Prostate-specific membrane antigen expression in bone metastases of lung adenocarcinoma: implications for diagnostic and therapeutic strategies
1



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Prostate-specific membrane antigen expression in bone metastases of lung adenocarcinoma: implications for diagnostic and therapeutic strategies
A 58‑year‑old man presented with a 1‑month history of dysuria. Laboratory test results showed an elevated level of serum prostate‑specific antigen (PSA) of 8.3 ng/ml (reference range, 0–4 ng/ml). Magnetic resonance imaging (MRI) showed a T2‑weighted hypointense lesion in the prostatic peripheral zone (Figure 1A) and multiple abnormal signal foci in the pelvic bones, supporting a provisional diagnosis of prostate adenocarcinoma with suspected osseous metastases.
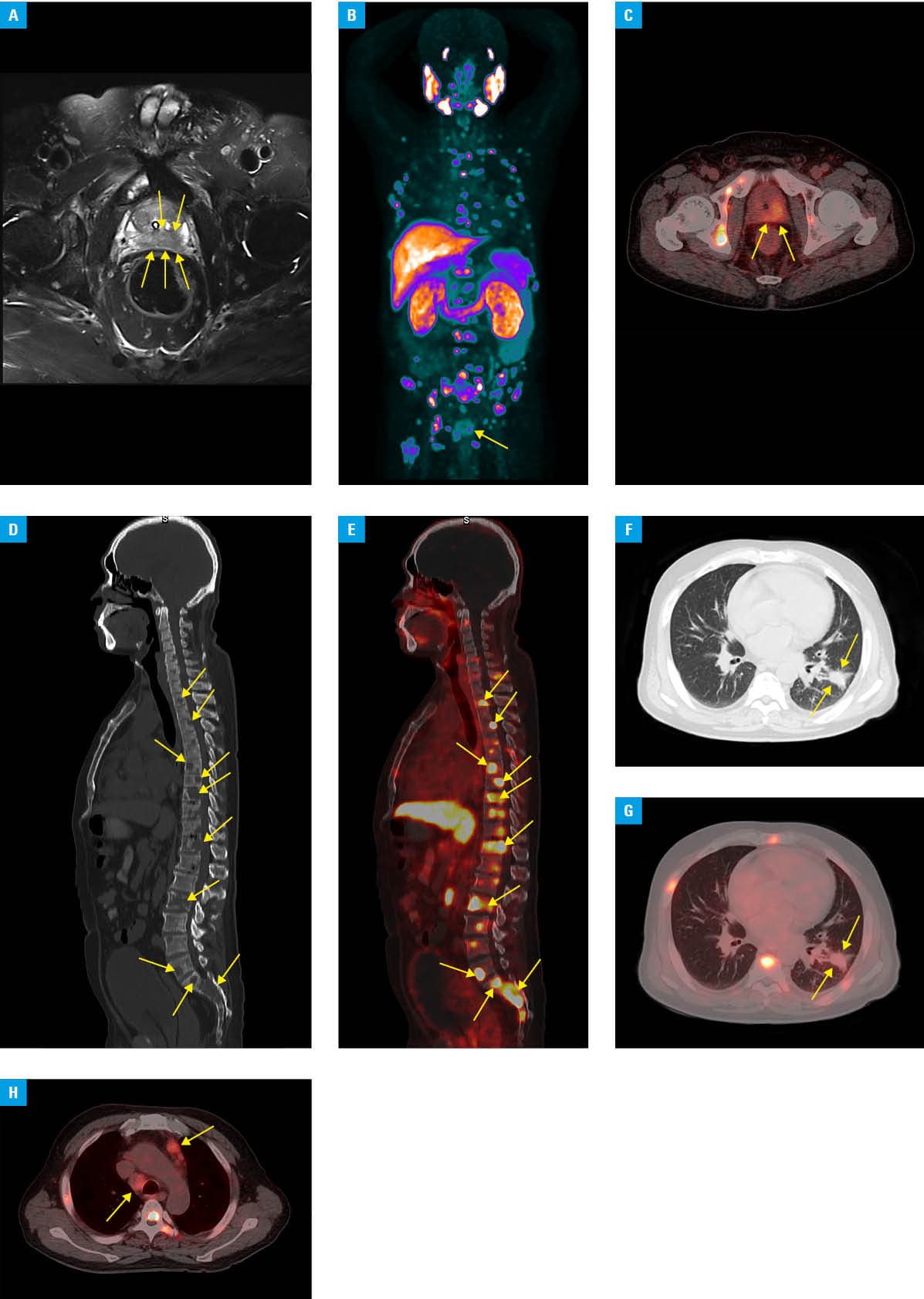
Abbreviations: 18F PSMA, fluorine‑18 prostate specific membrane antigen; PET/CT, positron emission tomography / computed tomography; SUVmax, maximum standardized uptake value
Subsequent fluorine‑18 prostate specific membrane antigen (PSMA)-1007 positron emission tomography / computed tomography (PET/CT) imaging identified moderate PSMA expression within the prostate gland, with a maximum standardized uptake (SUVmax) value of 6.5 (Figure 1B and 1C), which corresponded to the T2‑weighted hypointense area found on MRI. Additionally, multiple osteolytic bone lesions demonstrating markedly increased PSMA avidity (SUVmax, 36.2) were identified in the skull, spine, pelvis, bilateral scapulae, ribs, and sternum, suggestive of metastatic involvement (Figure 1D and 1E). A spiculated, lobulated soft tissue mass in the left lung exhibited faint PSMA expression (SUVmax, 2.2; Figure 1F and 1G). Furthermore, multiple enlarged mediastinal lymph nodes were observed, some of which demonstrated faint‑to‑moderate PSMA uptake (SUVmax range, 2–5.6; Figure 1H). Histologic and immunohistochemical analysis of ultrasound‑guided prostate biopsy established a diagnosis of metastatic pulmonary adenocarcinoma, with positive immunostaining for thyroid transcription factor‑1 and napsin A. The biopsy also showed benign prostatic hyperplasia with inflammatory infiltrates, which could account for the elevated PSA levels. Primary lung adenocarcinoma was confirmed on the histopathologic analysis of CT‑guided biopsy from the left lung lesion. Based on the integration of the biopsy and PET/CT imaging findings, the patient was diagnosed with left lung adenocarcinoma, presenting with extensive metastases involving multiple lymph node stations, bones, and the prostate.
Varying degrees of PSMA expression have been reported in multiple nonprostate malignancies, and cases of nonprostate cancer patients treated with PSMA‑directed radioligand therapy (PSMA‑RLT) have also been described in the literature.1 Previous studies have established significant PSMA overexpression in osseous metastases from renal cell carcinoma, with SUVmax ranging from 10 to 46.3.2 Here, we present a case of lung adenocarcinoma with multiple, intensely PSMA‑avid osteolytic bone metastases.
Skeletal metastases, occurring in 40%–60% of the patients with advanced lung adenocarcinoma, frequently lead to skeletal‑related events that markedly impair quality of life and correlate with reduced overall survival.3,4 Although standard therapies (eg, bisphosphonates, denosumab, or radiation) achieve symptomatic control in 60%–75% of the cases, high rates of refractory or recurrent disease underscore the need for novel targeted treatments.4 The considerable heterogeneity in PSMA expression between primary lung adenocarcinoma and its metastatic lesions exhibits a clear organotrophic pattern, with the unique tumor microenvironment of osseous metastases being the likely underlying driver of the notably intense avidity observed. These features support the use of α-emitting (eg, actinium‑225) or β-emitting (eg, lutetium‑177) PSMA‑RLT as a potential therapeutic option for refractory osseous metastases in selected patients with PSMA‑avid lung adenocarcinoma. Prior studies have shown a strong correlation between PSMA uptake and vascular endothelial growth factor receptor (VEGFR) / platelet‑derived growth factor receptor (PDGFR) expression.5 This molecular link supports combining PSMA‑targeted therapies with VEGFR/PDGFR inhibitors to potentially enhance efficacy in advanced lung adenocarcinoma with bone metastases. Further studies to answer various theragnostic considerations are required to guide their use in a real‑world setting.
- de Vries LH, Lodewijk L, Braat AJAT, et al. 68Ga‑PSMA PET/CT in radioactive iodine‑refractory differentiated thyroid cancer and first treatment results with 177Lu‑PSMA‑617. EJNMMI Res. 2020; 10: 18. | Crossref
- Gasparro D, Scarlattei M, Silini EM, et al. High prognostic value of 68Ga‑PSMA PET/CT in renal cell carcinoma and association with PSMA expression assessed by immunohistochemistry. Diagnostics. 2023; 13: 3082. | Crossref
- Tsuya A, Kurata T, Tamura K, et al. Skeletal metastases in non‑small cell lung cancer: a retrospective study. Lung Cancer. 2007; 57: 229‑232. | Crossref
- Coleman RE. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev. 2001; 27: 165‑176. | Crossref
- Gao J, Meng L, Xu Q, et al. 68Ga‑PSMA‑11 PET/CT parameter correlates with pathological VEGFR‑2/PDGFR-β expression in renal cell carcinoma patients. Mol Imaging Biol. 2022; 24: 759‑768. | Crossref
ARTICLE INFORMATION