in accordance with the European Association for the Study of the Liver (EASL) recommendations.10 The F4 score was the basis for a diagnosis of cirrhosis.22 The patients with cirrhosis were assessed with the Child–Pugh (CP) scale. We collected data on decompensated liver function, reflected by ascites or encephalopathy, both in the past and at the start of DAA therapy. We also report data on the time elapsed between OLTx and DAA treatment initiation, and the type of immunosuppression used.
Information on antiviral therapy included a history of previous treatment, the type of DAA regimen currently used, its effectiveness, and safety. The patients received either genotype‑specific or pangenotypic DAA options. The effectiveness of the treatment was measured by the sustained virologic response (SVR), defined as undetectable HCV RNA at 12 weeks after the end of the therapy. The patients with detectable viremia were considered virologic nonresponders, whereas those who did not have their HCV RNA assessed at this time point were considered lost to follow‑up (LTFU).
Safety data were collected throughout the treatment course and a 12‑week follow‑up period. We gathered data on treatment modification or discontinuation, occurrence of adverse events (AEs), including serious AEs (SAEs) and AEs of particular interest, such as ascites, encephalopathy, and gastrointestinal bleeding, and deaths. At the time of this analysis, in June 2025, retrospective data on patient survival and HCC recurrence were obtained.
Statistical analysis
Qualitative variables were analyzed by calculating their frequency and percentage distributions. Comparisons between categorical variables were made using the χ2 test or Fisher exact test, as appropriate. Since the quantitative data did not follow a normal distribution, they were described using medians and interquartile ranges (IQRs). To assess normality of the data distribution, the Shapiro–Wilk test was used. Survival analysis was performed using the Kaplan–Meier method to estimate the cumulative probability of overall survival, with survival rates at specific time points along with their 95% CIs. Differences between survival curves were assessed using the log‑rank test (Mantel–Cox). Correlations between continuous or ordinal variables were evaluated using the Spearman rank correlation coefficient. A P value below 0.05 was considered significant. Statistical calculations were performed using Statistica, version 13 (StatSoft, Tulsa, Oklahoma, United States) and GraphPad Prism, version 5.1 packages (GraphPad Software, Inc., La Jolla, California, United States).
Ethics
This study was approved by the Bioethics Committee of Jan Kochanowski University in Kielce (57/2024). All participants gave their written informed consent to participate in the therapeutic program, following the guidelines of the NHF.
Results
Study population
The study population included 58 patients selected from a national EpiTer‑2 database of 20 586 adults treated with DAA between July 1, 2015 and December 31, 2024, at 22 Polish hepatology centers (Figure 1).
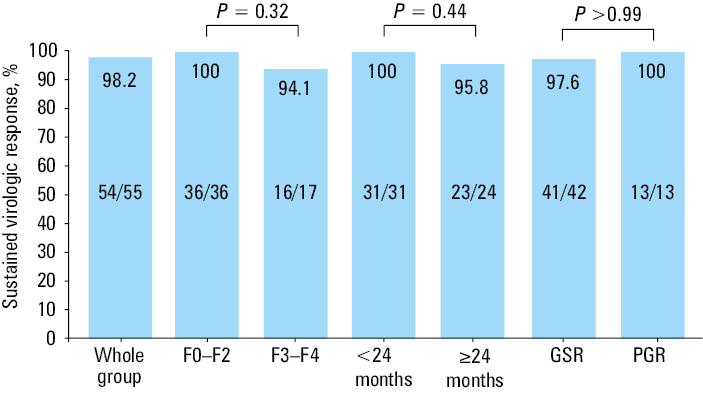
![Effectiveness of direct-acting antiviral (DAA) therapy in a per-protocol analysis according to the stage of the disease before DAA therapy initiation (fibrosis [F] grade 0–2 vs 3–4), the time elapsed from transplant to treatment, and the type of regimen (genotype-specific [GSR] vs pangenotypic [PGR])](/paim/_next/image/?url=https%3A%2F%2Fpamw.pl%2Fsites%2Fdefault%2Ffiles%2Fjson_zip_files%2Funcompressed%2F17131%2FIMAGES%2FKP_WEB__FIG_01.png&w=3840&q=75)
Abbreviations: DAA, direct‑acting antiviral; HCC, hepatocellular carcinoma; OLTx, orthotopic liver transplant
The analyzed population was predominantly male (70.7%), and mostly comprised individuals aged 50 years and older (84.5%; Table 1). A total of 49 patients (83%) had comorbidities, the most common of which was diabetes, followed by arterial hypertension and chronic kidney disease. Apart from immunosuppressive therapy after OLTx, 44.6% of the patients were on other medications due to coexisting diseases. No patient had HBV or HIV coinfection. Baseline median values of liver function parameters (albumin, bilirubin, INR) were within normal limits, while ALT activity was elevated (Table 1).
Parameter | Value | |
Data are presented as number (percentage) or median (interquartile range).
SI conversion factors: to convert ALT to µkat/l, multiply by 0.0167; albumin to g/l, by 10; bilirubin to µmol/l, by 17.1; hemoglobin to g/l, by 10; creatinine to µmol/l, by 88.4; HCV RNA to copies/ml, by 5.6
Abbreviations: ALT, alanine aminotransferase; BMI, body mass index; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HCV, hepatitis C virus; INR, international normalized ratio; others, see Figure 1 | ||
Age, y | 59 (53–63) | |
Age ≥50 y | 49 (84.5) | |
Sex | Women | 17 (29.3) |
Men | 41 (70.7) | |
BMI, kg/m2 | 26.3 (24.2–28.7) | |
Comorbidities | Any comorbidity | 49 (83) |
Diabetes | 32 (55.2) | |
Obesity | 10 (17.2) | |
Arterial hypertension | 31 (53.4) | |
Non‑HCC tumors | 1 (1.7) | |
Renal disease | 18 (31) | |
Concomitant medications (apart from immunosuppressants) | 37 (44.6) | |
HBV coinfection, HBsAg+ | 0 | |
HIV coinfection | 0 | |
ALT, IU/l | 80 (43–154) | |
Albumin, g/dl | 4.2 (3.8–4.5) | |
Bilirubin, mg/dl | 1 (0.8–1.3) | |
Hemoglobin, g/dl | 13.7 (12.6–15.2) | |
Platelets, × 103/µl | 137.5 (110–168) | |
Creatinine, mg/dl | 1 (0.8–1.2) | |
INR | 1 (1–1.1) | |
HCV RNA, × 106 IU/ml | 1.4 (0.8–2.6) | |
A majority of the patients were infected with the genotype (GT) 1b (86.2%), and less than half of the population (46.6%) was treatment‑experienced (Table 2). During the most recent therapy, 75.9% of the patients received genotype‑specific DAA options, most commonly the combinations of sofosbuvir / ledipasvir with or without ribavirin and ombitasvir / paritaprevir / ritonavir with or without dasabuvir and / or ribavirin. Twelve patients (20.7%) were diagnosed with liver cirrhosis at the start of DAA therapy, 4 of whom showed signs of decompensation in the form of ascites and / or hepatic encephalopathy (Table 2). Three patients with cirrhosis were classified as grade B, and none met the criteria for grade C on the CP scale. In the entire group analyzed, 11 patients had a history of decompensated liver function. The median (IQR) time from OLTx to initiation of antiviral treatment was 19.5 (9.8–36) months (Supplementary material, Figure S1). We found no significant correlation between fibrosis and the time from OLTx to DAA initiation (Spearman r = 0.11; P = 0.42), although a slight upward trend was observed.
Parameter | Value | |
Data are presented as number (percentage).
Abbreviations: DCV, daclatasvir; DSV, dasabuvir; F, fibrosis; IFN, interferon; LDV, ledipasvir; OBV, ombitasvir; PTV, paritaprevir; r, ritonavir; RBV, ribavirin; SMV, simeprevir; SOF, sofosbuvir; VEL, velpatasvir; VOX, voxilaprevir; others, see Figure 1 | ||
HCV genotype | ||
1 | 1 (1.7) | |
1b | 50 (86.2) | |
3 | 6 (10.4) | |
Not determined | 1 (1.7) | |
History of antiviral therapy | ||
Treatment‑naive | 31 (53.4) | |
Treatment‑experienced, nonresponder to IFN‑based regimens | 24 (41.4) | |
Treatment‑experienced, nonresponder to DAA regimens | 3 (5.2) | |
Current treatment regimen | ||
Genotype‑specific treatment regimens | Overall | 44 (75.9) |
SOF/LDV±RBV | 22 (37.9) | |
OBV/PTV/r±DSV±RBV | 20 (34.5) | |
SOF+SMV±RBV | 2 (3.4) | |
Pangenotypic regimens | Overall | 14 (24.1) |
SOF+RBV | 3 (5.2) | |
SOF+DCV±RBV | 3 (5.2) | |
SOF/VEL±RBV | 6 (10.3) | |
SOF/VEL/VOX | 2 (3.5) | |
History of hepatic decompensation | 11 (19) | |
Liver fibrosis at the start of DAA therapy | ||
F0 | 3 (5.2) | |
F1 | 18 (31) | |
F2 | 18 (31) | |
F3 | 5 (8.6) | |
F4 | 12 (20.7) | |
No data | 2 (3.5) | |
Liver decompensation at baseline | 4 (6.9) | |
Moderate ascites | 3 (5.2) | |
Encephalopathy | 2 (3.4) | |
Child–Pugh score, in relation to F4 | ||
B | 3 (25) | |
C | 0 | |
Three patients (5.2%) experienced acute transplant rejection prior to starting DAA therapy, which was successfully managed in 2 cases by increasing the dose of the immunosuppressive drug, whereas 1 patient required glucocorticosteroids. Immunosuppressive therapy included tacrolimus (n = 51), cyclosporine (n = 7), mycophenolate mofetil (n = 43), everolimus (n = 3), and glucocorticosteroids (n = 38) in various configurations. A majority of the patients were on immunosuppressive therapy with 3 drugs (n = 33; 56.9%), followed by 2‑drug regimen used in 18 individuals (31%), whereas immunosuppressive therapy with a single drug was administered in 7 patients (12.1%). The attending physician selected a DAA regimen after analyzing potential drug‑drug interactions using the Liverpool Hep Drug Interaction Checker tool, as recommended by the EASL. Immunosuppressive drug levels were regularly monitored and maintained within therapeutic values during and after treatment, in collaboration with the transplant center.
Treatment safety
A majority of the patients completed the treatment course as planned (Table 3). About 50% experienced at least 1 AE, predominantly weakness / fatigue. Most AEs were mild, while 2 patients experienced SAEs (HCC dissemination, urosepsis). Therapy was discontinued in 1 patient after 12 weeks of a planned 24‑week DAA regimen because of HCC dissemination. Three patients experienced AEs of special interest in the form of ascites, but 2 of them had ascites at baseline. Two patients died during the study period: one after treatment discontinuation due to HCC dissemination, and the other during treatment from late vascular complications following OLTx.
Parameter | Value | |
Data are presented as number (percentage) of patients.
a Two patients had ascites at baseline.
Abbreviations: AE, adverse event; others, see Table 2 | ||
Treatment course | According to schedule | 54 (93.1) |
RBV dose modification | 2 (3.45) | |
Therapy discontinuation | 2 (3.45) | |
Serious AEs | 2 (3.4) | |
AEs leading to discontinuation of treatment | 1 (1.7) | |
AEs | Any AE | 29 (50) |
Weakness / fatigue | 16 (27.6) | |
Anemia | 11 (19) | |
Headache | 5 (8.6) | |
Itchy skin | 1 (1.7) | |
Ascitesa | 3 (5.2) | |
Hepatic encephalopathy | 0 | |
Gastrointestinal bleeding | 0 | |
Death | 2 (3.4) | |
Treatment effectiveness
The 2 patients who died during the treatment and follow‑up period did not have their HCV RNA assessed at 12 weeks post‑therapy. Another patient missed the scheduled 12‑week follow‑up visit, bringing the total number of LTFU patients to 3. Overall, the SVR rate in the analyzed population, calculated according to intent‑to‑treat analysis, was 93.1% (54/58), and 98.2% (54/55) after excluding the LTFU cases (Figure 2).
The virologic nonresponder was a 59‑year‑old woman infected with GT1b and diagnosed with cirrhosis at the start of DAA therapy. She underwent a transplant 10 years before her 12‑week treatment for HCC (sofosbuvir + simeprevir; 2016), and previously received pegylated IFN (PegIFN) and ribavirin.
Survival and incidence of hepatocellular carcinoma recurrence in patients with a history of liver transplant for hepatocellular carcinoma
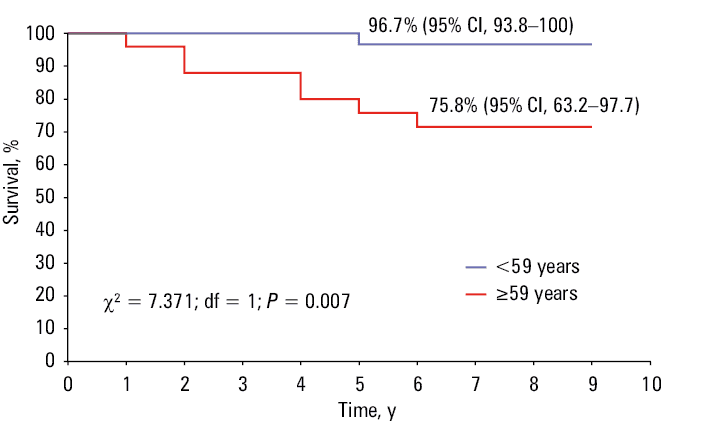
Long‑term data were available for all 58 patients who underwent OLTx prior to DAA therapy for HCC. Interestingly, the data were also available for the patient who did not have an SVR evaluation performed due to missing a visit 12 weeks after treatment; at the long‑term follow‑up, HCV RNA was undetectable in this patient. After DAA therapy, the patients were followed for a median (IQR) of 8 (6–9) years (Supplementary material, Figure S2). The Kaplan–Meier analysis estimated the 6‑year overall survival at 85% (95% CI, 72.2%–92.2%) in the whole population. Survival plateaued at 96.7% (95% CI, 93.8%–100%) from year 5 onward in the patients younger than 59 years (median age of the study population), as compared with 75.8% (95% CI, 63.2%–97.7%) from year 6 onward in the patients aged 59 years and older (log‑rank test: χ² = 7.371; df = 1; P = 0.007; Figure 3).
In addition to the abovementioned 2 patients who died during treatment or within the 12‑week follow‑up period, 8 deaths occurred during long‑term follow‑up. These were due to lung cancer (n = 1), prostate cancer (n = 1), rectal cancer (n = 1), stroke (n = 1), cardiovascular disease (n = 2), and HCC dissemination (n = 2). Two patients required liver retransplant due to the development of cirrhosis in the transplanted organ, and both were alive at the end of the long‑term follow‑up. Three individuals (5.4%) developed HCC recurrence in the transplanted liver, 1 during therapy, 1 at 12 weeks post‑treatment, and 1 within 2 years of DAA therapy initiation (Table 4). All of them were diagnosed with diabetes, and 2 also had arterial hypertension. All patients with recurrent liver cancer died due to HCC dissemination. We compared the patients who experienced either HCC recurrence or death with those who had neither event (Table 5). Significant differences were observed only for age, serum creatinine level, and CP class B. Due to the limited number of events, multivariate analysis was not performed.
Characteristics | Patient | ||
Woman, 60 y | Man, 63 y | Man, 61 y | |
Comorbidities | Diabetes | Diabetes, arterial hypertension | Diabetes, arterial hypertension |
HCV genotype | 1B | 1B | 1B |
BMI, kg/m2 | 25.07 | 20.98 | 26.83 |
Time between OLTx and DAA treatment, mo | 6 | 8 | 39 |
Immunosuppressive therapy | Tacrolimus + mycophenolate mofetil + glucocorticosteroid | Tacrolimus + mycophenolate mofetil + glucocorticosteroid | Tacrolimus + glucocorticosteroid |
Fibrosis grade at baseline of DAA therapy | 2 | 2 | 1 |
DAA regimen (year of treatment) | SOF/VEL, 12 weeks (2019) | OBV/PTV/r+DSV+RBV, 24 weeks (2017) | SOF/LDV+RBV, 12 weeks (2016) |
Treatment course | As planned | Discontinued after 12 weeks | As planned |
SVR | Achieved | Not assessed due to death | Achieved |
Time of HCC recurrence | During the 12 weeks of FU after DAA completion (2020) | During DAA therapy (2017) | Within 2 years of DAA therapy (2018) |
Outcome | Death due to HCC dissemination and COVID‑19 (2020) | Death due to HCC dissemination (2017) | Death due to HCC dissemination (2018) |
Parameter | No recurrence or death (n = 48) | Recurrence and / or death (n = 10) | P value | |
Data are presented as number (percentage) or median (interquartile range).
SI conversion factors: see Table 1
| ||||
Sex | Women | 14 (29.2) | 3 (30) | >0.99 |
Men | 34 (70.8) | 7 (70) | ||
Age, y | 58 (52–61) | 62.5 (60–63) | 0.04 | |
Age ≥50 y | 40 (83.3) | 9 (90) | >0.99 | |
BMI, kg/m2 | 26.3 (24.3–28.9) | 25.8 (23.5–28.7) | 0.41 | |
ALT, IU/l | 72 (43.5–146.5) | 83.5 (36–190) | 0.89 | |
Albumin, g/dl | 4.2 (3.8–4.5) | 4.1 (3.6–4.4) | 0.39 | |
Bilirubin, mg/dl | 1 (0.8–1.3) | 1 (0.8–1.2) | 0.97 | |
Hemoglobin, g/dl | 13.7 (12.8–15.3) | 13.2 (12–14.2) | 0.18 | |
Platelets, × 103/µl | 142 (106.5–172.5) | 130.5 (120–165) | 0.94 | |
Creatinine, mg/dl | 0.9 (0.8–1.1) | 1.1 (1.1–1.4) | 0.02 | |
INR | 1 (1–1.1) | 1 (1–1.1) | 0.73 | |
HCV RNA, × 106 IU/ml | 1.4 (0.5–2.6) | 1.5 (1.1–2.7) | 0.63 | |
DAA therapy with genotype‑specific regimen | 37 (77.1) | 7 (70) | 0.69 | |
DAA therapy with pangenotypic regimen | 11 (22.9) | 3 (30) | 0.69 | |
Comorbidities | Any | 39 (81.3) | 9 (90) | 0.67 |
Hypertension | 24 (50) | 7 (70) | 0.31 | |
Diabetes mellitus | 25 (52.1) | 7 (70) | 0.49 | |
Obesity | 9 (18.8) | 1 (10) | 0.67 | |
Renal disease | 16 (33.3) | 2 (20) | 0.71 | |
Non‑HCC tumors | 1 (2.1) | 0 | >0.99 | |
Genotype | Genotype 1b/non‑1b | 41 (87.2) | 9 (90) | >0.99 |
Genotype non‑1b | 6 (12.8) | 1 (10) | >0.99 | |
DAA treatment history | Treatment‑naive | 26 (54.2) | 5 (50) | >0.99 |
Treatment‑experienced | 22 (45.8) | 5 (50) | ||
History of ascites | 7 (14.6) | 2 (20) | 0.65 | |
History of encephalopathy | 1 (2.1) | 1 (10) | 0.32 | |
Encephalopathy and / or ascites at DAA baseline | 2 (4.2) | 2 (20) | 0.13 | |
Encephalopathy at DAA baseline | 1 (2.1) | 1 (10) | 0.32 | |
Ascites at DAA baseline | 1 (2.1) | 2 (20) | 0.07 | |
Advancement of the disease (F0–F2) | 31 (64.6) | 8 (80) | >0.99 | |
Advancement of the disease (F3–F4) | 15 (31.2) | 3 (30) | >0.99 | |
Child–Pugh >A in cirrhotics | 1 (10) | 2 (100) | 0.04 | |
Tacrolimus‑based immunosuppressive therapy | 43 (89.6) | 8 (80) | 0.59 | |
Cyclosporine‑based immunosuppressive therapy | 5 (10.4) | 2 (20) | 0.59 | |
Time from OLTx to DAA initiation, mo | 17 (10–33) | 30.5 (10–42) | 0.37 | |
Discussion
This retrospective RWE analysis of the individuals with a history of liver transplant for HCV‑related liver cancer was designed to evaluate the safety and effectiveness of DAA therapy in this patient population, and to assess the risk of HCC recurrence after antiviral treatment. Of note, only a few studies published to date evaluated patients with these characteristics, and, to our best knowledge, only 2 of them were conducted in a population larger than ours.19,20 The 58 patients included in the current study came from a population of more than 20 000 patients with CHC treated with DAA therapy at dozens of Polish hepatology centers over nearly a decade. Our cohort exhibited a clear male predominance, which is related to the male sex being a risk factor for the development of HCC, and is in line with other reports.7,23,24
We did not find a significant correlation between the time since OLTx and the degree of fibrosis; although, according to the available literature, longer time since the transplant is associated with a greater risk of fibrosis.25 However, the process of fibrosis development depends on several factors, both in the immediate post‑transplant period and in long‑term observation. These include parameters related to the recipient, the donor, and the transplant procedure. We observed an upward trend in fibrosis advancement over time, although it was not significant (P = 0.42). If we had studied a population with a more extended period between OLTx and DAA therapy, the association with disease progression might have been stronger.
The effectiveness of DAA treatment in the analyzed population was very high, exceeding 98%. The only patient who did not respond to the therapy was a middle‑aged GT1b‑infected woman with previous unsuccessful therapy with PegIFN and ribavirin. Ten years before starting the DAA treatment, she underwent a liver transplant, and at baseline, she was diagnosed with decompensated cirrhosis stage B on the CP scale. Both decompensated cirrhosis and previous failure of standard treatment are considered risk factors for nonresponse to DAA therapy.9 She completed the treatment as planned, without safety issues during therapy and throughout follow‑up.
Overall, more than half of the study population experienced AEs during therapy or the 12‑week follow‑up. Most of the AEs were mild and transient, but 2 events met the criteria for SAEs. In 1 case, it was urosepsis requiring hospitalization, and in the other, early recurrence of HCC with dissemination, which led to discontinuation of the antiviral therapy. This patient died within the 12‑week follow‑up period after treatment. The second death recorded in the study was due to late vascular complications of OLTx, and occurred during treatment. Three patients with cirrhosis reported symptoms of liver decompensation in the form of ascites. However, only 1 patient experienced it for the first time, while the other 2 already had ascites at the beginning of DAA therapy.
The high effectiveness of DAA treatment in patients with HCV infection after OLTx, regardless of the reason for transplant, was confirmed in previous reports.19,26,27 Some authors reported a lower efficacy rate of approximately 90%, which was associated with more advanced liver disease in their study groups, as compared with our population.28 These studies also document a good safety profile of DAA, while pointing out challenges related to potential interactions of all DAA treatment regimens with immunosuppressive drugs. Among the immunosuppressive drugs used in our patients, only mycophenolate mofetil and glucocorticosteroids do not pose a risk of drug–drug interactions; the others (tacrolimus, everolimus, and cyclosporine) show potential interactions with varying degrees of risk with all DAA options. Following the recommendations, the concentration of these drugs was monitored in each patient both during and after therapy, which allowed for the avoidance of safety issues resulting from drug interactions. Potential drug interactions are one of the reasons why this patient population is specific and requires close cooperation between specialists during therapy.
Another feature that makes this population unique is the risk of HCC recurrence after OLTx, which is inherent in the natural history of the disease.8,29 It occurs with a frequency of 8%–20% despite the application of predefined eligibility criteria for OLTx due to HCC.30 It depends on many factors, both related to the tumor (eg, histopathological characteristics, the number of lesions, their size, presence of microvascular invasion, α-fetoprotein levels) and to the patient.31 Patient‑related factors include the coexistence of other liver diseases and a viral etiology of HCC. For the latter factor, the use of antiviral therapy is a potential modifier of the natural history of the disease. While for HBV etiology, the association between successful antiviral therapy with viral load suppression and the risk of HCC recurrence after liver transplantat is well documented, controversial reports emerged for HCV in the early DAA era.31
The debate on the relationship between DAA treatment and HCC recurrence after radical surgery was sparked by the publication of the Barcelona Group study,14 which reported an unexpectedly high rate of early HCC recurrence of 27.6% in their patients, 95% of whom had liver cirrhosis. The phenomenon of HCC recurrence after HCV eradication following DAA therapy is due to the rapid clearance of HCV, which can induce changes in immune cells, cytokine network imbalance, and angiogenesis.32 Although the patients in the abovementioned study were treated with radical surgical methods other than OLTx, similarly to subsequent published analyses from Italy, which reported high HCC recurrence rates of 28.8% (17/59) and 43% (142/328), respectively, these findings provoked a discussion about the safety of DAA therapy after surgical treatment of HCC.15,16 Furthermore, in these analyses, all patients had cirrhosis, which is an independent risk factor for HCC development, even after successful antiviral therapy.33
A French multicenter prospective ANRS CO23 CUPILT (Compassionate Use of Protease Inhibitors in Viral C Liver Transplantation) study19 analyzed patients with HCV‑related HCC treated with OLTx. This study included the largest population analyzed to date in terms of HCC recurrence after DAA treatment.19 In a group of 314 patients, HCC recurred in only 7 individuals (2.2%), 5 of whom died. This percentage was significantly lower than the expected rate of 8%–20%, and recurrence was reported early, at a mean (SD) of 21 (14) weeks after DAA therapy. Since 5 of these 7 patients had risk factors for recurrence related to tumor histologic features, the researchers found no association between antiviral treatment and HCC recurrence. A comparatively low HCV‑related HCC recurrence rate of 3.18% in the patients who underwent a transplant for this reason and subsequently received DAA therapy was documented in a retrospective analysis of data from the United Network for Organ Sharing / Organ Procurement and Transplantation Network database.23 In this study, recurrence was also observed early, within the first few months of DAA therapy. An even lower rate of HCC recurrence in patients treated with OLTx and subsequent DAA therapy was observed in a Latin American population.20 Among 98 patients, HCC recurrence was reported in only 1 person, corresponding to an incidence of 0.7%. The authors of the abovementioned analyses found no evidence linking HCV eradication to an increased incidence of liver cancer recurrence. Other available reports included significantly smaller populations of patients treated with DAA after HCC‑related OLTx than ours, and the results obtained were inconsistent. In a retrospective Canadian study, 2 of 12 patients (16.7%) experienced cancer recurrence during 2‑year follow‑up after DAA therapy.34 Importantly, most of the patients did not meet the Milan criteria at the time of transplant; therefore, they were at a high risk for HCC recurrence. Comparison with a group not treated with DAAs showed no effect of the therapy on the risk of recurrence. It is hard to make a direct comparison between the results of our analysis, documenting a 5.4% HCC recurrence rate, and those of other studies due to differences in the characteristics of the populations analyzed in terms of potential confounding factors and different follow‑up periods. The value obtained in our study is higher than those described above, but lower than the 8%–20% risk expected based on historical data on HCC recurrence after OLTx. Thus, our study provides evidence that the risk of HCC recurrence in LTx recipients who subsequently received DAA therapy is not elevated.
On the other hand, a preliminary retrospective study conducted at a Polish transplant center showed HCC recurrence in 8 out of 19 patients (42.1%) after DAA treatment.28 However, in the control group of individuals not treated with DAAs, this percentage was higher (21/32; 65.6%; P = 0.06), confirming the lack of impact of DAA therapy on the risk of HCC recurrence. Furthermore, in that study, all patients in both subgroups had advanced cirrhosis, which influenced the final results. Regardless of the frequency of HCC recurrence in patients with a history of OLTx, in all studies, recurrences took place early, up to 2 years after the end of DAA therapy, which is consistent with our results.19,20,28,34 In long‑term follow‑up after treatment, we observed an all‑cause mortality rate of 17%, of which less than one‑third were deaths due to HCC recurrence. The overall 6‑year survival rate in our analysis was 85%. A study evaluating the survival of patients after OLTx for HCC, taking the time of surgery as a reference point, showed a 5‑year survival rate of 78.5%.35
A crucial decision to make for a patient with HCV‑related HCC with indications for LTx is the timing of the surgery and DAA therapy. According to current recommendations, the decision is case‑by‑case and based on a detailed analysis of the patient in close collaboration between hepatologists and transplantologists, taking into account the likelihood of response to HCV therapy and access to LTx.10,11 A single‑center study involving a group of patients with HCV‑related HCC treated with OLTx after virologically effective DAA therapy documented the beneficial effect of this approach on reducing the risk of HCC recurrence and patient survival.20
Our study has some limitations that should be acknowledged. These limitations stem from the retrospective nature of the analysis, which may cause possible bias and gaps in the collected data. We did not collect data on the characteristics of the liver tumor prior to OLTx, including fulfillment of the Milan criteria and other criteria used to qualify the patients for transplant. We did not collect data on initial HCC therapy or procedures performed to downstage the disease prior to OLTx. We also did not gather data on the location of HCC recurrence, whether local or extrahepatic. Finally, our study did not feature a control group, so we compared our results with published historical data. However, our analysis was performed in a large group of individuals selected from an extensive multicenter cohort of RWE patients treated for nearly a decade, since the beginning of the DAA era, which we consider to be a significant advantage of the study. In addition, we included patients treated with new pangenotypic options and collected long‑term data on all participants. Furthermore, the long‑term follow‑up period in our study was the longest of any published analysis to date.
Conclusions
In this study, which included all consecutive patients with HCV‑related HCC who received antiviral treatment after OLTx, selected from a large population of patients treated since the beginning of the DAA era, we observed a very high cure rate of over 98%. The HCC recurrence rate during long‑term follow‑up was only 5.4%. Although this value is lower than expected based on the natural history of the disease, patients with HCV‑related HCC require vigilant monitoring for tumor recurrence.
- Brzdęk M, Zarębska‑Michaluk D, Invernizzi F, et al. Decade of optimizing therapy with direct‑acting antiviral drugs and the changing profile of patients with chronic hepatitis C. World J Gastroenterol. 2023; 29: 949‑966. | Crossref
- Starnawski P, Nowak K, Augustyn Z, et al. Role of hepatotropic viruses in promoting hepatocellular carcinoma‑current knowledge and recent advances. Med Oncol. 2025; 42: 111. | Crossref
- World Health Organization. Hepatitis C. https://www.who.int/news‑room/fact‑sheets/detail/hepatitis‑c. Accessed August 13, 2025. | Crossref
- Weigand K, Stremmel W, Encke J. Treatment of hepatitis C virus infection. World J Gastroenterol. 2007; 13: 1897‑1905. | Crossref
- Flisiak R, Zarębska‑Michaluk D, Janczewska E, et al. Five‑years follow‑up of cured HCV patients with or without cirrhosis under real‑world interferon‑free therapy. J Hepatol. 2022; 77: S565‑S566. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION