Implementation of recommendations regarding pharmacotherapy optimization in patients with heart failure with reduced ejection fraction undergoing scheduled hospitalization: the HEROES study
Key words: chronic heart failure, guideline-directed medical therapy, natriuretic peptide, real-life observational study

 CC BY 4.0
CC BY 4.0
Implementation of recommendations regarding pharmacotherapy optimization in patients with heart failure with reduced ejection fraction undergoing scheduled hospitalization: the HEROES study
Introduction: Optimization of guideline‑directed medical therapy (GDMT) to improve the prognosis of patients with heart failure (HF) is one of the main goals of chronic care.
Objectives: We aimed to assess implementation of the recommendations regarding GDMT optimization in HF patients undergoing scheduled hospitalization, with particular emphasis on the patients with reduced left ventricular ejection fraction (LVEF).
Patients and methods: Our analysis included 412 patients with known LVEF (mean [SD] age, 66.7 [13.5] y; 297 men) admitted for elective hospitalization, representing a subset of 1422 participants of the HEROES study (Heart Failure Observational Study of the Polish Cardiac Society). Recruitment across 41 Polish centers took place from April 2022 to May 2024.
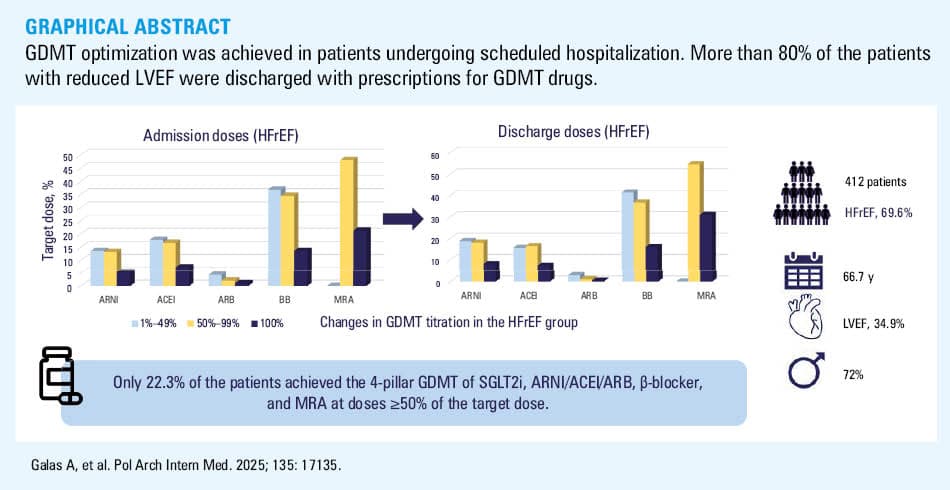
Results: Mean (SD) LVEF in the study group was 34.9% (14.4%). The patients with HF with reduced LVEF (HFrEF) constituted 69.7% (n = 287) of the whole group. In this subgroup, the use of angiotensin receptor‑neprilysin inhibitor (ARNI) / angiotensin‑converting enzyme inhibitor (ACEI) / angiotensin receptor blocker (ARB) increased from 81.5% of the patients at admission to 88.9% at discharge, of β-blocker from 85% to 94.4%, of mineralocorticoid receptor antagonist (MRA) from 69.7% to 86.1%, and of sodium‑glucose cotransporter 2 inhibitor (SGLT2i) from 59.2% to 83.6%. ARNI/ACEI/ARB therapy was optimized in 36.2% of the participants, while the rates of optimization were 24.7%, 27.2%, and 24.4% for β-blockers, MRA, and SGLT2i, respectively. However, only 64 patients (22.3%) attained the 4‑pillar GDMT of SGLT2i, ARNI/ACEI/ARB, β-blockers, and MRA at doses equal to or above 50% of the target dose.
Conclusions: In the Polish multicenter HEROES registry, over 80% of the patients with HFrEF were discharged on 4‑pillar GDMT. Nevertheless, the attainment of target high‑dose GDMT remained suboptimal. These findings provide new insights into the variability of GDMT implementation at the national level and underline the need for strategies to improve dosing optimization.
What's new?
Despite strong evidence supporting guideline‑directed medical therapy (GDMT) in heart failure (HF), real‑world implementation remains suboptimal, especially in clinically stable patients. This challenge is exacerbated during planned hospitalizations, where short stays and medical staff workload may limit therapeutic adjustments. Treatment inertia is notable among stable patients, emphasizing missed opportunities for GDMT optimization. Our study uniquely assessed GDMT optimization during elective hospital admissions in a real‑world Polish HF population, focusing on HF with reduced ejection fraction (HFrEF). Using data from the HEROES registry, we observed significant improvements in initiation and up‑titration of key therapies—β-blockers, renin‑angiotensin system inhibitors, mineralocorticoid receptor antagonists, and sodium‑glucose cotransporter 2 inhibitors—in the HFrEF subgroup. These findings highlight elective hospitalizations as vital moments for improving pharmacologic treatment, revealing gaps in practice and offering insights to enhance personalized, evidence‑based care and outcomes in HF, both locally and globally.
Introduction
Heart failure (HF) is a major cause of hospitalization in patients over 65 years of age, mainly due to its exacerbation.1-6 However, stable HF patients may also require hospitalization for scheduled revascularization, ablation, elective electrical cardioversion, or implantation of cardioverter‑defibrillators (ICDs) or cardiac resynchronization therapy (CRT) devices.1 The outcomes of HF patients could be improved using guideline‑directed medical therapy (GDMT)1,2 with angiotensin receptor‑neprilysin inhibitors (ARNIs), angiotensin‑converting enzyme inhibitors (ACEIs), β-blockers, mineralocorticoid receptor antagonists (MRAs), and sodium glucose cotransporter 2 inhibitors (SGLT2is). In the case of ACEI intolerance, angiotensin receptor blockers (ARBs), also referred to as renin‑angiotensin‑aldosterone system inhibitors (RAASis), may be used instead.
Each medical contact with an HF patient should be perceived as an opportunity to optimize pharmacotherapy, increase the doses of GDMT, or initiate therapy if it has not been used previously. However, most hospitalizations for the diagnosis or advanced treatment of HF are elective and focus on performing planned procedures. The tendency to shorten hospitalizations, high workloads of medical staff, and stable patient status may affect the eagerness of health care professionals to optimize therapy, especially in patients with reduced left ventricular ejection fraction (LVEF); this is despite the presence of guidelines that should be used as the cornerstone of therapeutic decisions.1,7 The real‑world data are concerning and reveal regional differences. In the CHAMP‑HF (Change the Management of Patients with Heart Failure) registry, which included 3518 HF individuals with mean (SD) LVEF of 29% (8%), only 18%, 14%, and 28% of the patients attained the target doses of ACEI, ARNI, and β-blockers, respectively. Moreover, only 1% were prescribed the target maximum dose for all recommended medications.8 In the GUIDE‑IT trial (Guiding Evidence Based Therapy Using Biomarker Intensified Treatment), 99.3% and 68.3% of the patients with HF and reduced LVEF (HFrEF) in Canada used β-blockers and MRA, respectively; this was significantly higher than in the United States (94.1% and 55.1%, respectively).9 The practices of Polish centers regarding this issue have not been analyzed previously.
Therefore, we aimed to assess implementation of the recommendations1,7 regarding GDMT optimization in the participants of the HEROES study (Heart Failure Observational Study of the Polish Cardiac Society) who were undergoing scheduled hospitalization, with a particular emphasis on patients with HFrEF.
Patients and methods
The HEROES registry was a prospective, multicenter, observational study endorsed by the Polish Cardiac Society, which enrolled HF patients (with preserved, mildly‑reduced, and reduced LVEF) in hospital and ambulatory settings, and was conducted in 41 Polish clinical centers. There were no specific exclusion criteria, with the exception of the patient’s unwillingness to participate.10
The study was designed to ensure broad geographic representation across Poland by including centers with variable availability of equipment: 25% with on‑site cardiac surgery operating room, 25% with a hemodynamics laboratory but no cardiac surgery operating room, and 50% without either facility. The patients included in the registry were all individuals admitted on designated weekdays in each center for various planned or urgent procedures with a current or prior diagnosis of HF; however, this analysis included only those hospitalized on a scheduled basis.
This study was mainly conducted before the era of the recommendations for SGLT2is in the treatment of HF with LVEF above 40%.11,12 Thus, the use of this class of medications was only mentioned in Supplementary material, Table S1.
The Bioethical Committee of the Medical University of Lodz approved implementation of the HEROES study (RNN/316/20/KE with the KE/762/23 update). The data were collected between April 2022 and May 2024.
The gathered data included demographics, anamnesis with special attention to HF history, HF hospitalizations and etiology, comorbidities, and medications at admission and discharge. Diagnostic test results were also accounted for, but we only included the tests deemed necessary by the physician to evaluate the hospitalized patient. These may have involved laboratory tests (blood count, liver function markers, serum creatinine, serum sodium and potassium, and estimated glomerular filtration rate) and transthoracic echocardiography with LVEF assessment. The study design and methodology were presented in detail previously.10
In this analysis, we assessed the frequency of changes in particular GDMT drug classes (introduction or up‑titration) during scheduled hospitalizations (in patients who were admitted for planned diagnostic or therapeutic procedures, such as coronary angiography, coronary angioplasty, ablation, and implantation or replacement of implantable devices; excluding patients hospitalized for HF exacerbation), with particular emphasis on patients with HFrEF. We defined “therapy optimization” as a dosage increase of any of ACEIs, ARBs, ARNIs, β-blockers, MRAs, or SGLT2is, as well as any switch from ACEI or ARB to ARNI or from ARB to ACEI. High GDMT doses were defined as achieving all 4 pillars—SGLT2i, ARNI/ACEI/ARB, β-blockers, and MRA—at doses equal to or above 50% of the target dose. The analysis was conducted in 412 patients with known LVEF values who underwent planned hospitalization and who were selected from the 1422 participants of the HEROES study (Figure 1).
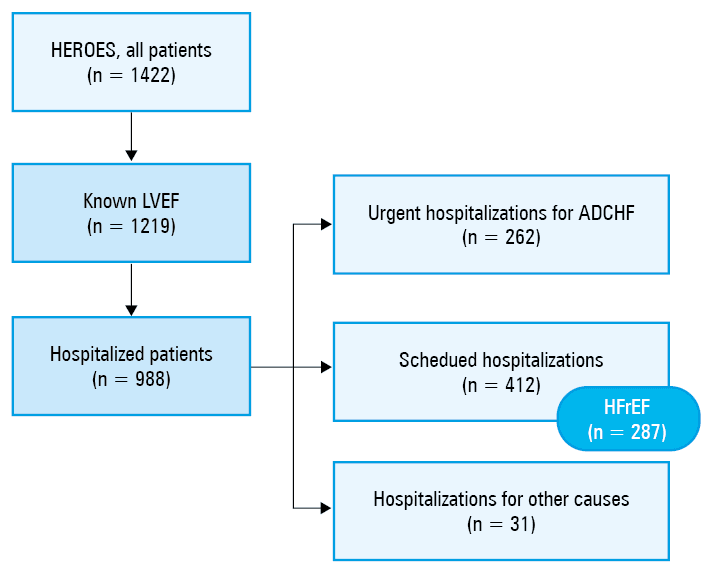
Abbreviations: ADCHF, acute decompensation of chronic heart failure; LVEF, left ventricular ejection fraction
Statistical analysis
To describe quantitative variables, we used mean and SD for normal distributions and median and interquartile range (IQR) for non‑normal distributions. The normality of the variable distribution was verified using the Shapiro–Wilk test. For categorical variables, the number of observations for each category with the corresponding percentage was presented. To compare paired categorical data, the McNemar test was used. A P value below 0.05 was considered significant. The analysis was performed using STATISTICA PL 13.3 package (TIBCO Software Inc., Palo Alto, California, United States).
Results
General characteristics of the study group
Median (IQR) age in the study group (297 men and 115 women) was 68 (59.2–76.3) years, with median (IQR) LVEF of 32% (24%–45%). The study group was dominated by patients with HFrEF (69.6%; n = 287; Figure 1). The patients with LVEF above 40% constituted 30.3% (n = 125) of the whole group: 40 with HF with mildly reduced EF (HFmrEF) and 85 with HF with preserved EF (HFpEF). De novo HF was diagnosed in 56 patients (13.4%). Detailed characteristics of the study participants are presented in Table 1. In the analysis for the whole group (regardless of EF), ARNI/ACEI/ARB use increased from 78.1% (n = 324) at admission to 85.4% (n = 352) at discharge. β-blocker use increased from 82.3% (n = 339) to 91.3% (n = 376), MRA from 60.4% (n = 249) to 73.8% (n = 304), and SGLT2i from 46.8% (n = 193) to 68.2% (n = 281; P <0.01 for all). Therapy with ARNI/ACEI/ARB was optimized in 33.3% of the patients (n = 137), with optimization rates of 25.2% (n = 104), 23.5% (n = 97), and 21.3% (n = 88) for β-blockers, MRA, and SGLT2i, respectively (Table 2; Supplementary material, Table S2). A considerable increase in diuretic usage was also noted (from 74.1% to 87.8%; P <0.01).
Characteristics | Study group (n = 412) | ||
Data are presented as number (percentage) or median (interquartile range).
a The number of patients with available data (if not available for all participants)
b Patient‑reported reduction in the ability to perform activities of daily living, as further detailed by the NYHA functional classification
c Vitamin K antagonists, n = 52 (25.2%)
Abbreviations: BMI, body mass index; CRT, cardiac resynchronization therapy; eGFR, estimated glomerular filtration rate; HF, heart failure; ICD, implantable cardioverter‑defibrillator; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide; NYHA, New York Heart Association; others, see Figure 1 | |||
Age, y | 68 (59.2–76.3) | ||
Women | 115 (27.9) | ||
BMI, kg/m2 (n = 406)a | 28 (24.9–32) | ||
At least 1 HF hospitalization in the last 6 months | 155 (51) | ||
Prior diagnosis of HF | 356 (86.4) | ||
HF with ischemic etiology | 154 (37.4) | ||
LVEF, % | 32 (24–45) | ||
Length of hospital stay, d | 6.5 (4–10) | ||
Smoking status | Current | 72 (17.5) | |
Former | 165 (40) | ||
Never | 175 (42.5) | ||
Clinical status at admission | |||
NYHA | Class I | 27 (6.6) | |
Class II | 133 (32.2) | ||
Class III | 188 (45.6) | ||
Class IV | 48 (11.7) | ||
Forester classification | Dry‑warm | 274 (66.5) | |
Dry‑cold | 133 (32.3) | ||
Wet‑warm | 1 (0.2) | ||
Wet‑cold | 4 (1) | ||
Systolic blood pressure, mm Hg | 125 (110–140) | ||
Diastolic blood pressure, mm Hg | 77 (70–85) | ||
Heart rate, bpm | 77 (66–90) | ||
Reduced exercise toleranceb | 277 (67.2) | ||
Dyspnea at rest | 90 (21.8) | ||
Orthopnea | 82 (19.9) | ||
Pulmonary rales | 143 (34.7) | ||
Peripheral edema | 177 (43) | ||
Hepatomegaly | 25 (6.1) | ||
Ascites | 16 (3.9) | ||
Laboratory results | |||
Hemoglobin, g/dl (n = 403)a | 13.8 (12.3–15) | ||
eGFR, ml/min/1.73 m2 (n = 394)a | 66 (49–96) | ||
eGFR <60 ml/min/1.73 m2 | 168 (42.7) | ||
eGFR <30 ml/min/1.73 m2 | 34 (8.6) | ||
Sodium, mmol/l (n = 397)a | 140 (138–142) | ||
Potassium, mmol/l (n = 400)a | 4.5 (4.1–4.8) | ||
NT‑proBNP, pg/ml (n = 324)a | 2569 (1020–6433) | ||
Comorbidities / procedures | |||
Coronary artery disease | 189 (45.9) | ||
Arterial hypertension | 258 (62.6) | ||
Valvular intervention | 29 (7) | ||
Chronic obstructive pulmonary disease | 49 (11.9) | ||
Asthma | 13 (3.2) | ||
Chronic kidney disease | 117 (28.4) | ||
Depression | 12 (2.9) | ||
Peripheral arterial disease | 21 (5.1) | ||
Severe liver insufficiency | 3 (0.7) | ||
Cancer | 28 (6.8) | ||
Atrial fibrillation | 224 (54.4) | ||
Diabetes mellitus | 165 (40) | ||
Implanted CRT device | 52 (12.7) | ||
Implanted ICD | 118 (28.7) | ||
Medications (n = 410)a | At admission | At discharge | |
Ivabradine | 21 (5.1) | 52 (12.6) | |
Diuretics | 304 (74.1) | 360 (87.8) | |
Digoxin | 41 (10) | 47 (11.5) | |
Statins | 284 (69.2) | 318 (77.6) | |
Antiplatelets | 158 (38.5) | 158 (38.5) | |
Anticoagulants | 206 (50.2)c | 233 (56.8) | |
Dihydropyridine calcium blockers | 67 (16.3) | 66 (16.1) | |
Nondihydropyridine calcium blockers | 2 (0.5) | 2 (0.5) | |
Amiodarone | 63 (15.3) | 64 (15.6) | |
Medication class | Usage at admission | Usage at discharge | Admission dose | Discharge dose | Up‑titration / down‑titration | ||
% of target dose category | n, % | % of target dose category | n, % | ||||
Data are presented as number (percentage).
a P <0.01 (for total ARNI/ACEI/ARB, see main text)
b P <0.01
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor‑neprilysin inhibitor; MRA, mineralocorticoid receptor antagonist; SGLT2i, sodium glucose cotransporter 2 inhibitor | |||||||
ARNI | 97 (23.5) | 134 (32.5)a | 1–49 | 42 (10.2) | 1–49 | 57 (13.8) | 54 (13.1) / 3 (0.7) |
50–99 | 40 (9.7) | 50–99 | 54 (13.1) | ||||
100 | 15 (3.6) | 100 | 23 (5.6) | ||||
ACEI | 181 (43.9) | 183 (44.4)a | 1–49 | 70 (17) | 1–49 | 60 (14.6) | 70 (17) |
50–99 | 71 (17.2) | 50–99 | 81 (19.7) | ||||
100 | 38 (9.2) | 100 | 39 (9.5) | ||||
ARB | 46 (11.2) | 35 (8.5)a | 1–49 | 20 (4.9) | 1–49 | 25 (6.1) | 13 (3.2) / 9 (2.2) |
50–99 | 28 (6.8) | 50–99 | 7 (1.7) | ||||
100 | 7 (1.7) | 100 | 2 (0.7) | ||||
β-Blocker | 339 (82.3) | 376 (91.3)b | 1–49 | 148 (35.9) | 1–49 | 168 (40.8) | 104 (25.2) / 40 (9.7) |
50–99 | 144 (35) | 50–99 | 154 (37.4) | ||||
100 | 47 (11.4) | 100 | 54 (13.1) | ||||
MRA | 249 (60.4) | 304 (73.8)b | 1–49 | 0 | 1–49 | 0 | 97 (23.5) / 23 (5.6) |
50–99 | 169 (41) | 50–99 | 194 (47.1) | ||||
100 | 79 (19.2) | 100 | 109 (26.5) | ||||
SGLT2i | 193 (46.8) | 281 (68.2)b | 100 | 193 (46.8) | 100 | 281 (68.2) | 88 (21.3) |
Characteristics of the heart failure with reduced ejection fraction subgroup
The patients with reduced LVEF constituted 69.7% (n = 287) of the whole group. They were predominantly men (n = 232; 80.8%), at a mean (SD) age of 63.6 (13.7) years and with mean (SD) LVEF of 26.9% (8.2%). Of these patients, 44 (15.4%) had a CRT device implanted, and 104 (36.4%) had an ICD. In the analysis of the subgroup with reduced EF, ARNI/ACEI/ARB use increased from 81.6% (n = 234) at admission to 88.9% (n = 254) at discharge, β-blocker use from 85% (n = 244) to 94.4% (n = 271), MRA from 69.7% (n = 200) to 86.1% (n = 247), and SGLT2i from 59.2% (n = 170) to 83.6% (n = 240; P <0.01 for all). Therapy with ARNI/ACEI/ARB was optimized in 36.2% (n = 104) of the patients, with optimization rates of 24.7% (n = 71), 27.2% (n = 78), and 24.4% (n = 70) for β-blockers, MRAs, and SGLT2is, respectively (Table 3). However, only 64 patients (22.3%) achieved the 4‑pillar GDMT of SGLT2i, ARNI/ACEI/ARB, β-blocker, and MRA at doses equal to or above 50% of the target dose (Supplementary material, Table S3). A clear increase in diuretic usage was also noted (from 77.2% to 88.4%; P <0.01).
Medication class | Usage at admission | Usage at discharge | Admission dose | Discharge dose | Up‑titration / down‑titration | ||
% of target dose category | n, % | % of target dose category | n, % | ||||
Data are presented as number (percentage).
a P <0.01 (for total ARNI/ACEI/ARB, see main text)
b P <0.01
Abbreviations: see Table 2 | |||||||
ARNI | 92 (32.1) | 128 (44.6)a | 1–49 | 39 (13.6) | 1–49 | 53 (18.5) | 53 (18.5) / 3 (1) |
50–99 | 38 (13.2) | 50–99 | 52 (18.1) | ||||
100 | 15 (5.2) | 100 | 23 (8) | ||||
ACEI | 120 (41.8) | 114 (40)a | 1–49 | 51 (17.8) | 1–49 | 45 (15.7) | 44 (15.3) / 18 (6.3) |
50–99 | 48 (16.7) | 50–99 | 47 (16.4) | ||||
100 | 21 (7.3) | 100 | 21 (7.3) | ||||
ARB | 22 (7.7) | 12 (4.2)a | 1–49 | 12 (4.2) | 1–49 | 8 (2.8) | 7 (2.4) / 4 (1.4) |
50–99 | 6 (2.1) | 50–99 | 3 (1) | ||||
100 | 3 (1) | 100 | 1 (0.3) | ||||
β-Blocker | 244 (85) | 271 (94.4)b | 1–49 | 106 (36.9) | 1–49 | 135 (41.5) | 71 (24.7) / 27 (9.4) |
50–99 | 99 (34.5) | 50–99 | 106 (36.9) | ||||
100 | 39 (13.6) | 100 | 46 (16) | ||||
MRA | 200 (69.7) | 247 (86.1)b | 1–49 | 0 | 1–49 | 0 | 78 (27.2) / 10 (3.5) |
50–99 | 138 (48.1) | 50–99 | 157 (54.7) | ||||
100 | 61 (21.3) | 100 | 98 (31) | ||||
SGLT2i | 170 (59.2) | 240 (83.6)b | 100 | 170 (59.2) | 100 | 240 (83.6) | 70 (24.4) |
Discussion
Our analysis of the HEROES study provides a focused evaluation of the implementation of GDMT in Poland in the patients with HF during planned hospitalizations. Our findings indicate that scheduled hospitalizations were generally used as an opportunity to optimize GDMT, with the majority of patients discharged on recommended therapies—most patients were using ARNI/ACEI/ARB (94%), β-blockers (94%), MRA (86%), and SGLT2i (84%). However, given the study’s limitations and the specific national setting, these results should be interpreted cautiously, and may not be directly generalizable. Moreover, it is important to highlight that this is the first study assessing changes in GDMT utilization in the patients with HF undergoing scheduled hospitalization, not only in Poland but also on a global scale.
At the time of data collection, an update to the HF treatment guidelines was released; however, these revisions pertained specifically to patients with HFmrEF and HFpEF,7 and did not impact the treatment of patients with chronic HFrEF, which was the focus of this study. Still, this led to increased use of SGLT2is in the HFmrEF and HFpEF groups following the release of the guidelines (Supplementary material, Tables S1 and S4).
Our results seem to support the fact that reaching 100% adherence is impossible due to inherent limitations. Ken Lee Chin et al13 demonstrated that about 7% of patients with HFrEF have contraindications or intolerance to ACEI/ARB and β-blockers, meaning that in real life, no more than 93% of the patients can achieve all 4 pillars of GDMT.
In the HEROES group, β-blockers and RAASis were the most commonly prescribed drugs, as was the case in previous registries. In the RECOLFACA registry (Colombian Heart Failure Registry), conducted in Colombia—a country classified as low‑income one—high rates of GDMT were observed among ambulatory HF patients, with usage rates of β-blockers, RAASi, and MRA reaching 88.9%, 72.3%, and 67.9%, respectively.14 Surprisingly, an ARNI was prescribed in only 13.1% of the patients. In contrast, treatment coordinated by primary care in ambulatory HFrEF patients included β-blockers and MRA less frequently (74% and 20%, respectively).15 Notably, the implementation of RAASi in our group was found to be similar to that in the European Society of Cardiology (ESC) Heart Failure Long Term registry (92%)16 and ESC‑HF pilot study (88%).17 In the ATA (Adherence to Guideline‑Directed Medical and Device Therapy in Outpatients with HFrEF) study,18 RAASis were used in 78.2% of the patients. Interestingly, the highest uptake of MRA in Asia was observed in China (78%), which was still lower than in our analysis.19 Furthermore, the Chinese patients had the lowest uptake of RAASi (60%). Among Asian countries, Indonesia reported the greatest usage of ACEI/ARB (87%), but the lowest of β-blockers (61%).19
The ESC guidelines not only recommend administration of ARNI/ACEI/ARB, β-blockers, MRA, and SGLT2i, but also highlight the importance of dose up‑titration.7,20 As mentioned above, only 1% of the patients are treated with the target maximum doses for all 4 recommended GDMT drugs.8 It has been proven that therapies at doses equal to or exceeding 50% of the recommended ones are associated with better outcomes.21 However, in real‑life scenarios, it is difficult to reach higher doses due to the frequent occurrence of hypotension, bradycardia, chronic renal disease, and hyperkalemia.8,21,22 In the ASIAN‑HF registry, the recommended maximum doses of ACEI/ARB, β-blockers, and MRA were reached in 17%, 13%, and 29% of patients, respectively,19 which is in line with our results (15.6%, 16%, and 31%, respectively). However, when comparing the proportions of patients achieving at least 50% of the recommended doses, the Polish cohort outperformed the Asian one (35.5% vs 19.8% for RAASis, 36.9% vs 17.1% for β-blockers, and 54.7% vs 21.1% for MRAs). On the other hand, these proportions for the Polish group were lower than those in the ATA study (41.9%, 31.2%, and 87.6% for RAASis, β-blockers, and MRAs, respectively).18 It is worth highlighting that we observed down‑titration of treatment in only a few cases, mostly for β-blockers in HFrEF (9.4%).
Emerging evidence suggests that optimization of GDMT in patients with HF is associated with a reduction in diuretic dosage, aiming to improve clinical outcomes while decreasing dependence on diuretics for volume management. However, in our study, we observed an increased frequency of diuretic use regardless of LVEF.23,24 The study by Matusik et al25 reported the use of RAASis, β-blockers, and MRAs at 83.1%–86.3%, 61.5%–83.3%, and 56.9%–71.6%, respectively, depending on patient age. This 2005 study assessed medication use across all HF types. Our data suggest that current use of β-blockers and MRAs is higher, and RAASi use is comparable, relative to the entire cohort in our study, with notably greater usage observed in the HFrEF subgroup.
Another noteworthy observation is that in our study ARNIs were used more frequently than in that by Carnicelli et al.26 In the context of early sacubitril / valsartan usage, more than 90% of the patients hospitalized for HFrEF were discharged without an ARNI. The authors also reported that the patients discharged without an ARNI were unlikely to receive it later.27
Another study conducted by Rywik et al28 in the Polish population several years before the HEROES registry clearly indicated the influence of GDMT on mortality. The authors reported that optimal dosing of ACEIs was achieved in 69.3% of the survivors vs 51.3% of nonsurvivors (P <0.001) within the HFrEF subgroup. Similarly, an optimal dose of β-blockers was administered to 69.3% of the survivors and 60.2% of the nonsurvivors (P <0.001). Notably, these differences were also observed in the whole HF cohort: 63.9% vs 47.9% for ACEIs and 64.4% vs 56.5% for β-blockers (both P <0.001).28
Our study also ascertained that treatment optimization was carried out not only in the patients with HFrEF but also for other types of HF. This may have been a strategy to optimize the treatment of comorbidities, such as increasing the dose of β-blockers to improve the control of heart rate in atrial fibrillation. As the new guidelines7 recommending the use of SGLT2i in patients with a LVEF greater than 40% were published during the course of our registry, we observed a significant increase in the frequency of their use over this period. This rise in prescription rates reflects rapid clinical adoption of the new recommendations in response to emerging evidence supporting the benefits of SGLT2is across a broad spectrum of HF phenotypes. In contrast to our findings, a study conducted in 202229 reported significantly lower rates of SGLT2i use among patients with HF. A SGLT2i was prescribed in only 19 out of 1081 HFpEF patients (1.8%) and 51 out of 1596 HFrEF patients (3.2%).
Optimizing GDMT in HF remains a crucial strategy for reducing mortality and hospitalizations1,7; however, its implementation in daily clinical practice remains challenging. Achieving optimal dosing requires frequent monitoring of laboratory parameters, adherence to regular follow‑up visits, and is often hindered by economic constraints and sociological factors, including health care resource limitations. The ESC guidelines recommend reaching target doses within 6 weeks,7 a goal that in real‑world settings is frequently unattainable due to practical difficulties associated with such close monitoring. Moreover, there is a growing tendency to consider patients without recent exacerbations as clinically stable, which can lead to neglecting or underestimating the importance of treatment optimization in this subgroup. This gap underscores the need for pragmatic approaches and intensified efforts to promote optimal HF management.
It is important to note that the utilization of ARNIs is significantly influenced by the lack of reimbursement. Similarly, during the period of registry data collection, SGLT2is were not reimbursed for patients with HFpEF, and were reimbursed only for a short time for those with HFrEF. This lack of reimbursement likely impacted the prescription patterns and accessibility of these therapies in clinical practice.
Limitations
The presented results should be interpreted in the context of several limitations. First, due to the observational registry design, some data regarding both admission and in‑hospital characteristics were missing, including LVEF data. Second, the HEROES patients were recruited from selected centers, which affects generalizability of the results. A limitation of this study is the predominance of data from major metropolitan areas, resulting in underrepresentation of eastern Poland despite the initial design aiming for broad geographic coverage. We acknowledge that the analysis was not designed to assess clinical outcomes, such as mortality, and that relevant biomarker data (eg, high‑sensitivity C‑reactive protein, creatinine, bilirubin) were not included due to the registry limitations. Laboratory tests were performed only when clinically indicated during hospitalization, for example, N‑terminal pro–B‑type natriuretic peptide levels were not routinely measured. This is particularly due to the fact that our analysis focused on planned hospitalizations involving clinically stable patients, in whom the need for extensive laboratory diagnostics was limited. Moreover, it should be noted that the primary aim of the analysis was not to evaluate laboratory parameters in relation to the use of GDMT. Another limitation of this study is that the reasons for suboptimal treatment were not evaluated. That was beyond its scope but represents a valuable direction for further research. Other limitations of the HEROES study have been previously reported.10
Conclusions
In the Polish multicenter HEROES registry, over 80% of patients with HFrEF were discharged on the 4‑pillar GDMT. Nevertheless, the attainment of target high‑dose GDMT remains suboptimal. These findings provide new insights into the variability of GDMT implementation at a national level, and underline the need for strategies to improve dosing optimization.
- McDonagh TA, Metra M, Adamo M, et al; ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42: 3599‑3726. | Crossref
- Kasprzak JD, Gorczyca‑Głowacka I, Sobczak‑Kaleta M, et al. Pharmacotherapy of heart failure A.D. 2023. Expert opinion of Working Group on Cardiovascular Pharmacotherapy, Polish Cardiac Society. Kardiol Pol. 2023; 81: 537‑556. | Crossref
- Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nat Rev Cardiol. 2016; 13: 368‑378. | Crossref
- Shah KS, Xu H, Matsouaka RA, et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5‑year outcomes. J Am Coll Cardiol. 2017; 70: 2476‑2486. | Crossref
- Maps of Health Needs. System and Implementation Analysis Database Platform. Epidemiology [in Polish]. https://basiw.mz.gov.pl/mapy‑informacje/mapa‑2022‑2026/analizy/epidemiologia/. Accessed November 27, 2022. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION