Enhancing chronic kidney disease screening through community pharmacists: a systematic review of pharmacist-led strategies
Key words: chronic kidney disease, CKD screening, community setting, patient outcomes, pharmacist-led intervention



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Enhancing chronic kidney disease screening through community pharmacists: a systematic review of pharmacist-led strategies
Introduction: Chronic kidney disease (CKD) affects over 700 million people worldwide, with its prevalence rising steadily each year. Early diagnosis remains challenging due to a lack of awareness of CKD risk factors and the absence of noticeable symptoms in the initial stages. Pharmacists can play a pivotal role in CKD screening and patient education.
Objectives: The primary aim of this systematic review was to identify specific pharmacist‑led interventions in community pharmacy settings that support CKD detection, assess their effectiveness, and evaluate their impact on patient outcomes.
Patients and methods: The review was conducted in accordance with the 2020 PRISMA guidelines and, given the absence of randomized trials, it included nonrandomized controlled trials and observational studies. A comprehensive search was carried out across 3 databases in 2025: PubMed, Embase, and the Cochrane Library.
Results: Nine original clinical research articles met the inclusion criteria. The findings indicated that pharmacist‑led interventions in the community pharmacies are diverse but consistently contribute to early detection of CKD. Moreover, the pharmacists can further help by supporting ongoing CKD management, enhancing collaboration with general practitioners within coordinated care frameworks, and increasing public awareness of the disease.
Conclusions: Pharmacist involvement in CKD screening improves public understanding of CKD risk factors, facilitates earlier initiation of treatment, and contributes to better long‑term patient outcomes.
What's new?
This is the first review focusing on the potential role of pharmacists in the screening of chronic kidney disease (CKD) in community pharmacies. CKD detection can be carried out by pharmacists in various ways, including the use of essential renal parameters and risk stratification. Moreover, the role of pharmacists goes beyond screening and they may also contribute to effective CKD management. The findings highlight the importance of early‑stage CKD detection, which is often asymptomatic, and show a common lack of awareness of CKD risk factors in the general population. Therefore, pharmacists could help improve CKD detection rates and contribute to better long‑term outcomes, leading to enhanced patient quality of life and economic benefits for the health care system.

Introduction
Chronic kidney disease (CKD) is defined as abnormalities in kidney structure or function persisting for more than 3 months, with implications for health. CKD is diagnosed based on at least 1 of 2 criteria documented or inferred for over 3 months: 1) glomerular filtration rate (GFR) below 60 ml/min/1.73 m² or 2) markers of kidney damage, such as albuminuria.1 CKD affects more than 700 million individuals worldwide, and its prevalence is increasing annually.2 This rise is largely due to a lack of awareness of CKD risk factors and the absence of typical symptoms in the early stages, leading to late diagnosis. The most common cause of CKD worldwide is diabetes,1 while hypertension is not only a major complication of the disease but also a key risk factor for its development.1 Patients with CKD have a 10- to 20‑fold higher risk of cardiovascular disease (CVD).3
In Poland, the detection rate of CKD remains low4; however, there are ongoing initiatives that aim to determine its prevalence.5 There are no dedicated programs targeting its early diagnosis.4 Moreover, the long‑term national health policy plan for nephrology for the years 2022–2026 focuses primarily on palliative and hospice care, while preventive measures are largely overlooked.4,6 Early diagnosis of CKD is, however, feasible within coordinated primary care services.4,7 It is noteworthy that certain initiatives aim to raise awareness of CKD and facilitate its early detection in primary care settings. National consultants in nephrology and family medicine, together with the President of the Polish Society of Nephrology, have issued national guidelines on the diagnosis and management of CKD in primary care, with an emphasis on coordinated care models.8 However, pharmacists are currently not engaged in these activities.
Pharmacists can play a crucial role in CKD screening and patient education. The International Pharmaceutical Federation (FIP) has introduced the CKD pharmacy toolkit to help pharmacists identify at‑risk patients and provide motivational counseling to encourage CKD screening.1 Its primary goal is to increase the number of undiagnosed at‑risk patients referred for CKD screening, thereby facilitating earlier diagnosis and management. CKD prevention and management involve setting and achieving therapeutic goals, identifying the need for nephroprotective therapy (eg, angiotensin‑converting enzyme inhibitors [ACEIs], sodium‑glucose cotransporter‑2 inhibitors [SGLT2is], or finerenone), and ensuring appropriate monitoring.1 Medication reviews provide an opportunity to identify and discontinue nephrotoxic medications and adjust dosages as needed.1 Slowing CKD progression in its early stages could yield economic benefits and, most importantly, prevent kidney failure and cardiovascular complications.1 Notably, cardiovascular mortality is one of the leading causes of death among CKD patients.1
This study systematically reviewed and discussed findings from original research investigating the role of pharmacists in CKD screening in community pharmacies. It aimed to find out if there are any scientific reports on pharmacist‑led interventions in community setting that facilitate CKD detection, and if so, what specific types of interventions are implemented, how effective they are in CKD screening, and how they contribute to improved patient outcomes.
Patients and methods
This systematic review was conducted in accordance with the 2020 PRISMA guidelines.9 Eligible publications included full‑text articles in English or Polish describing pilot programs, pharmaceutical care interventions, or educational activities that assessed the role of pharmacists in detecting CKD.
Exclusion criteria comprised conference abstracts, guidelines or expert statements, opinion papers, preprints, and publications that did not report outcomes of pharmacist‑led interventions.
A comprehensive search was performed across 3 databases—PubMed, Embase, and the Cochrane Library—on March 17 and March 21, 2025. The final search update was conducted on July 4, 2025.
A majority of the included studies were observational ones; 1 study was a subanalysis of a randomized controlled trial, but all other studies were nonrandomized. The inclusion criteria were defined using the PICO (Population, Intervention, Comparison, Outcome) framework. The studies only included adults without a formal diagnosis of CKD, and must have investigated pharmacist‑led activities (eg, medication review, screening, patient counseling, laboratory test referral) aimed at detecting CKD. They had to compare standard pharmacist practice / usual pharmacy care (without targeted CKD detection activities), and their outcome had to be the detection of CKD based on eGFR or albumin‑to‑creatinine ratio (ACR), identification of albuminuria, classification of patients as having a moderate or high CKD risk according to the QKidney algorithm, or CKD diagnosis confirmed through pharmacist‑facilitated consultation of renal function parameter with a general practitioner (GP).
The following search query was used: “(CKD OR chronic kidney disease OR renal insufficiency OR kidney insufficiency) AND (detection OR screening OR identification) AND (community pharmacy OR pharmacist).”
A comprehensive search strategy was developed to identify relevant studies. Various combinations of key words were used to ensure a wide range of studies were captured (Supplementary material, Tables S1–S3).
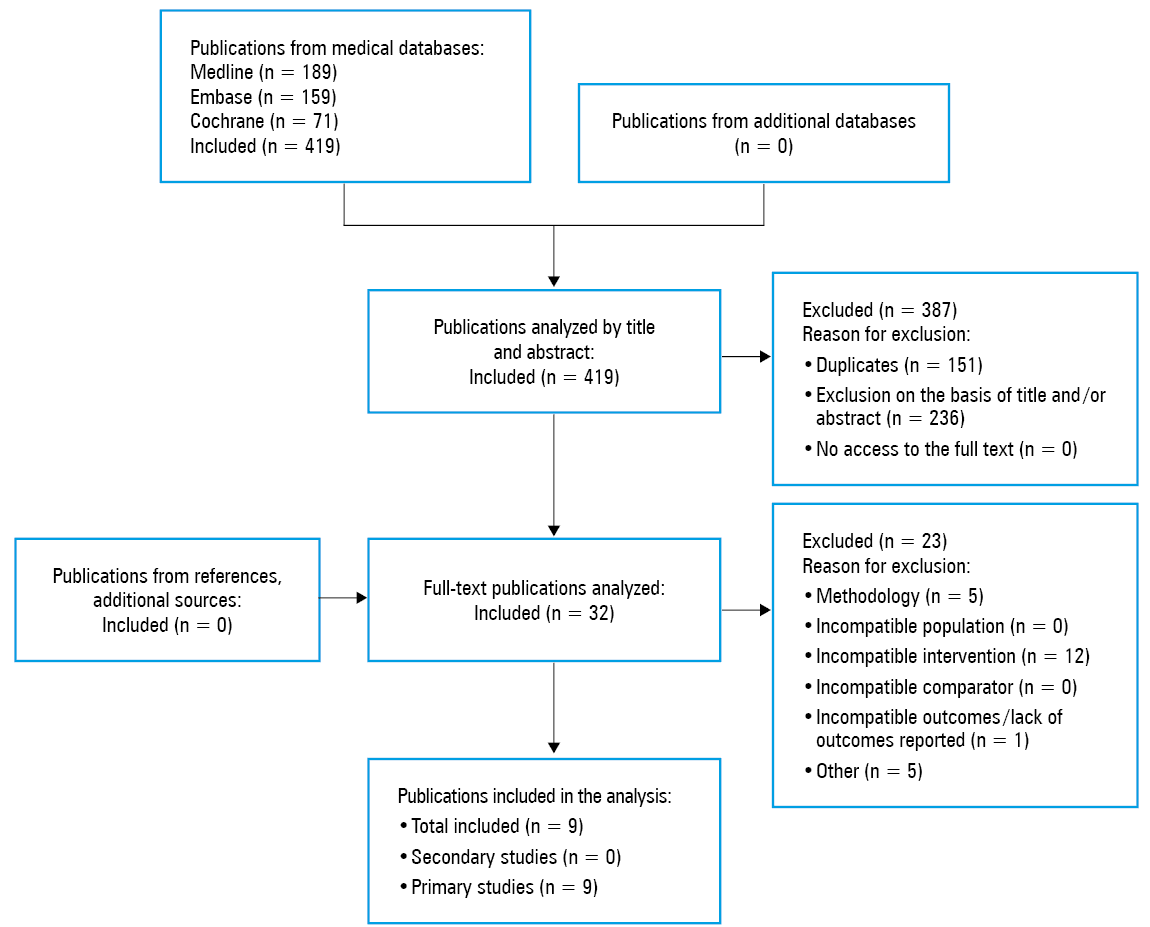
This yielded a total of 419 records. The records were imported into Rayyan platform (Rayyan Systems, Inc. Cambridge, Massachussets, United States) for screening.
After removing 160 duplicates, 259 titles and abstracts were independently screened by 2 researchers (AO and MR). Any discrepancies were resolved through discussion, with the involvement of a third reviewer (AD). This process yielded 32 records that initially met the inclusion and exclusion criteria. Full texts of these 32 articles were retrieved and assessed for eligibility.
Ultimately, 23 studies were excluded: 12 because the population or intervention did not meet the PICO criteria, 5 due to publication type (eg, research letters rather than full‑text original articles), 4 because they were not in English or Polish, and 1 due to a lack of reported outcomes. One duplicate was also removed. As a result, 9 original clinical research articles were included in the final review. Figure 1 summarizes the flow diagram of the study selection process.
Data extracted from each study included study design, population characteristics, description of the pharmacist‑led intervention, reported risk factors for CKD among participants, and primary outcomes.
Risk of bias was assessed using the ROBINS‑I tool, version 2 for nonrandomized studies, evaluating 7 domains: confounding, participant selection, classification of interventions, deviations from intended interventions, missing data, outcome measurement, and selective reporting.10 Each domain was rated as having low, moderate, serious, or critical risk of bias.10 The study did not require approval from an institutional review board or ethics committee.
Statistical analysis
The statistical analysis was not performed for this systematic review.
Results
In Tables 1 and 2 we summarize the pharmacist‑led interventions for CKD detection in patients with common risk factors, such as diabetes and hypertension. Frequently reported risk factors included hypertension, diabetes, age, vascular disease, obesity, smoking, and family history of CKD.
Study | Hypertension | Diabetes | Age | Vascular disease | Family history | Obesity | Smoking | Additional risk factors |
Abbreviations: CVD, cardiovascular disease; HbA1c, glycated hemoglobin; LDL‑C, low‑density lipoprotein cholesterol; NHS, National Health Service; NSAID, nonsteroidal anti‑inflammatory drug; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; UTI, urinary tract infection | ||||||||
Jairoun et al13 | X | X | X | X | – | – | – | Male sex |
Donovan et al15 | X | X | X | X | – | – | – | SLE, RA, Framingham >20%, LDL‑C, HbA1c |
Al Hamarneh et al17 | X | X | X | X | X | – | – | Sex, anemia, CVD history |
DePatis et al11 | X | X | X | X | – | – | – | Ethnic background, stroke history |
Papastergiou et al14 | X | X | X | X | X | – | – | Ethnicity (Aboriginal, etc.) |
Gheewala et al12 | X | X | X | X | X | X | X | Not specified |
Srimongkhol et al16 | X | X | X | X | X | – | – | Systemic infections (eg, pyelonephritis, endocarditis), recurrent UTIs, gout, high uric acid, NSAIDs, nephrotoxicity, kidney / urinary stones |
Yonel et al36 | – | – | X | – | – | – | – | Treatment via NHS services |
Vu et al18 | X | X | – | – | – | – | X | NSAID use |
Study and country | Setting | Study design | Risk of bias | Population | Method of screening | Study duration | Primary outcomes | Effect size on primary outcomes | Confirmation of CKD diagnosis after 3 months |
Abbreviations: ACR, albumin‑to‑creatinine ratio; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; GP, general practitioner; SCORED, Screening for Occult Renal Disease; others, see Table 1 | |||||||||
Jairoun et al,13 United Arab Emirates | Community pharmacies | Quantitative observational | Serious | n = 400 (mean age, 69 y; 57% women) with hypertension (86.5%), CVD (45%), or diabetes mellitus (32.3%) | Venous blood sample via fingerstick; PICCOLO device | 1 month | Effectiveness and risk factor identification | 38.8% of the patients with previously undiagnosed CKD; higher rate identification in older, hypertensive, and diabetic patients | – |
DePatis et al,11 United States | Community health center | Quantitative observational | Serious – critical | n = 30 (mean age, 60.8 y; 70% women) with hypertension (93%), CVD (13%), or heart failure (13%) | SCORED tool + education + urine dipstick | 4 months | Urinary albumin testing | 54% positive results for proteinuria | – |
Donovan et al,15 Canada | Community pharmacy | Quantitative observational | Serious | n = 89 (mean age, 67 y; 62.9% women) with hypertension (77.5%), CVD (33.7%), or tobacco use (46.1%) | StatSensor PoCT | 6 weeks | Recruitment and undiagnosed CKD | Recruitment rate: 59 participants per month; 90% with previously undiagnosed CKD | – |
Gheewala et al,12 Australia | Community pharmacies | Quantitative observational | Moderate | n = 389 (mean age, 63.3 y; 50.4% women) with hypertension (81.2%), diabetes mellitus (21.9%), or prior cardiovascular event (15.9%) | QKidney calculator | 1 year | Risk estimation and GP referral | Participant classification as: 33.4% moderate risk 1 (3%–7.9%); 11.6% moderate risk 2 (8%–15%); 7.2% high risk (>15%); 95.2% visited GP | X |
Papastergiou et al,4 Canada | Community pharmacy | Quantitative observational | Serious | n = 642 (mean age, 60 y; 55% women) with CKD risk factors—ethnic minority (80%), age >55 y (67%), or hypertension (45%) | HealthTab + PICCOLO | 6 months | CKD prevalence and risk factors | 11.5% identified at stage 3 CKD; 3 individuals with eGFR 15–29 ml/min/1.73 m2; 77% of the patients previously unaware of kidney condition | – |
Al Hamarneh,7 Canada | Community pharmacies | Randomized controlled trial | Serious | n = 720 (mean age, 63 y; 43% women) with diabetes mellitus (79%), CVD (30%), or tobacco use (27%) | RxEACH pathway: creatinine, eGFR, ACR | Not reported | Undiagnosed CKD | 40% newly diagnosed CKD | X |
Srimongkhol et al,16 Thailand | Community pharmacies | Quantitative observational | Serious | n = 521 (mean age, 54.8 y; 68.7% women) exposed to NSAIDs / nephrotoxins (46.3%), hypertension (25.9%), or age >60 y (25.3%) | Education + urine dipstick for microalbumin; Beckman Coulter LX20 PRO analyzer (modified Jaffe method for serum creatinine) | 12 weeks | Albuminuria before and after pharmacist counselling | Week 0: 57% positive results for albuminuria; week 12 (postcounselling): 32% still positive, 68% negative | X |
Yonel et al,36 United Kingdom | Community pharmacy | Quantitative observational | Serious | n = 51 (mean age, 65 y; 53% women) with CVD family history (63%), overweight (47%), or CVD (45%) | Finger‑prick blood sample for eGFR (Nova StatSensor) | Single visit | eGFR distribution | 1 known CKD case; 16 with eGFR >90 ml/min/1.73 m2, 19 participants with eGFR 60–89 ml/min/1.73 m2, 6 with eGFR 49–55 ml/min/1.73 m2 | – |
Vu A et al,18 United States | Primary care clinics | Quantitative observational | Serious | n = 20 (mean age, 63 y; 55% women) with hypertension (90%), diabetes mellitus (50%), or chronic NSAID use (15%) | Education, follow‑up eGFR testing | 9 months (February–October 2021) | CKD recognition based on eGFR trends and ACR screening | 4 patients with confirmed CKD stage 3a (≥2 with eGFR <60 ml/min/1.73 m2 over 3 months); 4 suspected CKD cases; 2 with moderate albuminuria (ACR, 30–300 mg/g) | X |
Primary outcomes included detection of undiagnosed CKD and proteinuria; secondary outcomes were identification of individuals at an increased 5‑year CKD risk and follow‑up rates with GPs.
All studies demonstrated feasibility of pharmacist‑led CKD screening. Interventions typically recruited high‑risk patients during pharmacy visits or by using dedicated tools, such as the SCORED (Screening for Occult Renal Disease) questionnaire11 and QKidney calculator.12 The patients scoring 4 or higher on SCORED questionnaire were classified as high‑risk and offered education alongside the urine dipstick test to assess the ACR.11 The patients with a 5‑year risk equal to or above 3%, as determined by the QKidney calculator, received personalized letters addressed to their physicians, and all of them were followed‑up by telephone after 9 months.12 The screening procedures included eGFR and / or albuminuria testing, using devices such as PICCOLO13,14 (a validated point‑of‑care tool; Zoetis Inc, Parsippany, New Jersey, United States), StatSensor15 (a blood chemistry analyzer for venous blood testing to assess creatinine levels and estimate GFR; Nova Biomedical, Waltham, Massachussets, United States), or the urine dipstick test.11,16 The patients with positive urine dipstick test results for albuminuria underwent confirmatory laboratory testing, and were then referred to a primary care unit for further evaluation.
In another intervention, Al Hamarneh et al17 reported a screening process embedded within the RxEACH (The Alberta Vascular Risk Reduction Community Pharmacy Project) study. The pharmacists identified eligible patients based on recent laboratory data and medication history—specifically prescriptions for antihypertensives or hypoglycemics. If the required laboratory tests had not been completed within the previous 12 months, the pharmacists ordered them as part of the intervention. This pharmacist‑led screening not only contributed to improved renal outcomes but also significantly enhanced patient awareness of CKD prevention. In a study by Srimongkhol et al,16 mean (SD) self‑awareness score regarding CKD increased from 6.43 (2.34) to 8.06 (1.06) following pharmacist‑delivered education. Similarly, Vu et al18 concluded that general knowledge about kidney health improved, as 95% of the participants reported moderate or high confidence in interpreting their kidney test results after receiving education from a pharmacist.
Risk of bias
Risk of bias was assessed using the ROBINS‑I tool for nonrandomized studies10 (Supplementary material, Table S4). Al Hamarneh et al17 was initially considered for the RoB2 tool19 but reassessed with ROBINS‑I, as the patients were not randomized. Most studies showed a serious risk of bias, underlining the need for higher‑quality research.
Proposal of the algorithm for the community pharmacists
Based on the conducted systematic review, we propose an algorithm for community pharmacists to identify individuals with undiagnosed CKD (Supplementary material, Figure S1).
The algorithm was developed according to an evidence‑informed consensus approach, based on the findings of a systematic review, the framework proposed by FIP,3 the Kidney Disease: Improving Global Outcomes guidelines,1 and the recommendations of the Polish Society of Family Medicine.8 The development of the algorithm was guided by the principles of guideline adaptation (ADAPTE framework)20 and by the general assumptions of the Medical Research Council framework for developing and evaluating complex health care interventions.21 Due to the nature of the identified studies (mainly observational and nonrandomized), formal quality assessment using the GRADE approach22 was not applied. The final structure of the algorithm was agreed upon through team discussion, in a manner resembling expert consensus techniques23 (eg, Delphi, nominal group technique), to ensure consistency and practical applicability of the algorithm.
Discussion
The review identified a limited number of studies addressing the detection of CKD by pharmacists. None of the identified publications were available in Polish or examined the Polish health care context.
Despite heterogeneity of the studies, common features included targeting high‑risk populations and using point‑of‑care technologies. Early CKD detection improves disease control, reduces complications, delays progression, and enhances outcomes.24-26 Pharmacists can further optimize care by adjusting drug doses and avoiding nephrotoxic medications.27,28
Types of interventions
Patient recruitment often occurs during pharmacy visits or through tools such as the SCORED questionnaire11 and QKidney calculator,12,29 which improve risk stratification and referrals.12 eGFR and albuminuria testing remain central, with devices such as PICCOLO13,14 and StatSensor15 enabling rapid assessments. For the pharmacists without access to such equipment, an alternative approach is to review laboratory results from the previous 12 months or, if necessary, order appropriate tests.17 Urine dipsticks provide quick albuminuria screening, but positive results warrant confirmatory ACR testing.30,31
Many patients remain unaware of the significance of eGFR or ACR values, or even that their previous results were abnormal. Importantly, ACR may represent the earliest detectable abnormality in renal function.31 Therefore, urine dipstick testing can serve as a practical first step for a rapid qualitative assessment of albuminuria. If the result is positive, laboratory‑based quantitative ACR testing is warranted. Given the strong prognostic value of elevated ACR, expanding its use in pharmacy‑based screenings may significantly improve early CKD detection rates.30,31
A key pharmacist‑led intervention—closely linked to community‑based CKD screening—is the delivery of multicomponent education. This typically includes information on CKD risk factors, the importance of laboratory assessments of renal function, and guidance on interpreting test results. Such educational activities are essential for empowering patients to understand and actively manage their kidney health.16,18
Effectiveness of screening
Pharmacist‑led screening consistently detects previously undiagnosed CKD, with some studies reporting detection in as many as 40% of the participants.13,15,17 It also increases follow‑up rates with a GP after abnormal screening results.12,14,16 Such interventions enhance patient self‑awareness and encourage behaviors that can slow down disease progression.16,18 Pharmacists help to bridge the gaps in CKD awareness, particularly in settings where routine kidney monitoring is lacking.24,25 Their involvement enables identification of the individuals who should already have been aware of their CKD risk or were already exhibiting clinical indicators of the disease.
Clinical impact and future directions
Early detection facilitates nephroprotective treatment and the management of CKD‑related comorbidities, such as diabetes and hypertension, thereby reducing disease progression, cardiovascular events, and the need for dialysis.26 The role of a pharmacist covers medication optimization,24,25,27 improving patient outcomes, and lowering health care costs. As accessible health care professionals, pharmacists are well‑positioned to support ongoing CKD management, including adjusting drug dosages based on renal function and identifying potentially nephrotoxic medications.24,25,27,28
With their comprehensive approach to patient care, pharmacists can also contribute to holistic treatment strategies. This includes counseling on the most appropriate pharmacological options, particularly for patients with multiple risk factors—not only renal, but also cardiovascular.32 In addition, through multicomponent educational activities, pharmacists can increase patient knowledge of nonpharmacological foundations of a healthy lifestyle that are essential for kidney health, such as reducing dietary salt intake.33
The pharmacist‑led screening interventions open new pathways for interprofessional collaboration.34,35 The patients identified as being at a high risk of CKD, or presenting with abnormal screening results, can be referred directly to their GPs. This approach accelerates diagnostic processes, enables timely initiation of treatment for CKD and related comorbidities, and may reduce long‑term economic burden on health care systems. More broadly, these findings underscore the value of integrating pharmacists into coordinated health care models to improve chronic disease management.35
Conclusions
This systematic review indicates that involving pharmacists in CKD screening represents a valuable opportunity to raise public awareness of CKD risk factors. The pharmacist‑managed screening programs support early identification of CKD—often in patients with abnormal laboratory results who are unaware of their clinical significance. Pharmacist contributions to CKD care can be multidimensional, extending from education and screening to long‑term management. These interventions have the potential to improve patient outcomes and contribute meaningfully to the development of more integrated and effective coordinated care systems.
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024; 105: S117‑S314. | Crossref
- Francis A, Harhay MN, Ong ACM, et al. Chronic kidney disease and the global public health agenda: an international consensus. Nat Rev Nephrol. 2024; 20: 473‑485. | Crossref
- International Pharmaceutical Federation. Chronic kidney disease pharmacy toolkit. 2025. https://www.fip.org/files/content/publications/2023/2023‑05‑17_Pharmacy_Toolkit_How_To_Guide.pdf. Accessed August 26, 2025.
- Supreme audit office, report on audit findings: diagnostics and provision of care for patients with chronic kidney disease [in Polish]. https://www.nik.gov.pl/plik/id,31243,vp,34339.pdf. Accessed August 26, 2025.
- Jazienicka A, Babicki M, Krajewska M, et al. A nationwide epidemiological study of chronic kidney disease prevalence in a high‑risk patient population without prior diagnosis in primary health care in Poland. J Clin Med. 2025; 14: 3600. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION