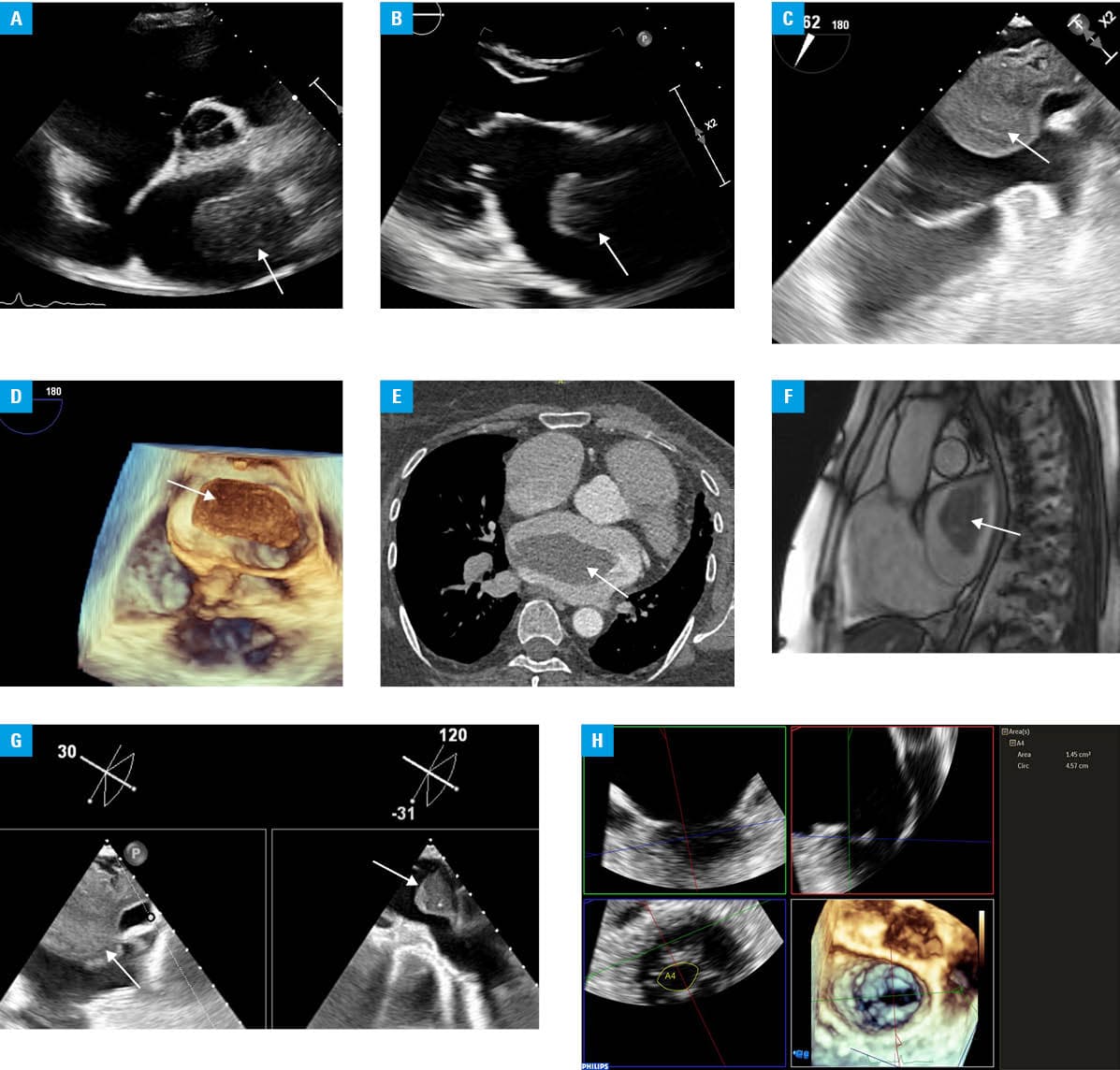
A 63‑year‑old woman with permanent atrial fibrillation (AF) was admitted urgently to our hospital due to a large mass in the left atrium (LA), detected on transthoracic echocardiography (Figure 1A and 1B). The patient had previously been treated for breast cancer. At the time of hospital admission, she reported dizziness when standing and discomfort associated with arrhythmia (European Heart Rhythm Association class 2b). Laboratory tests showed an elevated D‑dimer level (1957 ng/ml; reference range [RR] <500 ng/ml). Transesophageal echocardiography (TEE; Figure 1C and 1D) was performed, followed by computed tomography (CT; Figure 1E) and cardiac magnetic resonance imaging (MRI; Figure 1F), which identified a mass attached to the LA roof, measuring approximately 7 cm × 3 cm × 6 cm, narrowing the ostium of both superior pulmonary veins (Figure 1G). According to CT and MRI, the image primarily corresponded to a thrombus. Differential diagnosis also included a primary cardiac tumor (myxoma) or, given the patient’s oncologic history, a metastatic lesion. TEE also showed moderate rheumatic mitral valve disease (mitral valve area on 3‑dimentional echocardiography measured 1.5 cm²; Figure 1H) and severe, eccentric tricuspid regurgitation due to annular dilation and prolapse of the septal leaflet. After excluding cancer recurrence, the heart team decided on urgent cardiac surgery. During the procedure, the LA mass was completely removed. The operator macroscopically suspected a myxoma. A mechanical St. Jude Medical 29M mitral valve prosthesis (Abbott Laboratories, Chicago, Illinois, United States) was implanted. Tricuspid valve repair was performed with placement of a 34‑mm tricuspid annuloplasty ring (Edwards Lifesciences, Irvine, California, United States). The left atrial appendage was closed using a 40‑mm AtriClip (AtriCure, Inc., Mason, Ohio, United States). Postoperative recovery was uneventful. Histopathologic analysis of the excised lesion showed that the mass was a thrombus.
A detailed review of the patient’s anticoagulation therapy history indicated that from the diagnosis of mixed mitral valve disease (at that time, the mitral valve area was assessed at 1.8 cm², with a mean mitral gradient of 5 mm Hg), a cardiologist switched the patient from dabigatran to warfarin. Several years later, the patient was diagnosed with breast cancer and started oncologic treatment. The oncologist then changed the anticoagulation from warfarin to enoxaparin at a dose of 80 mg once daily. Two years after the completion of cancer therapy, the patient was admitted to our hospital with the described giant LA thrombus and was still on a reduced dose of LMWH. Of note, the patient’s body weight was 91 kg and renal function was normal (creatinine, 78 µmol/l; reference range [RR], 44–80 µmol/l; estimated glomerular filtration rate based on the Modification of Diet in Renal Disease eqution, 70 ml/min; RR >60 ml/min). She reported no recent severe bleeding episodes and her hemoglobin level was 15.4 g/dl (RR, 12–16 g/dl). Switching from direct anticoagulants to vitamin K antagonists is recommended in patients with AF and rheumatic mitral stenosis, with a mitral valve area smaller than or equal to 2 cm2.1 Due to long‑lasting AF, a moderate mitral stenosis with a significantly enlarged LA (LA volume index, 88 ml/m² of the body surface area), and a history of cancer, our patient certainly had a very high risk of thromboembolism.2 Therefore, she required a therapeutic, rather than prophylactic, dose of anticoagulants.
- Praz F, Borger MA, Lanz J, et al. 2025 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio‑Thoracic Surgery (EACTS). Eur Heart J. 2025 Aug 29:ehaf194. | Crossref
- Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio‑Thoracic Surgery (EACTS): developed by the Task Force for the management of atrial fibrillation of the European Society of Cardiology (ESC), with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Endorsed by the European Stroke Organisation (ESO). Eur Heart J. 2024; 45: 3314‑3414. | Crossref
ARTICLE INFORMATION