Persistent SARS-CoV-2 infection mimicking interstitial lung disease in an immunocompromised patient



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Persistent SARS-CoV-2 infection mimicking interstitial lung disease in an immunocompromised patient
We present a case of a 72‑year‑old woman admitted to a pulmonology department due to nonspecific interstitial lung lesions. Her medical history included high‑grade follicular lymphoma (G3A), treated with 6 cycles of chemotherapy combined with anti‑CD20 monoclonal antibody, obinutuzumab, followed by maintenance therapy with obinutuzumab.
In January 2022, during maintenance therapy, she developed a mild SARS‑CoV‑2 infection presenting with fever, headache, and dry cough. The diagnosis was confirmed by an anterior nasal swab rapid antigen test.
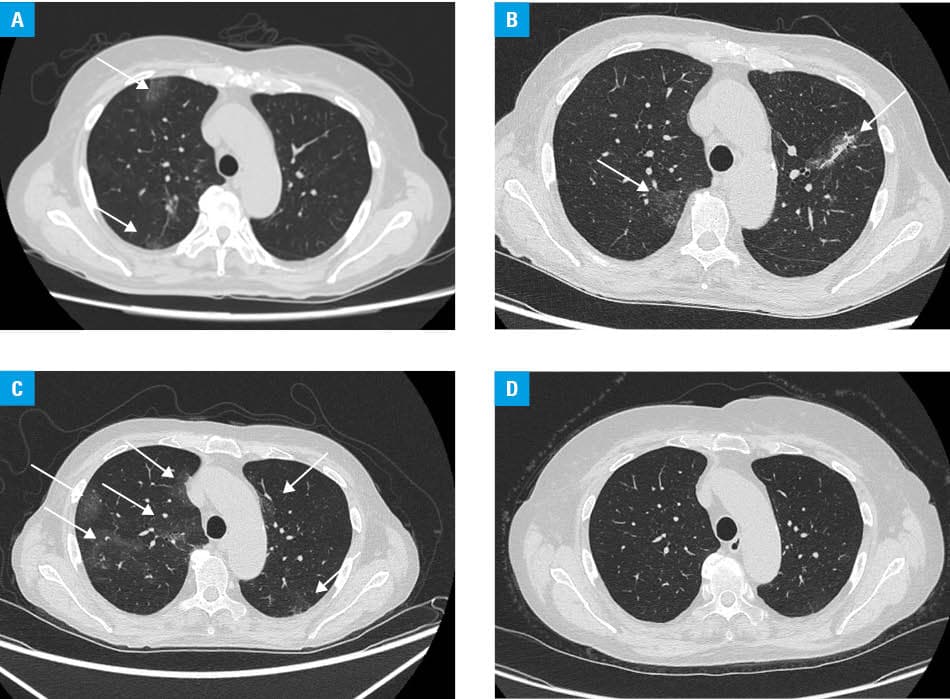
In July 2022, as part of routine lymphoma follow‑up, the patient underwent high‑resolution computed tomography (HRCT) of the chest, which showed interstitial lung lesions bilaterally affecting about 10% of the lungs (Figure 1A). She received empirical antibiotic treatment.
Approximately 6 months later, the patient was readmitted with persistent dry cough and general malaise. Physical examination showed bilateral basal crackles. Laboratory test results indicated mild anemia (hemoglobin, 9.9 g/dl; reference range [RR], 12–16 g/dl], eosinopenia (eosinophils, 0.01 × 103/µl; RR, 0.05–0.5 × 103/µl], and an elevated C‑reactive protein level (CRP; 59.8 mg/l; RR <5 mg/l). Autoimmune markers (rheumatoid factor, anti‑cyclic citrullinated peptide, antinuclear antibodies, and antineutrophil cytoplasmic antibodies) were negative. On bronchoscopy, respiratory samples for respiratory viruses, atypical bacteria, Pneumocystis jirovecii, and bacterial cultures were obtained, with test results being negative.
Repeat HRCT demonstrated bilateral, migratory ground‑glass opacities in a different location than previously (Figure 1B). Pulmonary function test results were normal, except for reduced diffusing capacity for carbon monoxide (DLCO) of 49% of the value predicted. Bronchofiberoscopy was performed. Bronchoalveolar lavage fluid (BALF) cultures and polymerase chain reaction (PCR) assays for bacterial, viral, and fungal pathogens were negative. BALF cytology showed lymphocyte predominance (71%) without eosinophils. BALF for SARS‑CoV‑2 was not performed. Based on HRCT imaging, drug‑induced interstitial lung disease (DI‑ILD) was suspected, and methylprednisolone was initiated (32 mg/day; approximately 0.5 mg/kg/d) and tapered.
In May 2023, during steroid dose reduction, HRCT demonstrated worsening ground‑glass opacities (Figure 1C), DLCO declined further to 34% of the value predicted, and the 6‑minute walk test showed oxygen desaturation. Repeat bronchofiberoscopy included BALF sampling for SARS‑CoV‑2 PCR and lymphocyte immunophenotyping. BALF showed a predominance of CD3+ T cells (85.24%), excluding lymphoma relapse. SARS‑CoV‑2 PCR was positive in BALF despite negative nasopharyngeal PCR and antigen tests. Serology confirmed absence of anti‑SARS‑CoV‑2 antibodies, consistent with B‑cell depletion due to obinutuzumab therapy.
Given these findings and limited available literature, treatment with nirmatrelvir and ritonavir was initiated.1,2 Methylprednisolone was reintroduced at 32 mg/d and tapered over several months. Clinical improvement was observed. CRP and hemoglobin levels normalized. In October 2023, HRCT showed significant lesion regression, and DLCO improved to 47% of the value predicted (Figure 1D). One‑year follow‑up demonstrated near complete regression of interstitial changes, and DLCO increased to 53% of the value predicted.
This case illustrates an atypical presentation of SARS‑CoV‑2 in an immunocompromised patient with B‑cell depletion, highlighting the need to consider persistent infection. In differential diagnosis, other opportunistic viral infections, such as cytomegalovirus, Epstein–Barr virus, or HIV, should be excluded. Evidence supporting antiviral therapy against SARS‑CoV‑2 remains limited.1,2 Belkin et al3 reported persistent inflammatory seronegative COVID‑19 with fever, elevated CRP, pulmonary involvement, and absent antibodies due to B‑cell depletion. Our case emphasizes the importance of sampling site—only lower respiratory tract reverse‑transcription PCR confirmed infection.4 Even though BALF PCR confirmed only the presence of viral RNA, which does not prove active replication, this cannot be fully confirmed in clinical settings, without sequencing or longitudinal viral load data. Nevertheless, antiviral therapy proved efficient in the current case.
Prolonged SARS‑CoV‑2 infection should be considered in patients receiving B‑cell depleting therapy. Moreover, lymphomas themselves contribute to immunosuppression and are linked to a higher risk of long‑lasting or atypical COVID‑19 manifestations.5 SARS‑CoV‑2 infection can mimic other causes of bilateral ground‑glass opacities, including DI‑ILD, requiring careful diagnostic evaluation.
- Faxén L, Edvinsson M. Persistent SARS‑CoV‑2 infection in patients with B‑cell deficiency: a case series of successful antiviral treatment of four patients. Ups J Med Sci. 2023; 128: e9807. | Crossref
- Jung S, Yagi Y, Fukushima K, et al. Successful dual antiviral therapy with remdesivir and ensitrelvir in a case of prolonged COVID‑19 following B‑cell depleting immunotherapy for malignant lymphoma. IDCases. 2023; 34: e01890. | Crossref
- Belkin A, Leibowitz A, Shargian L, Yahav D. The unique presentation of SARS‑CoV‑2 Infection in patients with B‑cell depletion: definition of ‘persistent inflammatory sero‑negative COVID’. Clin Microbiol Infect. 2023; 29: 1‑3. | Crossref
- Ramos KJ, Kapnadak SG, Collins BF, et al. Detection of SARS‑CoV‑2 by bronchoscopy after negative nasopharyngeal testing: stay vigilant for COVID‑19. Respir Med Case Rep. 2020; 30: 101120. | Crossref
- Kosmaczewska A, Frydecka I. Dysregulation of the immune system as a driver of the critical course of novel coronavirus disease 2019. Pol Arch Intern Med. 2020; 130: 779‑788. | Crossref
ARTICLE INFORMATION